

Sequential Use of Bare-Metal Stents and Drug-Coated Balloons to Treat Coronary Artery Stenosis
Abstract: Introduction. Drug-coated balloons (DCBs) are increasingly used in percutaneous coronary intervention (PCI). The sequential use of DCB and bare-metal stent (BMS) represents a novel approach and results of pilot studies have been encouraging. The aim of this study was to assess long-term outcomes of patients who received treatment with DCB and BMS and additionally study whether the order (BMS or DCB first) affected outcomes. Methods. This is a single-center, non-randomized, prospective study of patients who underwent PCI between July 2009 and July 2011. Two groups were defined: DCB followed by BMS (DCBgBMS) or BMS followed by DCB (BMSgDCB). Our primary outcome was target lesion revascularization (TLR) at 7 months. Results. A total of 128 patients (173 lesions) with a mean age of 67 years were included. The BMSgDCB group consisted of 53 patients (78 lesions) and the DCBgBMS group consisted of 75 patients (95 lesions). The mean follow-up was 7.4 months. The TLR rate was 4/76 (5%) in the BMSgDCB group and 3/90 (3%) in the DCBgBMS group (P=.83). Conclusion. Our study demonstrates good results of sequential BMS and DCB use in an all-comers population. If confirmed by larger studies, this could be a valuable approach in patients with contraindications to drug-eluting stent implantation.
J INVASIVE CARDIOL 2012;24(10):555-559
Key words: drug-coated balloon, bare-metal stent, paclitaxel, percutaneous coronary intervention, target lesion revascularization
____________________________________________________
Stent use has dramatically reduced the rate of angiographic and clinical restenosis and currently they are used in nearly all percutaneous coronary intervention (PCI) procedures.1,2 Drug-eluting stents (DESs) have brought the rate of in-stent restenosis (ISR) down to 3%-20% depending on the lesion in which they are applied,2 but the increased rate of late stent thrombosis (ST) has been a matter of concern for some years. Additionally, the use of DES makes double antiplatelet therapy necessary and can be problematic in patients with a bleeding disorder or those under oral anticoagulation.
Drug-coated balloons (DCBs) have been recently introduced into clinical practice3 and are mainly used for treatment of ISR.4 We recently demonstrated that DCBs are a reasonable alternative for primary use in simple lesions without the need for stent implantation.5 The experience with the combined use of stents and DCBs is limited, but recent studies have demonstrated encouraging results.6 Previous studies have shown that a relatively short duration of contact between the antiproliferative drug and the vessel wall is necessary to prevent ISR.6,7
It is not clear if stent implantation should be followed by DCB treatment or vice versa. As demonstrated previously, application of the drug on the stent surface might worsen endothelialization, which has been identified as one of the main problems of late stent thrombosis.8 One small study with angiographic and optical coherence tomography (OCT) follow-up did not show major differences, except for better stent apposition in those who underwent stent implantation in the first instance.9
The aim of this study was to describe outcomes after sequential use of BMS and DCB and compare whether the strategy of DCB followed by BMS is superior to the strategy of BMS followed by DCB.
Methods
This is a single-center, non-randomized, prospective observational study of patients treated in a tertiary care center in Switzerland (Luzerner Kantonsspital, Luzern).
Patients. All patients undergoing a coronary angiogram for stable coronary artery disease or acute coronary syndrome (ACS) were eligible to be included in this registry. One interventional cardiologist (PE) identified all patients and treated them with one of the two strategies. The included patients were not consecutive, but they represent the broad range of patients treated in our hospital. Patients with cardiogenic shock, previous resuscitation, or left main PCI were not included in this registry. Patients with potential contraindications to long-term double-antiplatelet therapy qualified for a combined treatment of BMS and DCB. The interventions were performed between July 2009 and July 2011.
