

Relationship Between Myocardial Bridges and Arrhythmic Complications
ABSTRACT: Myocardial bridge (MB) is defined as compression of coronary artery during systole while it is normal in diastole. In angiographic series, the prevalence of this anomaly was reported between 0.5% and 2.5%. It is occasionally seen in the middle segment of the left anterior descending coronary artery. Although MB is considered to be a benign anomaly, the association of MB with ischemia, systolic dysfunction, conduction abnormality, arrhythmias, and sudden cardiac death were reported. Herein, we report 3 cases of MB that were diagnosed with coronary angiography and were associated with arrhythmic complications. In 2 patients, complete atrioventricular block was present, and another patient was diagnosed with sick sinus syndrome with the help of an electrophysiological study. All patients underwent permanent cardiac pacemaker implantation.
J INVASIVE CARDIOL 2012;24(11):E300-E302
_________________________________________________________________
 Case Report 1. A 51-year-old woman was admitted to the cardiology clinic because of loss of consciousness. She had no previous history of disease. She described presyncope occurring approximately 1 year prior. The present syncope lasted 1-2 minutes and there were no epileptic attacks or incontinence. Physical examination on admission was unremarkable. Blood pressure levels were also normal. Twelve-lead electrocardiogram revealed sinus bradycardia (32 bpm) (Figure 1). After 1 mg of atropine, heart rate quickened (136 bpm). Transthoracic echocardiography revealed normal systolic and diastolic functions. We performed 24 hour Holter monitoring which demonstrated tachycardia-bradycardia attacks. In addition, there were sinus pauses lasting more than 3 seconds during daily Holter monitoring. Because of suspicion of sick sinus syndrome, we performed an electrophysiology study. Sinus node dysfunction was detected. We also performed coronary angiography because of intermittent chest pains and there
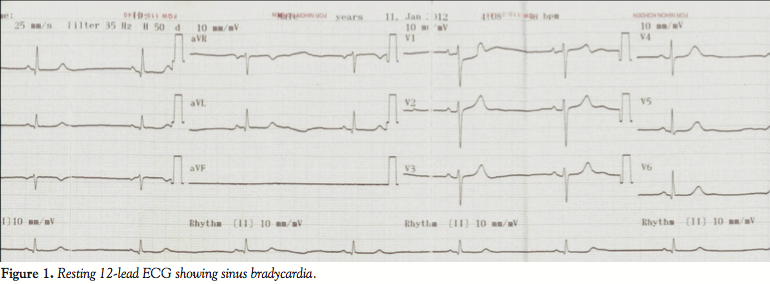
Case Report 1. A 51-year-old woman was admitted to the cardiology clinic because of loss of consciousness. She had no previous history of disease. She described presyncope occurring approximately 1 year prior. The present syncope lasted 1-2 minutes and there were no epileptic attacks or incontinence. Physical examination on admission was unremarkable. Blood pressure levels were also normal. Twelve-lead electrocardiogram revealed sinus bradycardia (32 bpm) (Figure 1). After 1 mg of atropine, heart rate quickened (136 bpm). Transthoracic echocardiography revealed normal systolic and diastolic functions. We performed 24 hour Holter monitoring which demonstrated tachycardia-bradycardia attacks. In addition, there were sinus pauses lasting more than 3 seconds during daily Holter monitoring. Because of suspicion of sick sinus syndrome, we performed an electrophysiology study. Sinus node dysfunction was detected. We also performed coronary angiography because of intermittent chest pains and there 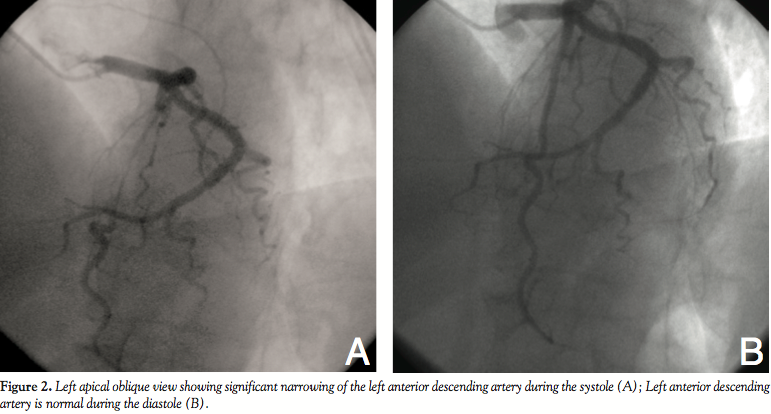 were no significant lesions. Only myocardial bridge (MB) in the left ascending coronary artery (LAD) causing significant stenosis was demonstrated (Figures 2A and 2B). A permanent pacemaker (dual-chamber) was implanted because of symptomatic sinus bradycardia. She was discharged on the fifth day of admission.
were no significant lesions. Only myocardial bridge (MB) in the left ascending coronary artery (LAD) causing significant stenosis was demonstrated (Figures 2A and 2B). A permanent pacemaker (dual-chamber) was implanted because of symptomatic sinus bradycardia. She was discharged on the fifth day of admission.
