

Safety and Effectiveness of the Nav-6 Filter in Preventing Distal Embolization During Jetstream Atherectomy of Infrainguinal Peripheral Artery Lesions
Abstract: Background. The risk of distal embolization (DE) during infrainguinal peripheral artery interventions (PAI) is often mitigated by the use of embolic protection devices. There are limited data on the use of filters with the Jetstream (JS) atherectomy device (Boston Scientific), a rotational cutter with aspiration capacity. The Nav-6 filter is uniquely suited for use with the JS due to its wire compatibility and detachment from the filter; however, data on the off-label use of this combination have not been reported. Methods. Consecutive patients between October 2008 and April 2015 undergoing endovascular infrainguinal PAI with JS were analyzed as part of the Excellence in Peripheral Artery Disease (XL-PAD) registry (NCT01904851). Patients were divided into two subgroups with Nav-6 filter use vs no filter use. Descriptive and univariate analyses were performed. Results. Among 141 patients (mean age, 67.8 ± 10.8 years; 169 lesions) included in this study, the Nav-6 filter was used in 82 (59%). Use of a filter was more frequent in longer lesions (146 ± 106 mm vs 91 ± 72 mm; P=.01), in more severe stenoses (95% vs 87%; P=.04), and in chronic total occlusions (33% vs 8.3%; P=.01). Patients receiving filters had longer procedure duration (102 ± 51 min vs 66 ± 41 min; P=.01) and longer fluoroscopy times (31 ± 16 min vs 21 ± 10 min; P<.001). Use of the Nav-6 filter with the JS during PAI was associated with numerically lower rates of DE (1.8% vs 8%; P=.10) and similar rates of death and amputation. At 12 months, the target-lesion revascularization rate was higher in the filter group (22% vs 2.7%; P=.02), likely secondary to use of the filter in more complex lesions. Conclusion. Nav-6 filter during JS atherectomy was predominantly used during complex infrainguinal PAI and was associated with less occurrence of DE.
J INVASIVE CARDIOL 2016;28(8):330-333. Epub 2016 May 15.
Key words: Jetstream device, atherectomy, distal embolization, embolic filter, Nav-6 filter, infrainguinal disease, peripheral arterial disease, peripheral intervention
Distal embolization (DE) occurs frequently during infrainguinal interventions and requires additional treatment in 2%-10% of cases.1-7 Predictors of DE include long lesion length, total occlusion, thrombus, moderate to severe calcifications, and the use of atherectomy devices.5-9 Embolic protection has been used to varying degrees among different operators.10,11 The overall cost-effectiveness of embolic protection devices has not been evaluated, but their use has been associated with frequent capture of embolic debris, less patient and operator radiation dose, reduced use of contrast, shorter hospital stay, and lower procedural times.12,13
The Jetstream (JS) atherectomy device (Boston Scientific) is a rotational and aspirational atherectomy catheter indicated for treatment of infrainguinal peripheral arterial disease.14 DE continues to occur with JS atherectomy.14-16 Although the off-label use of the Spider filter (Medtronic) was performed with the JS device, it is currently not recommended in the Instructions for Use label because of the potential risk of wire entrapment on the device.17 Also, the Spider filter and its wire are one unit, and wire motion with advancement of the JS leads to basket movement, which potentially carries the risk of vessel spasm and dissection. The Nav-6 filter (Abbott Vascular), on the other hand, has a detached wire from its filter and therefore wire motion does not move the basket. Furthermore, there is no known incompatibility with the use of the BareWire (Abbott Vascular), which is typically used with this filter. In this study, we review the experience of operators with the use of the Nav-6 filter with the JS device in the Excellence in Peripheral Arterial Disease (XL-PAD) multicenter registry (NCT01904851).
Methods
The XLPAD registry is a multicenter peripheral arterial disease registry with eleven sites contributing consecutive patients treated for femoropopliteal arterial occlusive disease. The registry uses a web-based electronic data capture system (RedCap) for data acquisition. The cine films are reviewed by a core laboratory at the VA Medical Center in Dallas, Texas. Consecutive patients between October 2008 and April 2015 undergoing endovascular infrainguinal PAI with JS were analyzed as part of the XL-PAD registry. Patients were divided into two subgroups: Nav-6 filter use and no filter use. DE is a captured variable in the registry. Demographic, angiographic, procedural, and 12-month outcome data were analyzed. Continuous variables were described as mean ± standard deviation and compared using t-test or Wilcoxon rank-sum test, as appropriate. Nominal variables were presented as percentages and compared using Chi-square test. Descriptive and univariate analyses were performed using JMP version 11.0 (SAS Institute).