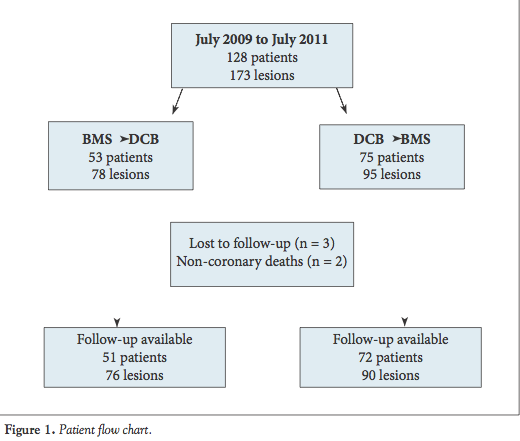 Informed consent was obtained from all patients for data gathering and clinical/telephone follow-up. Treatment strategies. In the BMSgDCB group, the implantation of a BMS was followed by the use of a DCB. In the DCBgBMS group, the lesion was initially treated with a DCB and followed by BMS implantation (Figure 1). Treatment strategy was at the discretion of the operator.
Informed consent was obtained from all patients for data gathering and clinical/telephone follow-up. Treatment strategies. In the BMSgDCB group, the implantation of a BMS was followed by the use of a DCB. In the DCBgBMS group, the lesion was initially treated with a DCB and followed by BMS implantation (Figure 1). Treatment strategy was at the discretion of the operator.
Technical details of PCI. All interventions were performed using the femoral artery approach and 7 Fr catheters. Both predilatation with a non-coated balloon or direct stenting were considered acceptable strategies. The lesion diameter and length were assessed visually. The Pantera Lux (Biotronik) and the InPact (Invatec, Medtronic) were used as DCBs. Both balloons are paclitaxel-coated with a drug concentration of 3.0 µg/mm². The balloons were inflated at nominal pressure for 40 seconds. A new DCB was used for every new lesion. Prokinetic (Biotronik) and Skylor (Invatec) were used as BMSs.
All patients were pretreated with aspirin and a thienopyridine (clopidogrel or prasugrel) and heparin was used for the PCI in all patients.
Outcomes. Patients were followed either by telephone or by planned clinical assessment in an outpatient setting. The follow-up was scheduled with all patients at 6 months, but due to various delays it was completed at 7 months. The telephone interview was performed by a second-year cardiology fellow. A detailed history of current symptoms and any cardiac investigations was performed over the phone. If patients complained of new-onset chest pain or shortness of breath, they were seen in outpatient clinics and then a very low threshold for repeat coronary angiography was applied.
Statistical analysis. Continuous data are expressed as mean ± standard deviation. The prevalence of categorical variables is shown as absolute numbers and percentages. Comparisons between the two groups (BMSgDCB vs DCBgBMS) were performed using two-tailed non-paired t-test for continuous variables and a Chi-squaredχtest for categorical variables. A P-value of <.05 was considered statistically significant.
Results
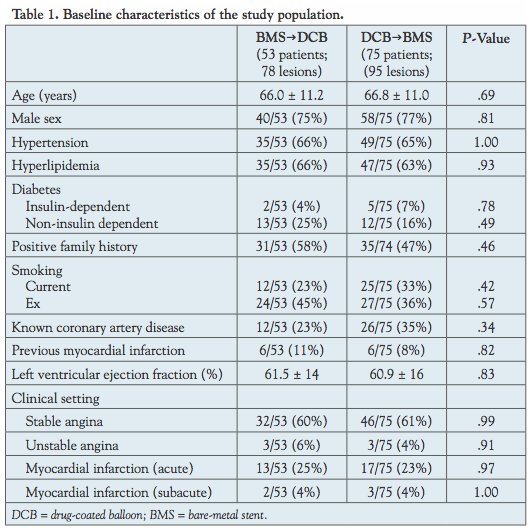 The study population consisted of a total of 128 patients (173 lesions) treated between July 2009 and July 2011. The BMSgDCB group included 53 patients (78 lesions) and the DCBgBMS group included 75 patients (95 lesions). Baseline demographic and clinical characteristics were well-balanced between the two study groups and are summarized in Table 1.
