

A Self-Expandable Coronary Stent System to Treat Complex Coronary Stenosis Complicated by Poststenotic Aneurysm: An Optical Coherence Tomographic Evidence-Based Case Report
ABSTRACT: Coronary artery aneurysm is a relatively uncommon disorder characterized by coronary artery dilatation with diameter that exceeds 50% of the normal adjacent segments with atherosclerosis being the most common etiology.1 Aneurysms can be adjacent to a stenosis in a post- or prestenotic location. Both anatomical conditions are technically challenging regarding their percutaneous treatment because of the large discrepancy in size between the stenotic and dilated segments, and require careful choice of the most appropriate technique and device. We have successfully treated a coronary stenosis complicated by a poststenotic aneurysm in a 60-year-old patient with atypical angina using a novel self-expandable coronary stent system implanted with optical coherence tomography (OCT) guidance. OCT scan after implantation showed residual stent malapposition inside the aneurysm despite postdilatation. Thanks to the ability of this stent to self-expand over time, 6-month OCT follow-up showed an optimal result in terms of stent apposition, strut coverage, and absence of in-stent restenosis.
J INVASIVE CARDIOL 2011;23(12):E277-E280
______________________________________________
Coronary artery aneurysm is relatively uncommon, with incidence from 0.3% to 4.9%, characterized by coronary artery dilatation with diameter that exceeds 50% of the normal adjacent segments.1 Atherosclerosis is the most common etiology in adults.2,3 Weakening of the tunica media and hemodynamic factors play an important role in the formation of aneurysms. The observation of poststenotic aneurysms suggests the transformation, beyond the stenosis, of potential energy into kinetic energy resulting in increased lateral pressure and dilation of the vessel wall downstream of the stenosis. Aneurysms can also be prestenotic, the formation of which is linked to the increased lateral pressure upstream from the stenosis.4,5 Indications for the treatment of this disorder and the techniques to use remain to be determined.6 In the presence of a poststenotic aneurysm, the percutaneous treatment of the stenosis presents considerable technical difficulties caused by the large discrepancy in size between stenosis and dilatation. This condition requires careful choice of the best device to be used and represents a challenge for the interventional cardiologist. The Stentys stent (STENTYS S.A.) is a novel self-expandable coronary stent system designed to allow optimal adaptation of the stent struts to the vessel wall in order to reduce the occurrence of stent malapposition that is considered one of the most powerful morphometric predictors of stent thrombosis.7,8 Optical coherence tomography (OCT) is a novel high-resolution invasive coronary imaging technique that allows fast scan of long coronary segments with the possibility of assessing vessel size, atherosclerosis morphology, and stent architecture with sub-millimeter resolution that is currently 10 times higher than intravascular ultrasound. OCT could be helpful in planning and guiding the optimal treatment of complex coronary disease.9,10
Case Report
 A 60-year-old male Caucasian patient who was hypertensive, dyslipidemic, and a heavy smoker, presented with a history of syncopal episode about 7 months prior without evidence of brain disease on a subsequent CT scan. Two weeks later, the patient reported several episodes of atypical angina. A series of investigations were then performed, including:
A 60-year-old male Caucasian patient who was hypertensive, dyslipidemic, and a heavy smoker, presented with a history of syncopal episode about 7 months prior without evidence of brain disease on a subsequent CT scan. Two weeks later, the patient reported several episodes of atypical angina. A series of investigations were then performed, including:
- Electrocardiogram that showed no significant changes;
- Echocardiogram that showed hypokinesis of the left ventricular inferior and posterior walls with an ejection fraction of 48%; and
- Stress/rest myocardial SPECT (99mTc-MIBI) with maximal exercise testing that was positive for inducible mild myocardial ischemia in the inferior and posteroseptal walls.
