

Right Coronary Artery to Coronary Sinus Fistula
Abstract: Coronary arteriovenous fistulas are very uncommon. We present a case of a very large right coronary artery to coronary sinus fistula, ultimately leading to congestive heart failure and necessitating surgical intervention.
J INVASIVE CARDIOL 2012;24(10):552-553
Key words: coronary sinus fistula
_________________________________________________________
 A 53-year-old female with hypertension and obesity presented with exertional dyspnea and chest pain which started about a year ago, and has been worsening with time. She had an unremarkable physical examination, including normal heart sounds. Her cardiac evaluation included a transesophageal echocardiography, which showed a large, tortuous right coronary artery (RCA) abutting the coronary sinus (CS) (Figures 1 and 2; Videos 1 and 2 available at invasivecardiology.com). The flow convergence measurement showed high
A 53-year-old female with hypertension and obesity presented with exertional dyspnea and chest pain which started about a year ago, and has been worsening with time. She had an unremarkable physical examination, including normal heart sounds. Her cardiac evaluation included a transesophageal echocardiography, which showed a large, tortuous right coronary artery (RCA) abutting the coronary sinus (CS) (Figures 1 and 2; Videos 1 and 2 available at invasivecardiology.com). The flow convergence measurement showed high  volume flow in the RCA (Figure 3; Video 3 available at invasivecardiology.com). Other significant findings included left ventricular hypertrophy, left atrial enlargement, as well as mild right atrial (RA) and ventricular (RV) enlargement and dysfunction. Her left ventricular ejection fraction (LVEF) was well preserved at 65%. For further evaluation, coronary angiography was obtained. It demonstrated a massively dilated right coronary artery (RCA) measuring up to 14 mm in diameter, with a fistulous connection to right atrium (RA) (Figure 4;
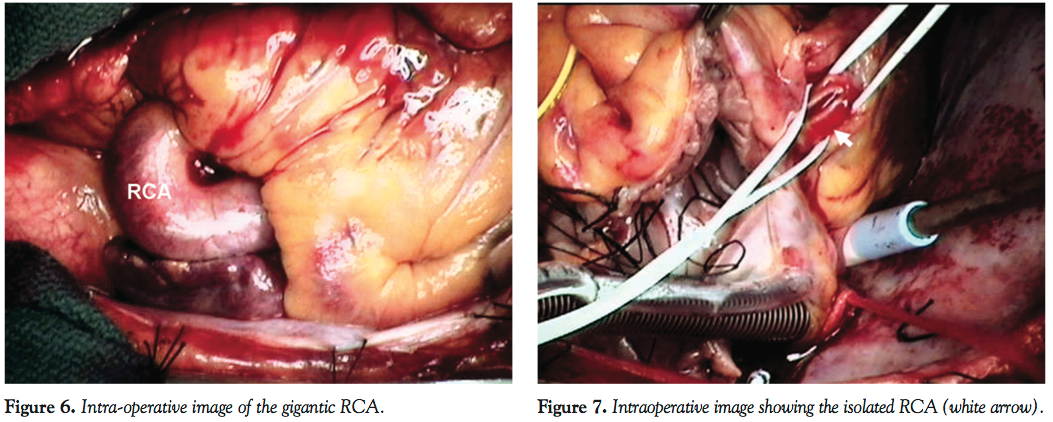
volume flow in the RCA (Figure 3; Video 3 available at invasivecardiology.com). Other significant findings included left ventricular hypertrophy, left atrial enlargement, as well as mild right atrial (RA) and ventricular (RV) enlargement and dysfunction. Her left ventricular ejection fraction (LVEF) was well preserved at 65%. For further evaluation, coronary angiography was obtained. It demonstrated a massively dilated right coronary artery (RCA) measuring up to 14 mm in diameter, with a fistulous connection to right atrium (RA) (Figure 4;  Video 4 and 5 available at invasivecardiology.com). This was followed by a computed tomography angiogram of the chest, which showed the tortuous RCA measuring 17.5 mm (Figure 5), draining into the RA via the coronary sinus (CS). Both surgery and percutaneous coil embolization were considered for the treatment of the RCA to CS fistula, and the patient chose the surgical approach. The surgery was performed 5 months from the initial diagnosis. Intra-operatively, the patient was found to have a 15 mm RCA (Figures 6 and 7;
Video 4 and 5 available at invasivecardiology.com). This was followed by a computed tomography angiogram of the chest, which showed the tortuous RCA measuring 17.5 mm (Figure 5), draining into the RA via the coronary sinus (CS). Both surgery and percutaneous coil embolization were considered for the treatment of the RCA to CS fistula, and the patient chose the surgical approach. The surgery was performed 5 months from the initial diagnosis. Intra-operatively, the patient was found to have a 15 mm RCA (Figures 6 and 7; 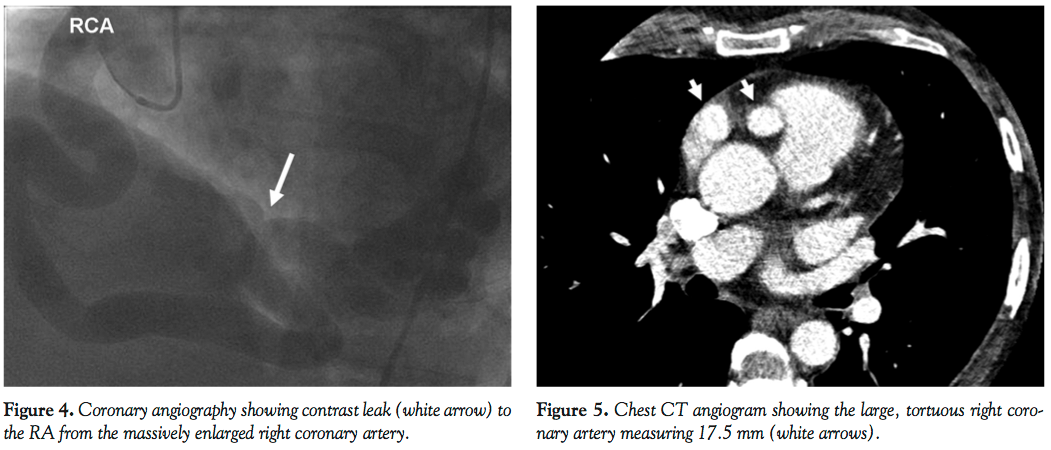 Video 6 available at invasivecardiology.com) related to the coronary sinus fistula. Her LVEF was decreased at around 40%, and her RV and RA were significantly enlarged. Continuous high-velocity flow was confirmed with the intra-operative transesophageal echocardiography. Ligation of the fistula was performed at the level of its entry into the CS without complications. The patient recovered well from her surgery, and was discharged home on the fourth postoperative day.