Results
A total of 141 patients (mean age, 67.8 ± 10.8 years; 169 lesions) were included in this study. Table 1 illustrates demographic and clinical variables. Patients in the no filter group were older, but they had the same degree of mean Rutherford-Becker category and ankle-brachial index. There were more males who received the filter than females. The rates of diabetes, smoking, hypertension, and chronic kidney disease were similar between the two groups.
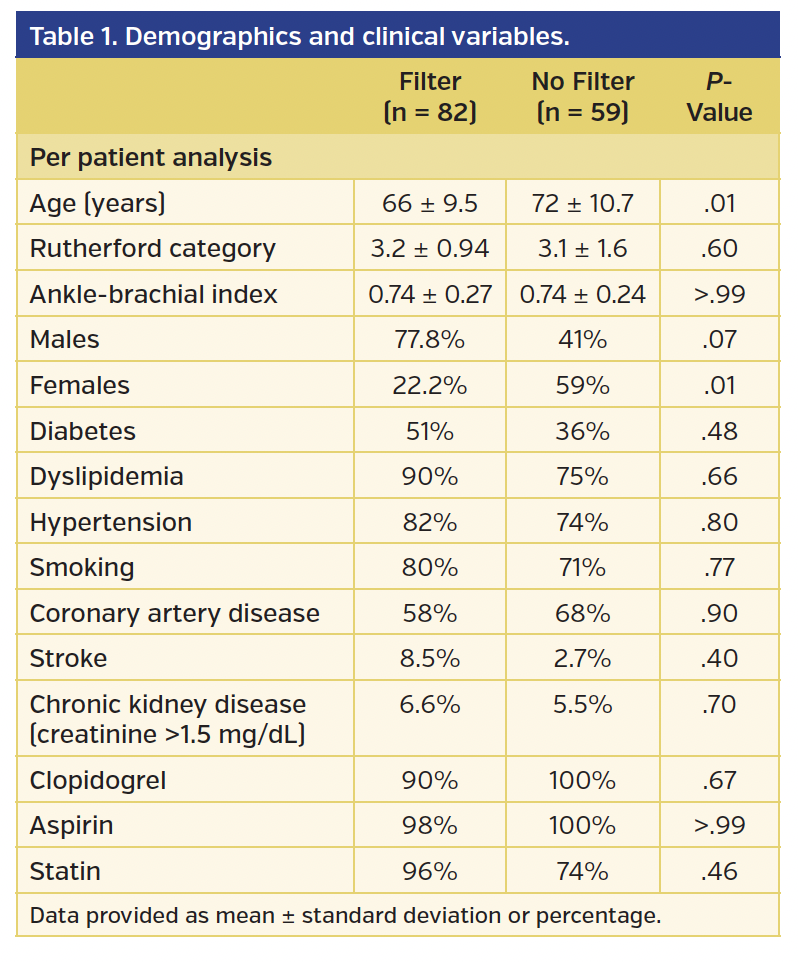
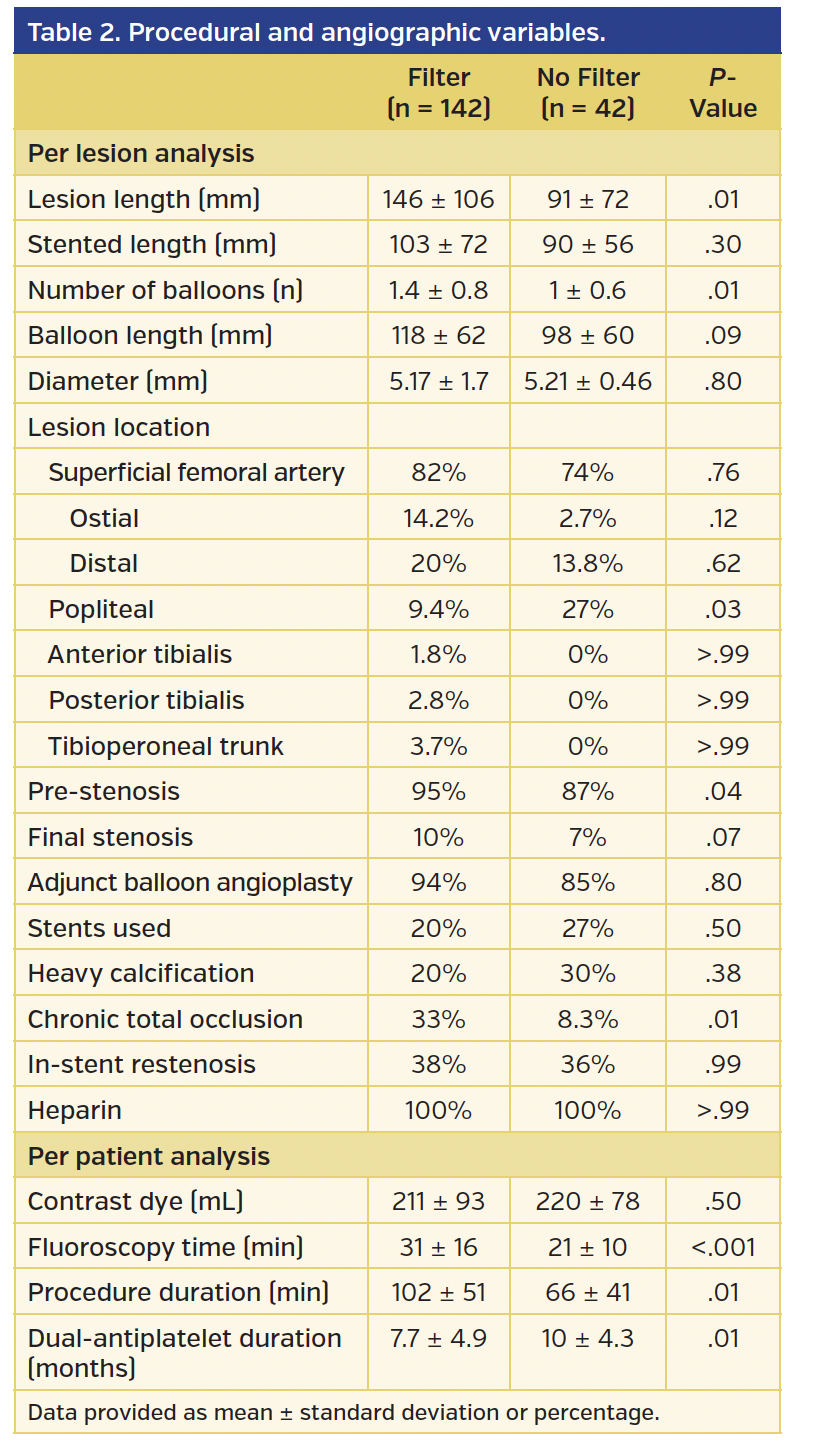
Table 2 illustrates angiographic and procedural variables. Nav-6 filter was used in 82 patients (58.2%). Use of a filter was more frequent for longer lesions (146 ± 106 mm vs 91 ± 72 mm; P=.01), severe stenoses (95% vs 87%; P=.04), and chronic total occlusions (33% vs 8.3%; P=.01). Patients receiving filters had longer procedures (102 ± 51 min vs 66 ± 41 min) and fluoroscopy times (31 ± 16 min vs 21 ± 10 min; P<.001), reflecting a more complex disease treated under embolic filter protection, particularly chronic occlusions and long lesions. Most lesions treated were in the femoropopliteal and over one-third of limbs treated had in-stent restenoses.