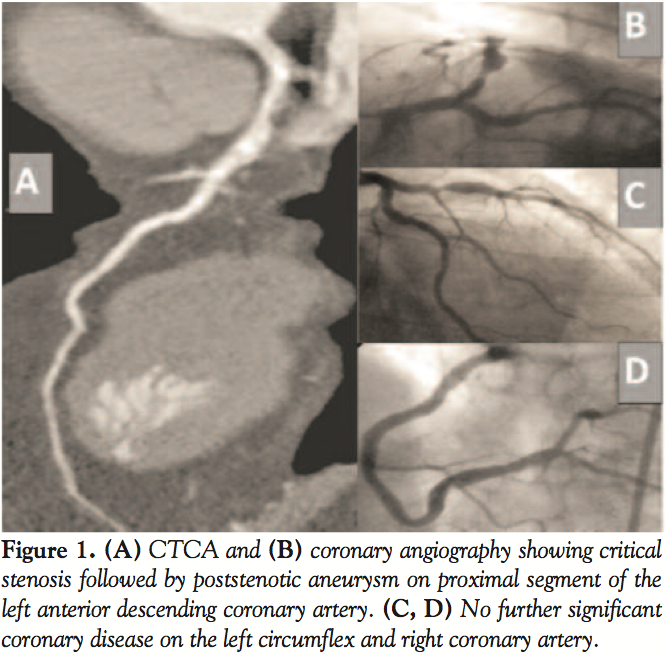
 Following these equivocal results, the patient underwent a 64-slice computed tomography coronary angiography (CTCA), which showed critical stenosis in the proximal left anterior descending (LAD) followed by poststenotic aneurysm (Figure 1A). The patient was then admitted to our hospital asymptomatic for elective diagnostic catheterization. Coronary angiography confirmed the presence of a significant stenosis at the level of the proximal LAD complicated by the poststenotic aneurysm (Figure 1B); no other significant coronary disease was
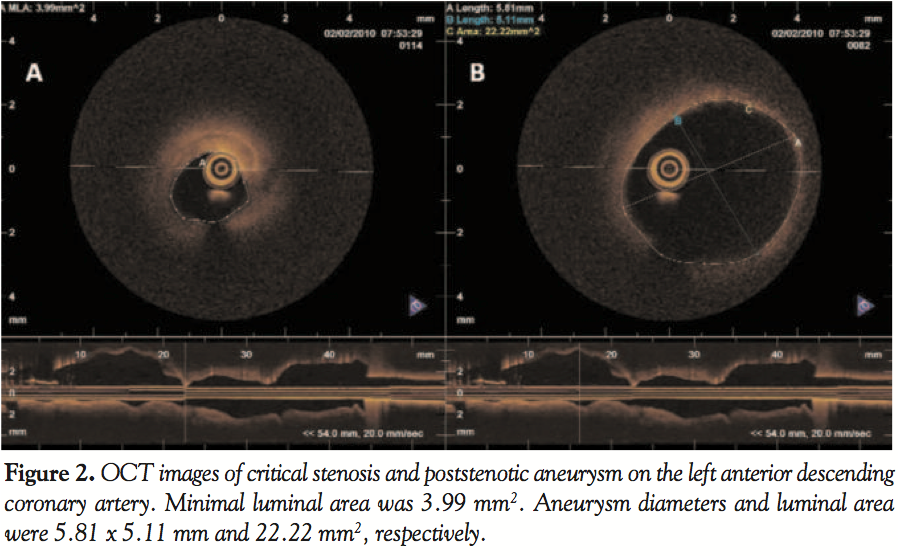
Following these equivocal results, the patient underwent a 64-slice computed tomography coronary angiography (CTCA), which showed critical stenosis in the proximal left anterior descending (LAD) followed by poststenotic aneurysm (Figure 1A). The patient was then admitted to our hospital asymptomatic for elective diagnostic catheterization. Coronary angiography confirmed the presence of a significant stenosis at the level of the proximal LAD complicated by the poststenotic aneurysm (Figure 1B); no other significant coronary disease was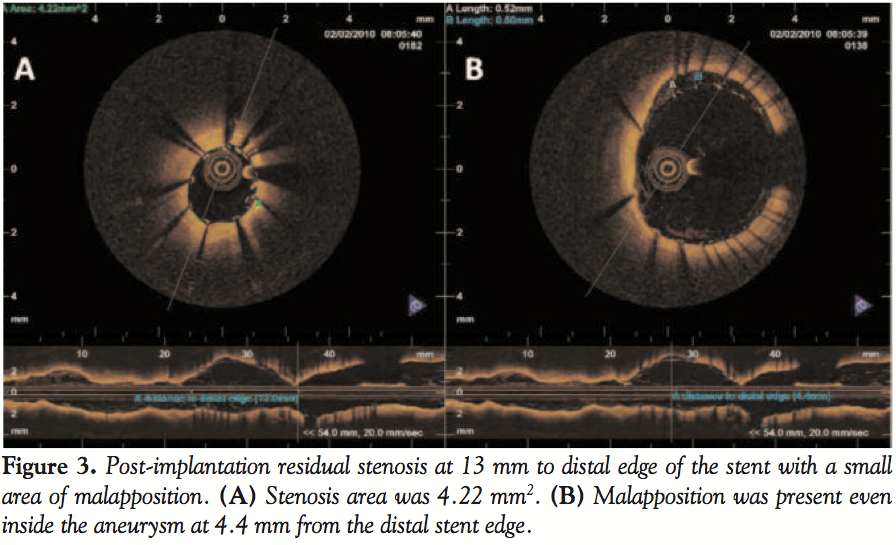 found in the remaining coronary tree (Figures 1C and 1D). In the same session, a frequency domain optical coherence tomography (FD-OCT) scan of the LAD was performed using the C7XR OCT image system (St. Jude Medical, Inc.) for lesion assessment. After administration of a bolus of 70 IU/kg unfractionated heparin, the left coronary artery was cannulated with an XB guiding catheter (Cordis Corporation) and a standard 0.014-inch coronary guidewire was positioned at the distal LAD. Since