Video 6 available at invasivecardiology.com) related to the coronary sinus fistula. Her LVEF was decreased at around 40%, and her RV and RA were significantly enlarged. Continuous high-velocity flow was confirmed with the intra-operative transesophageal echocardiography. Ligation of the fistula was performed at the level of its entry into the CS without complications. The patient recovered well from her surgery, and was discharged home on the fourth postoperative day.
 First described by Krause in 1865,1 coronary arteriovenous fistulas are very uncommon. The incidence of coronary arteriovenous fistulas in patients undergoing diagnostic cardiac catheterization has been reported to be 0.1%.2 Although both left and right coronary tree origins are common, the right coronary tree is involved more often (50%-55%) than the left coronary tree.2,3 In order of decreasing frequency, the most common drainage sites are the RV (41%), RA (26%), pulmonary artery (17%), CS (7%), left atrium (5%), left ventricle (3%), and superior vena cava (1%).3 Although frequently asymptomatic, coronary arteriovenous fistulas often presents with chest pain, exertional dyspnea, and palpitation,4,5 and can lead to congestive heart failure, myocardial infarction, spontaneous bacterial endocarditis, and fistula rupture.4 Because of these potential complications, timely intervention is indicated.
First described by Krause in 1865,1 coronary arteriovenous fistulas are very uncommon. The incidence of coronary arteriovenous fistulas in patients undergoing diagnostic cardiac catheterization has been reported to be 0.1%.2 Although both left and right coronary tree origins are common, the right coronary tree is involved more often (50%-55%) than the left coronary tree.2,3 In order of decreasing frequency, the most common drainage sites are the RV (41%), RA (26%), pulmonary artery (17%), CS (7%), left atrium (5%), left ventricle (3%), and superior vena cava (1%).3 Although frequently asymptomatic, coronary arteriovenous fistulas often presents with chest pain, exertional dyspnea, and palpitation,4,5 and can lead to congestive heart failure, myocardial infarction, spontaneous bacterial endocarditis, and fistula rupture.4 Because of these potential complications, timely intervention is indicated.
References
- Krause W. Ueber den Ursprung einer akzessorischen A. coronaria aus der A. pulmonalis. Z Ratl Med. 1865;24:225-229.
- Vavuranakis M, Bush CA, Boudoulas H. Coronary artery fistulas in adults: incidence, angiographic characteristics, natural history. Cathet Cardiovasc Diagn. 1995;35(2):116-120.
- Levin DC, Fellows KE, Abrams HL. Hemodynamically significant primary anomalies of the coronary arteries. Angiographic aspects. Circulation. 1978;58(1):25-34.
- Liberthson RR, Sagar K, Berkoben JP, et al. Congenital coronary arteriovenous fistula. Report of 13 patients, review of the literature and delineation of management. Circulation. 1979;59(5):849-854.
- Ata Y, Turk T, Bicer M, et al. Coronary arteriovenous fistulas in the adults: natural history and management strategies. J Cardiothorac Surg. 2009;4:62.
_________________________________________________________
From the Division of Cardiac Surgery, University of Rochester Medical Center, Rochester, New York.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript submitted April 2, 2012 and accepted May 16, 2012.
Address for correspondence: Vakhtang Tchantchaleishvili, MD, University of Rochester Medical Center, Box Cardiac Surgery, 601 Elmwood Avenue, Rochester, NY 14642. Email: Vakhtang_Tchantchaleishvili@urmc.rochester.edu