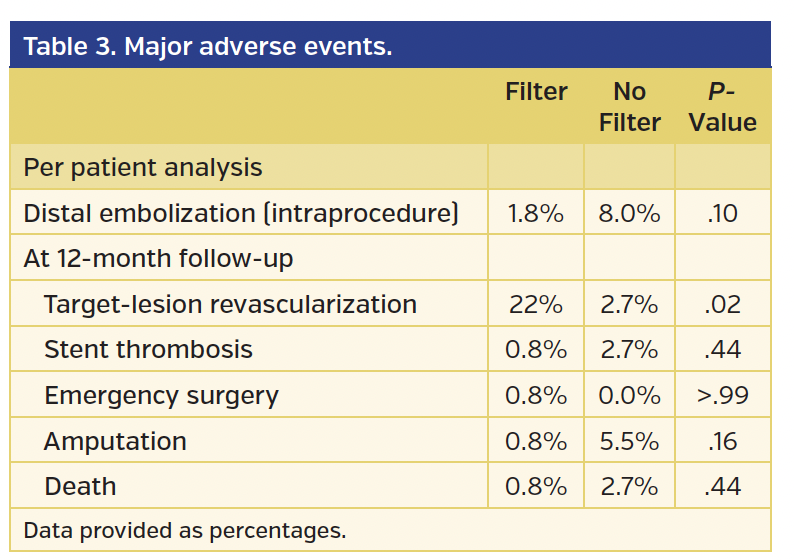
The use of the Nav-6 filter with the JS during PAI was associated with numerically lower rates of DE (1.8% vs 8.0%, respectively; P=.10) (Table 3). Death and amputation rates were low and similar in both groups. Twelve-month target-lesion revascularization rate was higher in the filter group (22% vs 2.7%; P=.02), likely secondary to the more complex lesions treated. There were no device-related problems reported. Also, no spasms or dissections at the site of the filter positioning were reported. Filter retrieval was successful in all patients.
Discussion
Distal embolization is a major concern with the increase in the use of atherectomy for femoropopliteal interventions.2,4-7 Distal embolization has generally been reported in 1%-10% of lower-extremity endovascular procedures.4-7,17-19 Main clinical concerns include the potential for increased incidence of acute limb ischemia with worse limb salvage rates, increased procedure time and radiation exposure to patient and operator,12 and loss of good outflow, which may result in adverse long-term outcomes.20-22 Although the use of embolic protection devices (EPDs) has shown to provide a protective effect against DE (particularly when treating high-risk lesions), high cost remains a concern. In addition, EPDs can potentially cause damage to the inner vessel wall, resulting in dissection and spasm at the landing site of the filter. In this study, EPDs were used more frequently in high-risk anatomy including total occlusions and long calcified disease, which are known to be independent predictors of DE. The procedural times, radiation exposure amounts, and overall outcomes were worse in the filter group; this was predominantly related to the more complex disease treated in this group. Despite the complex anatomy in the filter group and the higher DE potential, the filter group had numerically and clinically less DE requiring treatment compared with the less complex patients with no filter (1.8% vs 8%; P>.99).
Jetstream atherectomy is an upgraded version of the Pathway atherectomy system, with more aspiration and cutting capacity. In the Pathway PVD trial,16 “minor” DE occurred in 10% of patients with no filter, and all patients were managed successfully. In the Jetstream Calcium study,23 again no filter was used and DE was not noted despite treatment of moderate and severe calcified disease. Both studies, however, included short lesions (mean lesion length, 2.7 cm in the Pathway PVD study and 4.5 cm in the Jetstream Calcium study). In contrast, preliminary data from the JET registry15 of 155 patients showed a DE rate of 2.2% who required additional treatment. EPD was used in only 19% of patients and mean lesion length was 22 cm. Also, data from the feasibility JetStream ISR study17 indicated a DE rate of 9.4% requiring treatment (2 out of 3 limbs with no filters and 1 out of 3 limbs with Spider filter). In this registry, 50% of limbs treated were done under EPD and macrodebris were noted in 12.5% of filters. Finally, in the Excellence in Peripheral Arterial Disease (xlPAD) registry,14 DE occurred in 4.4% of patients; none of these patients had an EPD, which was used in 42.6% of cases overall, and mean lesion length was 13.4 cm. These data indicate that Jetstream atherectomy causes minimal or no DE in shorter lesions <5 cm (despite significant calcification, as seen in the Jetstream Calcium study), but DE requiring treatment may occur in long lesions particularly when EPDs are not used. This is consistent with our data where DE continued to occur in long complex disease with the Jetstream device and EPD seems to be at least numerically protective against DE.