Case Report 2. A-72-year-old man was admitted to the emergency department because of syncope attack. Admission 12-lead ECG revealed third-degree atrioventricular (AV) block (Figure 3). The patient was hemodynamically stable. Bedside echocardiography was normal (ejection fraction, 68%). The patient was hospitalized in the cardiology clinic. After detailed examinations, we performed coronary angiography to explain complete AV block. Coronary 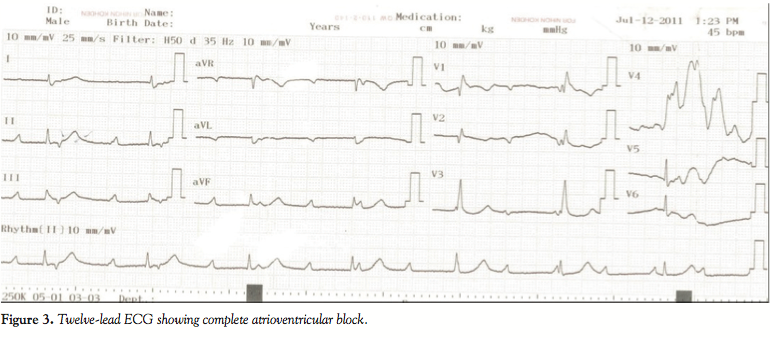 angiography revealed MB causing severe stenosis (80%) in the LAD. There were no significant lesions in the coronary arteries. A permanent pacemaker with ventricular demand rate responsive mode was implanted. The patient was discharged on the sixth day of admission.
angiography revealed MB causing severe stenosis (80%) in the LAD. There were no significant lesions in the coronary arteries. A permanent pacemaker with ventricular demand rate responsive mode was implanted. The patient was discharged on the sixth day of admission.
Case Report 3. A-59-year-old man presented to the emergency department because of dizziness lasting for 3 months. He had previous history of hypertension and dyslipidemia. He was on amlodipine (5 mg/day) and atorvastatin (10 mg/day) treatments. On physical examination, the patient’s pulse was regular with 42 bpm. Twelve-lead resting ECG showed complete AV block. Echocardiography did not reveal systolic or diastolic dysfunction. Admission cardiac biomarkers were within normal limits. Coronary angiography was performed and revealed MB causing severe stenosis (70%) in the LAD artery (Figures 4A and 4B). Permanent pacemaker implantation with DDDR mode was implanted. The patient was discharged within 4 days of admission.
within 4 days of admission.
Discussion. MB occurs when epicardial coronary artery tunnels through the myocardium. It was first described as a congenital anomaly by Granicia in 1922 and in 1960, Portman angiographically demonstrated occlusion of the coronary arteries in the systole. MB is most commonly localized in the middle segment of the LAD.1 Although the prevalence of MB ranged between 15% and 85% in necropsy studies, the frequency was found low (0.5%-2.5%) in angiographic studies.2,3 MB as a benign structure was associated with ischemia, infarctus, systolic dysfunction, conduction abnormalities, arrhythmias, and sudden cardiac death.4 Though pathophysiology of MB is still unknown, the main factors were attributed to the grade of systolic compression, heart rate, and diastolic filling duration.1 While asymptomatic patients do not require any treatment, patients with angina need to be treated with initial medical treatment such as beta-blockers, calcium-channel blockers, and alternative treatment options such as surgical myotomy, coronary stenting, and bypass operation.5
It is well known that coronary arteries are supplied with blood flow in diastole. However, myocardial perfusion via coronary arteries is damaged in systole in patients with MB. This problem was related to consistent mechanical stress due to myocardial segment, coronary vasospasm in response to endothelial injury, and premature atherosclerosis.6 Nevertheless, intravascular ultrasound studies showed that coronary compression is also proceeding during diastole.7 Effective vasodilators and nitrates were tried to solve vasospasm, but they worsened symptoms as a cause of enhanced systolic coronary compression. Several arrhythmic complications were reported in patients with MB: paroxysmal AV block,8 ventricular tachycardia,9,10 and sudden cardiac death.11,12 Paroxysmal AV block was induced by exercise in an otherwise healthy young man and was related to MB.8 Afterwards, autopsies of younger patients with sudden cardiac death showed increased prevalence of MB.13 In another case, severe hypotension and complete AV block in a 74-year-old patient was associated with MB.14 The pathophysiology of sudden cardiac death still remains unknown. Within 2 months, 2 patients presented with complete AV block and were angiographically diagnosed with MB. Interestingly, another patient with syncope was diagnosed with sick sinus syndrome and coronary angiography revealed MB. Although MB was mentioned in the etiology of complete AV block, there is no knowledge about the causative role of MB in the etiology of sick sinus syndrome. We postulated that MB related ischemia like an ischemia in a consequence of atherosclerotic process might cause AV block. Though the relationship of MB with arrhythmic events and ischemia was reported in small studies or case reports, there are no large and randomized studies in this field. Our aim is to raise awareness of MB and relevant arrhythmic events like complete AV block and sick sinus syndrome. The main question is why the arrhythmias didn’t appear until later in the patients’ lives because MB is something that the patients were born with and this has yet to be answered.