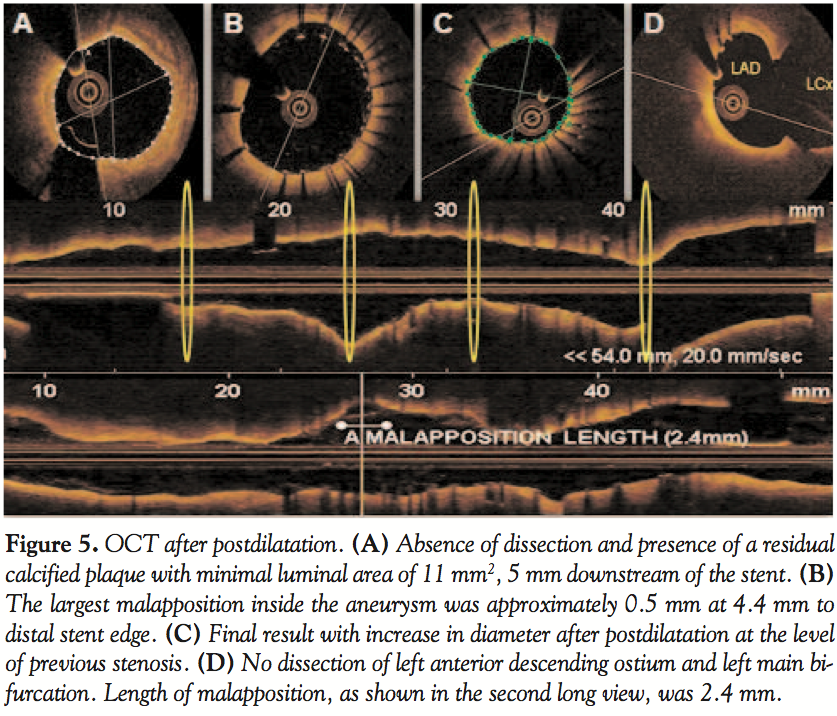
found in the remaining coronary tree (Figures 1C and 1D). In the same session, a frequency domain optical coherence tomography (FD-OCT) scan of the LAD was performed using the C7XR OCT image system (St. Jude Medical, Inc.) for lesion assessment. After administration of a bolus of 70 IU/kg unfractionated heparin, the left coronary artery was cannulated with an XB guiding catheter (Cordis Corporation) and a standard 0.014-inch coronary guidewire was positioned at the distal LAD. Since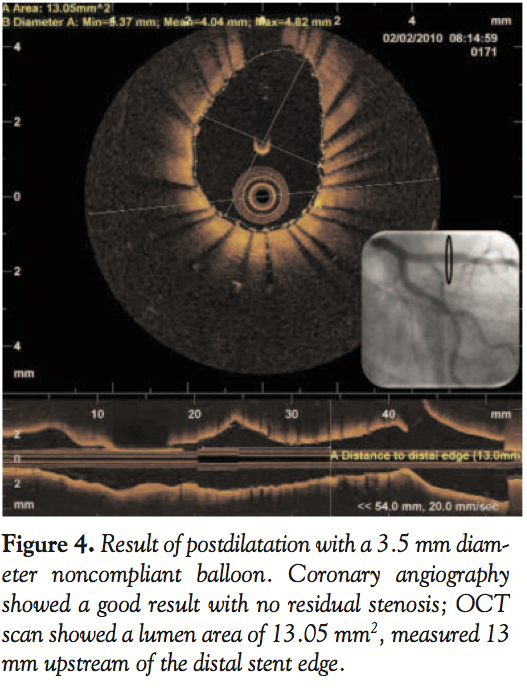 the OCT-derived minimal luminal area was consistent with a hemodynamically significant stenosis according to the intravascular ultrasound criteria,11 we decided to proceed with stenting of the proximal LAD stenosis. We used the novel STENTYS self-expandable 3.5-4.5 x 22 mm coronary stent system to treat the coronary stenosis and to avoid stent underexpansion within the poststenotic aneurysm. After stent deployment, OCT analysis showed a significant in-stent residual stenosis at 13 mm to distal edge of the stent with concomitant stent malapposition at the level of both the stenosis and the aneurysm (Figure 3). In order to optimize the acute result, high pressure postdilatation with a 3.5 x 15 mm non-compliant Quantum Maverick Balloon (Boston Scientific Corporation) was