The study population consisted of a total of 128 patients (173 lesions) treated between July 2009 and July 2011. The BMSgDCB group included 53 patients (78 lesions) and the DCBgBMS group included 75 patients (95 lesions). Baseline demographic and clinical characteristics were well-balanced between the two study groups and are summarized in Table 1.
Lesion details are described in Table 2. The angiographic characteristics were well-matched between the two groups, but there were more patients with de novo stenosis in the  BMSgDCB group (97% vs 86%; P=.04) and the reference vessel diameter was greater in the BMSgDCB group (3.2 ± 0.4 mm vs 3.0 ± 0.5 mm; P=.02).
BMSgDCB group (97% vs 86%; P=.04) and the reference vessel diameter was greater in the BMSgDCB group (3.2 ± 0.4 mm vs 3.0 ± 0.5 mm; P=.02).
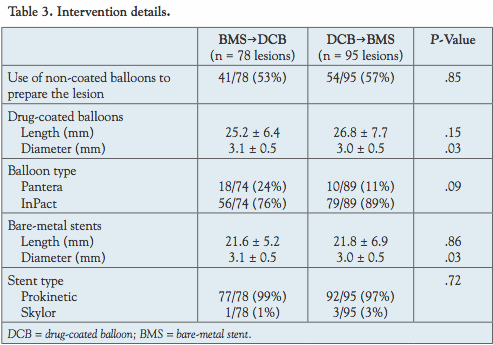
The length of BMS and DCB was comparable between both groups. The diameter of DCB and BMS was larger in the BMSgDCB group (P=.03). The majority of the lesions were pretreated with conventional balloon before DCB or BMS use (53% in BMSgDCB and 57% in DCBgBMS; P=.85) (Table 3).
 Outcomes. Outcomes are summarized in Table 4. The mean follow-up time was similar in both groups (7.5 ± 2.5 months vs 7.2 ± 1.8 months; P=.59).
Outcomes. Outcomes are summarized in Table 4. The mean follow-up time was similar in both groups (7.5 ± 2.5 months vs 7.2 ± 1.8 months; P=.59).
A total of 3 patients (2.3%) were lost to follow-up. One patient (0.8%) sustained a cardiac death (death during percutaneous aortic valve replacement) and 1 patient (0.8%) died of septic shock.
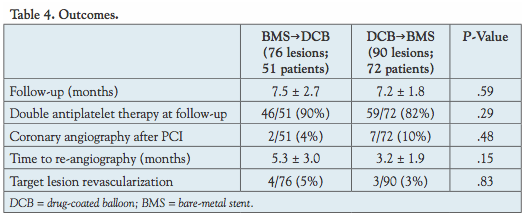 The vast majority of patients were still treated with double antiplatelet therapy at follow-up (Table 4).Repeat coronary angiogram was performed in 2/51 patients (4%) in the BMSgDCB group and in 7/72 patients (10%) in the DCBgBMS group. TLR was performed in 4/76 lesions (5%) in the BMSgDCB group and in 3/90 lesions (3%) in the DCBgBMS group (P=.83).
The vast majority of patients were still treated with double antiplatelet therapy at follow-up (Table 4).Repeat coronary angiogram was performed in 2/51 patients (4%) in the BMSgDCB group and in 7/72 patients (10%) in the DCBgBMS group. TLR was performed in 4/76 lesions (5%) in the BMSgDCB group and in 3/90 lesions (3%) in the DCBgBMS group (P=.83).
The lesion characteristics of the patients with TLR can be seen in Table 5. There were 2 patients and 4 lesions in the BMSgDCB group, and 3 patients and 3 lesions in the DCBgBMS 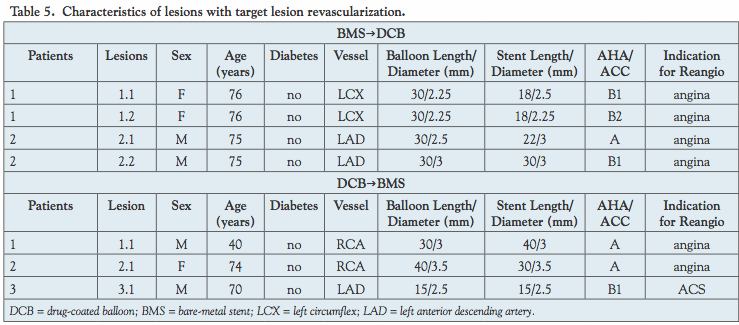 group. None of the patients were diabetic, but they all had rather long lesions (Table 5).
group. None of the patients were diabetic, but they all had rather long lesions (Table 5).