References
- Angelini P, Trivellato M, Donis J, Leachman RD. Myocardial bridges: A review. Prog Cardiovasc Dis. 1983;26(1):75-88.
- Hillman ND, Mavroudis C, Backer CL, Duffy CE. Supraarteriel decompression myotomy for myocardial bridging in a child. Ann Thoracic Surg. 1999;68(1):244-246.
- Kurtoğlu N, Ermeydan C, Akdemir R, et al. Koroner Miyokardiyal Bridge Sıklığının 12279 Anjiografi Vakasında Değerlendirilmesi; Cinsiyet Bir Faktörmü? Türk Girişim Kard Der. 1999;3:134-137.
- Möhlenkamp S, Hort W, Ge J, Erbel R. Update on myocardial bridging. Circulation. 2002;106(20):2616-2622.
- Ng E, Jilaihawi H, Gershlick AH. Symptomatic myocardial bridging--a niche indication for drug-eluting stents? Int J Cardiol. 2005;99(3);463-464.
- Tio RA, Ebels T. Ventricular septal rupture caused by myocardial bridging. Ann Thorac Surg. 2001;72(4):1369-1370.
- Hakeem A, Cilingiroglu M, Leesar MA. Hemodynamic and intravascular ultrasound assessment of myocardial bridging: fractional flow reserve paradox with dobutamine versus adenosine. Catheter Cardiovasc Interv. 2010;75(2):229-236.
- den Dulk K, Brugada P, Braat S, Heddle B, Wellens HJ. Myocardial bridging as a cause of paroxysmal atrioventricular block. J Am Coll Cardiol. 1983;1(3):965-969.
- Kracoff OH, Ovsyshcher I, Gueron M. Malignant course of a benign anomaly: myocardial bridging. Chest. 1987;92(6):1113-1115.
- Feld H, Guadanino V, Hollander G, Greengart A, Lichstein E, Shani J. Exercise-induced ventricular tachycardia in association with a myocardial bridge. Chest. 1991;99(5):1295-1296.
- Desseigne P, Tabib A, Loire R. Myocardial bridging on the left anterior descending coronary artery and sudden death. Apropos of 19 cases with autopsy. [In French.] Arch Mal Coeur Vaiss. 1991 Apr;84(4):511-516.
- Cutler D, Wallace JM. Myocardial bridging in a young patient with sudden death. Clin Cardiol. 1997;20(6):581-583.
- Sunnassee A, Shaohua Z, Liang R, Liang L. Unexpected death of a young woman: is myocardial bridging significant? A case report and review of literature. Forensic Sci Med Pathol. 2011;7(1):42-46.
- Ohtsuka T, Hirose Y, Gamo M, Sato M. Severe hypotension and atrio-ventricular block in a patient of left lung cancer associated with myocardial bridging. Masui. 2003;52(1):70-72.
___________________________________________________
From Konya University, Meram School of Medicine, Cardiology Department, Konya, Turkey.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript submitted March 27, 2012, provisional acceptance given May 16, 2012, final version accepted June 11, 2012.
Address for correspondence: Halil Ibrahim Erdogan, MD, Konya Universitesi, Meram Tip Fakultesi, Kardiyoloji Sekreterligi, Meram, 42090 Konya, Turkey. Email: drhalilibrahimerdogan@gmail.com