Although the DE rate has not been directly compared between atherectomy devices, DE seems to occur at higher frequency with laser atherectomy4,6,18 and SilverHawk/TurboHawk atherectomy,2,5-7 as seen in several studies, occurring in close to the majority of patients with complex disease treated with directional atherectomy and almost one-half of the patients treated with laser as captured by EPD. In the PROTECT registry,5 the Spider FX or EmboShield (Abbott Vascular) EPDs were used in 40 consecutive patients (50 lesions) who had at least one high-risk feature for DE, namely, moderate to severe calcification, chronic total occlusion, angiographic filling defect suggestive of an intravascular thrombus, ulcerated lesions at least 30 mm in length, or long lesions (≥50 mm). Forty-three lesions were treated with balloon angioplasty with or without stenting and 13 lesions were treated with SilverHawk atherectomy and adjunctive balloon angioplasty. Debris <2 mm in length and clinically significant macroembolization (≥2 mm in length) occurred in 100% and 90.9% of the SilverHawk group, respectively, and in 37.9% and 27.6% of the non-atherectomy group, respectively. The logistic regression analysis identified SilverHawk treatment versus percutaneous transluminal angioplasty with or without stenting as an independent predictor of clinically significant DE (odds ratio, 31; 95% confidence interval, 3.31-300.34; P<.01). Restenotic lesions were also predictive (odds ratio, 15; 95% confidence interval, 2.53-90.90; P<.01) of significant DE compared with de novo lesions. In the DEEP Emboli study,4 EPDs were used in 20 patients who were treated with excimer laser for complex disease. Macrodebris were found in 12 of 18 patients (66.7%) after treatment with the laser and in 7 of 20 patients (35.0%) after adjunctive treatment. It is speculated that the aspiration property of the Jetstream device contributes to reducing the rate of DE, but comparative trials among atherectomy devices are needed to prove this observation.
Conclusion
These data indicate that DE is highly prevalent during peripheral artery intervention and occurs during treatment of a wide variety of lesions encountered in clinical practice, reinforcing the potential need for distal embolic protection, especially with atherectomy. However, it is imperative that the cost-effectiveness of embolic filter protection be validated in a large randomized trial before universal adoption can be recommended.
References
1. Karnabatidis D, Katsanos K, Kagadis GC, et al. Distal embolism during percutaneous revascularization of infra-aortic arterial occlusive disease: an underestimated phenomenon. J Endovasc Ther. 2006;13:269-280.
2. Roberts D, Niazi K, Miller W, et al; for the DEFINITIVE Ca++ Investigators. Effective endovascular treatment of calcified femoropopliteal disease with directional atherectomy and distal embolic protection: final results of the DEFINITIVE Ca(++) trial. Catheter Cardiovasc Interv. 2014;84:236-244.
3. Shammas NW, Weissman NJ, Coiner D, et al. Treatment of subacute and chronic thrombotic occlusions of lower extremity peripheral arteries with the excimer laser: a feasibility study. Cardiovasc Revasc Med. 2012;13:211-214.
4. Shammas NW, Coiner D, Shammas GA, et al. Distal embolic event protection using excimer laser ablation in peripheral vascular interventions: results of the DEEP EMBOLI registry. J Endovasc Ther. 2009;16:197-202.
5. Shammas NW, Dippel EJ, Coiner D, et al. Preventing lower extremity distal embolization using embolic filter protection: results of the PROTECT registry. J Endovasc Ther. 2008;15:270-276.
6. Lam RC, Shah S, Faries PL, et al. Incidence and clinical significance of distal embolization during percutaneous interventions involving the superficial femoral artery. J Vasc Surg. 2007;46:1155-1159.
7. Suri R, Wholey MH, Postoak D, et al. Distal embolic protection during femoropopliteal atherectomy. Catheter Cardiovasc Interv. 2006;67:417-422.
8. Shammas NW, Shammas GA, Dippel EJ, et al. Predictors of distal embolization in peripheral percutaneous interventions: a report from a large peripheral vascular registry. J Invasive Cardiol. 2009;21:628-631.
9. Shrikhande GV, Khan SZ, Hussain HG, et al. Lesion types and device characteristics that predict distal embolization during percutaneous lower extremity interventions. J Vasc Surg. 2011;53:347-352.
10. Lookstein RA, Lewis S. Distal embolic protection for infrainguinal interventions: how to and when? Tech Vasc Interv Radiol. 2010;13:54-58.
11. Müller-Hülsbeck S, Schäfer PJ, Hümme TH, et al. Embolic protection devices for peripheral application: wasteful or useful? J Endovasc Ther. 2009;16(Suppl 1):I163-I169.
12. Shammas NW, Shammas GA, Dippel EJ, et al. Intraprocedural outcomes following distal lower extremity embolization in patients undergoing peripheral percutaneous interventions. Vasc Dis Management. 2009;6:58-61.
13. Dippel EJ, Parikh N, Wallace KL. Use of SpiderFX embolic protection device vs distal embolic event: hospital length of stay, operating room time, costs and mortality (abstr). J Am Coll Cardiol. 2013;62:B161.