Discussion
This study assessed a novel approach in the percutaneous treatment of coronary artery disease. Our main finding is that the combined use of DCB and BMS is a valuable approach with excellent TLR rates at 7 months.
DCBs have only been introduced in clinical practice in recent years, and have been shown to be effective in the treatment of ISR. A recently published study demonstrated superiority of DCB compared to non-coated balloons in DES restenosis.10 We recently demonstrated that DCBs are a good alternative for the treatment of simple lesions.5 The combined approach sequentially using BMS and DCB is not used routinely and small studies have demonstrated promising results. This is the first study to test this approach in a larger all-comers population.
The rates of TLR (5% in the BMSgDCB group and 3% in the DCBgBMS group) are very good compared to previously published data of BMS ISR11 and DES ISR.12 This finding is even more important in light of the clinical presentation and lesion complexity in our population. More than 30% of the patients had an ACS, 9% of the patients in the DCBgBMS had ISR, calcification was at least moderate in more than half of the population and only 14%-16% of the patients had type A lesions according to the American Heart Association classification.
The absolute number of TLR was 4/76 (5%) in patients with BMSgDCB and 3/90 (3%) in patients with DCBgBMS. Although the difference was not statistically significant (P=.83) due to low patient numbers, this could potentially be an important finding and warrants further investigation. Previous studies have shown that a relatively short duration of contact between the antiproliferative drug and the vessel wall is necessary to prevent ISR.4,13 Applying the antiproliferative drug on the vessel wall seems to offer additional benefits compared to applying the drug on the stent surface. In fact, avoiding the application of the drug on the stent surface might offer a better endothelialization, which has been identified as one of the main problems of late stent thrombosis.8
One recently published study compared DCB + BMS vs BMS vs DES in bifurcation lesions treated with a single-stenting technique. In this study with 6-month angiographic follow-up, DESs showed superior angiographic results compared to DCB and BMS.14 The authors did not find a significant difference in late luminal loss between patients treated with DCB + BMS and those with BMS alone. These findings are in slight contradiction to our results, since the TLR is relatively low in our patients.
However, our reference vessel diameter was 3 mm, indicating that late luminal loss even if apparent angiographically did not reach a clinical significance.
This novel approach remains to be proven effective in larger studies. The concept of abluminal drug coating for DESs is already being used in different stent designs,15,16 and could be a major step forward in avoiding late complications of DES implantation, especially stent thrombosis.
Study limitations. We are presenting the results of a registry and not a prospective randomized trial. Angiographic follow-up and the use of intravascular ultrasound would have been ideal. We cannot exclude that the rate of restenosis was underestimated as we did not have a planned cohort with predefined angiographic follow-up.
Conclusion
The current study demonstrated good outcomes of a combined, sequential approach of DCB and BMS in an unselected population of patients with coronary artery disease. Both approaches using DCB and BMS had very low ISR rates.
The study was too small to draw clear conclusions on which strategy is better. Larger and more comprehensive studies are warranted to clarify the exact role of this novel approach to treat patients with CAD.
References
- Pfisterer M, Nietlispach F, Jeger R, Kaiser C. Drug-eluting coronary stents in clinical practice: lessons from the BAsel Stent Kosten-Effektivitäts Trials (BASKET). A review of the BASKET trials. Swiss Med Wkly. 2011;141:w13263.