performed at the level of stenosis, avoiding the distal portion of the stent protruding into the aneurysm to avoid the risk of coronary rupture. The final OCT scan showed complete apposition of the stent in its proximal segment with a lumen area of 13 mm2 and diameters of 3.37 x 4.82 mm at 13 mm to distal edge of the stent, with no intimal dissection or plaque protrusion (Figure 4). It also showed persistence of strut malapposition inside the aneurysm with a maximal stent-to-wall distance of approximately 0.5 mm and a length of the malapposed segment of 2.4 mm at 4.4 mm to the distal edge of the stent (Figure 5). Final angiography showed a good result with TIMI 3 flow and no residual stenosis on LAD. Six months later, an elective follow-up coronary angiography and OCT scan were performed to assess the long-term result of percutaneous intervention, particularly in terms of stent strut coverage and apposition, especially inside the aneurysm. Coronary angiography showed TIMI 3 flow and absence of restenosis. OCT analysis showed optimal stent apposition with complete strut coverage and absence of restenosis, both at the level of the previously stenotic tract and inside the aneurysm. An increase in stent diameter compared to the index procedure was found not only at the level of the aneurysm, ensuring complete apposition, but also at the level of the previously treated stenosis as an effect of the radial force developed during stent self-expansion with further improvement in vessel diameters (Figure 6).