14. Shammas NW, Sarode K, Mohammad A, et al. Indications for use and outcomes with the Jetstream atherectomy device from the XLPAD registry. Presented at SCAI 2015, San Diego May 6-9, 2015. Catheter Cardiovasc Interv. 2015;Abstracts 082:S51.
15. Shammas NW, Gray W, Garcia L, et al; for the JET Investigators. Procedural success and in-hospital outcomes in treating femoropopliteal arteries with the Jetstream Navitus system in the post-market JET registry. Presented at CRT, Washington DC, February 2015. JACC Cardiovasc Interv. 2015;8(Suppl S):S35.
16. Zeller T, Krankenberg H, Steinkamp H, et al. One-year outcome of percutaneous rotational atherectomy with aspiration in infrainguinal peripheral arterial occlusive disease: the multicenter pathway PVD trial. J Endovasc Ther. 2009;16:653-662.
17. Shammas NW, Shammas GA, Park H, et al. Safety and in-hospital outcomes of JetStream atherectomy in treating in-stent restenosis of femoropopliteal arteries. Presented at American College of Cardiology Scientific Sessions, San Diego, CA, March 2015. JACC. 2015;65:A1812.
18. Dippel EJ, Makam P, Kovach R, et al; EXCITE ISR Investigators. Randomized controlled study of excimer laser atherectomy for treatment of femoropopliteal in-stent restenosis: initial results from the EXCITE ISR trial (EXCImer Laser Randomized Controlled Study for Treatment of FemoropopliTEal In-Stent Restenosis). JACC Cardiovasc Interv. 2015;8:92-101. Epub 2014 Dec 10.
19. Siablis D, Karnabatidis D, Katsanos K, et al. Outflow protection filters during percutaneous recanalization of lower extremities’ arterial occlusions: a pilot study. Eur J Radiol. 2005;55:243-249.
20. Smolock CJ, Anaya-Ayala JE, El-Sayed HF, et al. Clinical efficacy of concomitant tibial interventions associated with superficial femoral artery interventions in critical limb ischemia. J Vasc Surg. 2013;57:19-27.
21. Davies MG, Saad WE, Peden EK, et al. Impact of runoff on superficial femoral artery endoluminal interventions for rest pain and tissue loss. J Vasc Surg. 2008;48:619-625.
22. Ihnat DM, Duong ST, Taylor ZC, et al. Contemporary outcomes after superficial femoral artery angioplasty and stenting: the influence of TASC classification and runoff score. J Vasc Surg. 2008;47:967-974.
23. Maehara A, Mintz GS, Shimshak TM, et al. Intravascular ultrasound evaluation of Jetstream atherectomy removal of superficial calcium in peripheral arteries. EuroIntervention. 2015;11:96-103.
From the 1VA North Texas Health Care System, Dallas, Texas; 2Dallas VA Medical Center, Dallas, Texas; 3VA North Texas Healthcare System and UT Southwestern Medical Center, Dallas, Texas; and 4Midwest Cardiovascular Research Foundation, Davenport, Iowa.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. Dr Mohammad reports consulting fees from Medicure. Dr Brilakis reports consulting/speaker honoraria from Abbott Vascular, Asahi Intecc, Boston Scientific, Elsevier, GE Healthcare, Somahlution, St. Jude Medical, and Terumo; research support from Boston Scientific and InfraRedx; spouse is an employee of Medtronic. Dr S. Banerjee reports research grants from Boston Scientific, the Medicines Company; consultant/speaker honoraria from Gilead, St Jude, Cordis, Boehinger Ingerheim, Sanofi, Medtronic; ownership in MDCare Global (spouse); intellectual property in HygeiaTel. Dr Shammas receives educational and research grants from Boston Scientific and Abbott to the Midwest Cardiovascular Research Foundation. He is a trainer for Jetstream atherectomy and is on the steering committee of the JET registry and the principal investigator for JetStream ISR. Other conflicts of interest can be found on www.mcrfmd.com. The remaining authors report no conflicts of interest regarding the content herein.
Manuscript submitted March 1, 2016 and accepted March 15, 2016.
Address for correspondence: Nicolas W. Shammas, MD, MS, FACC, FSCAI, Midwest Cardiovascular Research Foundation, 1622 E. Lombard Street, Davenport, IA 52803. Email: shammas@mchsi.com