- Dangas GD, Claessen BE, Caixeta A, Sanidas EA, Mintz GS, Mehran R. In-stent restenosis in the drug-eluting stent era. J Am Coll Cardiol. 2010;56(23):1897-1907.
- Banning AP, Lim CC. Drug-eluting balloons: what is their place on the interventionalist’s shelf? Heart. 2010;96(16):1257-1258.
- Scheller B, Hehrlein C, Bocksch W, et al. Treatment of coronary in-stent restenosis with a paclitaxel-coated balloon catheter. N Engl J Med. 2006;355(20):2113-2124.
- Cuculi F, Young M, Beeler R, Schoenenberger AW, Erne P. Good efficacy of drug-eluting balloons in a mixed population of patients with coronary artery disease. J Invasive Cardiol. 2012;24(4):151-153.
- Wohrle J, Birkemeyer R, Markovic S, et al. Prospective randomised trial evaluating a paclitaxel-coated balloon in patients treated with endothelial progenitor cell capturing stents for de novo coronary artery disease. Heart. 2011;97(16):1338-1342.
- Speck U, Scheller B, Abramjuk C, Bernhardt U. Drug delivery by angiographic contrast media: inhibition of restenosis. Acad Radiol. 2005;12(Suppl 1):S14-S17.
- Onuma Y, van Beusekom HM, Sorop O, van der Giessen WJ. The paradigm of endothelium and stent thrombosis in DES. EuroIntervention. 2008;4(Suppl C):C17-C21.
- Gutierrez-Chico JL, van Geuns RJ, Koch KT, et al. Paclitaxel-coated balloon in combination with bare-metal stent for treatment of de novo coronary lesions: an optical coherence tomography first-in-human randomised trial, balloon first vs. stent first. EuroIntervention. 2011;7(6):711-722.
- Rittger H, Brachmann J, Sinha AM, et al. A randomized, multicenter, single-blinded trial comparing paclitaxel-coated balloon angioplasty with plain balloon angioplasty in drug-eluting stent restenosis: The PEPCAD-DES study. J Am Coll Cardiol. 2012;59(15):1377-1382.
- Kastrati A, Dirschinger J, Boekstegers P, et al. Influence of stent design on 1-year outcome after coronary stent placement: a randomized comparison of five stent types in 1147 unselected patients. Cathet Cardiovasc Intervent. 2000;50(3):290-297.
- Maluenda G, Ben-Dor I, Gaglia MA Jr, et al. Clinical outcomes and treatment after drug-eluting stent failure: the absence of traditional risk factors for in-stent restenosis. Circ Cardiovasc Interv. 2012;5(1):12-19.
- Scheller B, Speck U, Abramjuk C, Bernhardt U, Bohm M, Nickenig G. Paclitaxel balloon coating, a novel method for prevention and therapy of restenosis. Circulation. 2004;110(7):810-814.
- Stella PR, Belkacemi A, Dubois C, et al. A multicenter randomized comparison of drug-eluting balloon plus bare-metal stent versus bare-metal stent versus drug-eluting stent in bifurcation lesions treated with a single-stenting technique: six-month angiographic and 12-month clinical results of the drug-eluting balloon in bifurcations trial. Cathet Cardiovasc Intervent. 2012 Mar 15 (Epub ahead of print).
- Laborde JC, Borenstein N, Behr L, Ramcharitar S. Stentys coronary bifurcation stent. EuroIntervention. 2007;3:162-165.
- Bege N, Steinmuller SO, Kalinowski M, et al. Drug-eluting stents based on poly(ethylene carbonate): optimization of the stent coating process. Eur J Pharm Biopharm. 2012;80(3):562-570
__________________________________________
From the Department of Cardiology, Luzerner Kantonsspital, Luzern, Switzerland.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript submitted February 21, 2012, provisional acceptance given March 23, 2012, final version accepted May 16, 2012.
Address for correspondence: Prof. Paul Erne, Department of Cardiology, Luzerner Kantonsspital, 6000 Luzern 16, Switzerland. Email: paul.erne@ksl.ch