the OCT-derived minimal luminal area was consistent with a hemodynamically significant stenosis according to the intravascular ultrasound criteria,11 we decided to proceed with stenting of the proximal LAD stenosis. We used the novel STENTYS self-expandable 3.5-4.5 x 22 mm coronary stent system to treat the coronary stenosis and to avoid stent underexpansion within the poststenotic aneurysm. After stent deployment, OCT analysis showed a significant in-stent residual stenosis at 13 mm to distal edge of the stent with concomitant stent malapposition at the level of both the stenosis and the aneurysm (Figure 3). In order to optimize the acute result, high pressure postdilatation with a 3.5 x 15 mm non-compliant Quantum Maverick Balloon (Boston Scientific Corporation) was performed at the level of stenosis, avoiding the distal portion of the stent protruding into the aneurysm to avoid the risk of coronary rupture. The final OCT scan showed complete apposition of the stent in its proximal segment with a lumen area of 13 mm2 and diameters of 3.37 x 4.82 mm at 13 mm to distal edge of the stent, with no intimal dissection or plaque protrusion (Figure 4). It also showed persistence of strut malapposition inside the aneurysm with a maximal stent-to-wall distance of approximately 0.5 mm and a length of the malapposed segment of 2.4 mm at 4.4 mm to the distal edge of the stent (Figure 5). Final angiography showed a good result with TIMI 3 flow and no residual stenosis on LAD. Six months later, an elective follow-up coronary angiography and OCT scan were performed to assess the long-term result of percutaneous intervention, particularly in terms of stent strut coverage and apposition, especially inside the aneurysm. Coronary angiography showed TIMI 3 flow and absence of restenosis. OCT analysis showed optimal stent apposition with complete strut coverage and absence of restenosis, both at the level of the previously stenotic tract and inside the aneurysm. An increase in stent diameter compared to the index procedure was found not only at the level of the aneurysm, ensuring complete apposition, but also at the level of the previously treated stenosis as an effect of the radial force developed during stent self-expansion with further improvement in vessel diameters (Figure 6).
Discussion
 This case report provides evidence that significant coronary stenosis associated with poststenotic aneurysm can be safely and effectively treated with the self-expandable Stentys stent, ensuring full stent apposition and coverage at the level of both the stenotic and aneurysmal segments. This solves the problem created by the large discrepancy in size between these 2 segments of the coronary artery. We used the Stentys stent because of its ability to self-expand over time, which provides an optimal stent apposition even in vessels with highly discrepant sizes that are difficult or impossible to treat optimally with traditional balloon-expandable stents. In our case, OCT was effective to guide this complex coronary intervention, providing important information with regard to lesion morphology and the acute and long-term results of both stent apposition and coverage. We found that a FD-OCT system can provide full vessel visualization, even in large coronary aneurysms, overcoming the limitations of previous available time domain OCT systems.10 It is becoming a reasonable alternative to intravascular ultrasound as a guide for complex coronary intervention with improved spatial resolution.
This case report provides evidence that significant coronary stenosis associated with poststenotic aneurysm can be safely and effectively treated with the self-expandable Stentys stent, ensuring full stent apposition and coverage at the level of both the stenotic and aneurysmal segments. This solves the problem created by the large discrepancy in size between these 2 segments of the coronary artery. We used the Stentys stent because of its ability to self-expand over time, which provides an optimal stent apposition even in vessels with highly discrepant sizes that are difficult or impossible to treat optimally with traditional balloon-expandable stents. In our case, OCT was effective to guide this complex coronary intervention, providing important information with regard to lesion morphology and the acute and long-term results of both stent apposition and coverage. We found that a FD-OCT system can provide full vessel visualization, even in large coronary aneurysms, overcoming the limitations of previous available time domain OCT systems.10 It is becoming a reasonable alternative to intravascular ultrasound as a guide for complex coronary intervention with improved spatial resolution.
 OCT is a high-resolution imaging technique that has been recently introduced in the clinical scenario in order to provide in vivo information on coronary artery anatomy with near light microscopy resolution. The high resolution of this imaging technique enables detailed evaluation not only of coronary atherosclerotic plaques but also regarding the vascular response to coronary interventional devices, such as new-generation coronary stents, providing important information on stent apposition, neointima formation and strut coverage over time in patients with potentially significant clinical implications.1-12 In recent years, the need for more precise information regarding coronary artery disease to achieve optimal treatment has seen intravascular imaging become an area of primary importance in interventional cardiology. OCT in this field has grown and is spreading. It benefits both therapeutic and research purposes and also fills gaps in conventional invasive coronary imaging.
OCT is a high-resolution imaging technique that has been recently introduced in the clinical scenario in order to provide in vivo information on coronary artery anatomy with near light microscopy resolution. The high resolution of this imaging technique enables detailed evaluation not only of coronary atherosclerotic plaques but also regarding the vascular response to coronary interventional devices, such as new-generation coronary stents, providing important information on stent apposition, neointima formation and strut coverage over time in patients with potentially significant clinical implications.1-12 In recent years, the need for more precise information regarding coronary artery disease to achieve optimal treatment has seen intravascular imaging become an area of primary importance in interventional cardiology. OCT in this field has grown and is spreading. It benefits both therapeutic and research purposes and also fills gaps in conventional invasive coronary imaging.
We conclude emphasizing the high performance of the Stentys stent that led to the complete coverage of the aneurysm without complication during PCI, but especially without stent malapposition or restenosis at 6-month OCT follow-up.
References
- Swaye PS, Fisher LD, Litwin P, et al. Aneurysmal coronary artery disease. Circulation. 1983;67(1):134-138.
- Syed M, Lesch M. Coronary artery aneurysm: a review. Prog Cardiovasc Dis. 1997;40(1):77-84.
- Demopoulos VP, Olympios CD, Fakiolas CN, et al. The natural history of aneurysmal coronary artery disease. Heart. 1997;78(2):136-141.
- Virmani R, Robinowitz M, Atkinson JB, et al. Acquired coronary arterial aneurysms: an autopsy study of 52 patients. Human Pathol. 1986;17(6):575-583.
- Markis JE, Joffe CD, Cohn PF, Feen DJ, Herman MV, Gorlin R. Clinical significance of coronary artery ectasia. Am J Cardiol. 1976;37(2):217-222.
- Harandi S, Johnston SB, Wood RE, Roberts WC. Operative therapy of coronary arterial aneurysm. Am J Cardiol. 1999;83(8):1290-1293.
- IJsselmuiden A, Verheye S. First report on the use of a novel self-expandable stent for treatment of ST elevation myocardial infarction. Catheter Cardiovasc Interv. 2009;74(6):850-854.
- Finn AV, Joner M, Nakazawa G, et al. Pathological correlates of late drug-eluting stent thrombosis: strut coverage as a marker of endothelialization. Circulation. 2007;115(18):2435-2441.
- Ozaki Y, Okumura M, Ismail TF, et al. The fate of incomplete stent apposition with drug-eluting stents: an optical coherence tomography-based natural history study. Eur Heart J. 2010;31(12):1470-1476.
- Bezerra HG, Costa MA, Guagliumi G, Rollins AM, Simon DI. Intracoronary optical coherence tomography: a comprehensive review clinical and research applications. JACC Cardiovasc Interv. 2009;2(11):1035-1046.
- Nishioka T, Amanullah AM, Luo H, et al. Clinical validation of intravascular ultrasound imaging for assessment of coronary stenosis severity: comparison with stress myocardial perfusion imaging. J Am Coll Cardiol. 1999;33(7):1870-1878.
- Tamburino C, La Manna A, Di Salvo ME, et al. First-in-man 1-year clinical outcomes of the Catania coronary stent system with nanothin polyzene-F in de novo native coronary artery lesions: the ATLANTA (Assessment of The LAtest Non-Thrombogenic Angioplasty stent) trial. JACC Cardiovasc Interv. 2009;2(3):197-204.
______________________________________________
From the 1Division of Cardiology, Ferrarotto Hospital, University of Catania, Catania, Italy, and 2ETNA Foundation, Catania, Italy.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript submitted February 28, 2011, provisional acceptance given March 21, 2011, final version accepted June 3, 2011.
Address for correspondence: Dr. Alessio La Manna, Ospedale Ferrarotto-Alessi, Dipartimento di Cardiologia, 31 Via S.Citelli, 95124 Catania, Italy. Email: lamanna.cardio@gmail.com










