Serial Dilation of Low-Profile Stents Delivered in the Aorta and Pulmonary Arteries in Pediatric Patients Leads to Spontaneous Fractures but Not to Adverse Events
Abstract: Objectives. Low-profile stents placed in pediatric patients with congenital heart disease must be expanded by balloon angioplasty to accommodate patient growth. During the process of serial dilation, some stents may spontaneously fracture. The incidence and safety profile of spontaneous fracture is unclear. We report the performance characteristics and safety profile of a cohort of low-profile, premounted stents placed in the pulmonary arteries and aorta and then serially dilated over time to accommodate patient growth, including incidence of fracture and any adverse events. Methods. A retrospective chart review was conducted of 25 pediatric patients who underwent 27 stent placements with low-profile, premounted stents from January 2005 to September 2018. Results. Nine stents (33%) sustained a spontaneous fracture. There was no statistically significant association between stent fracture and our variables of interest, ie, patient gender, patient weight at time of original stenting, stent location (aorta vs pulmonary artery), stent type, original diameter of stent, and weight at the time of stent implantation. There was no association between time to spontaneous fracture and the aforementioned variables of interest. The majority of the spontaneous fractures occurred within the first 4 years after stent implantation, and there was no difference in survival between the 3 stent types investigated in our cohort. Conclusion. One-third of stents undergoing serial dilation for patient growth fractured spontaneously. Patients with fractured stents were free from significant adverse events in this cohort.
Key words: pediatric cardiology, stent fracture
Due to small vessel size, endovascular stent implantation in small pediatric patients requires low-profile stents deliverable through small vascular sheaths (up to a 7 Fr diameter sheath in a vein or a 5 Fr sheath in an artery). These low-profile stents can be serially dilated to accommodate patient growth up to a point, but do not allow for expansion to full adult vessel diameter.1-3 To avoid iatrogenic stenosis as the vessel grows beyond the stent’s maximum expansion diameter, the small stent must either be surgically removed or fractured in the catheterization laboratory.
Throughout the process of serial dilations, but before intentional fracture or surgical excision, some stents fracture spontaneously (meaning they fracture at some point in the outpatient setting and are discovered at subsequent follow-up). However, the reported incidence of spontaneous fracture varies widely.4,5 Additionally, the risks associated with spontaneous stent fracture are not well known. Theoretical concerns include stent collapse leading to partial or full obstruction with hemodynamic compromise, embolization of stent fragments, stent migration, thrombosis, intimal tear, hemorrhage, vessel dissection, or pseudoaneurysm.
The aim of this study is to report the performance characteristics and safety profile of a cohort of low-profile, premounted stents originally delivered through small vascular sheaths (less than 7 Fr in a vein or 5 Fr in an artery) in the aorta or pulmonary artery, then serially dilated for patient growth. We report the incidence of spontaneous stent fracture and any related adverse events, including the theoretical concerns listed above. We also compare the demographic and clinical characteristics of the spontaneous fracture group with those of the non-fracture group.
Methods
We performed a retrospective chart review of pediatric patients who underwent original vessel stenting from January 2005 to September 2018 at the Rady Children’s Hospital catheterization laboratory in San Diego, California. Inclusion criteria were: (1) original stents delivered through a sheath ≤7 Fr in a vein or ≤5 Fr in an artery; (2) stents implanted in the aorta and pulmonary arteries; and (3) stents that underwent at least 1 dilation after original implantation. All data were collected from Rady Children’s Hospital San Diego electronic medical records.
Statistical analysis. To compare demographic and clinical variables of interest for an association with spontaneous fracture, a 2-sample t-test was used for continuous variables and Fisher’s exact test was used for categorical variables. Univariate Cox proportional hazard model was used to assess the relationship of time to spontaneous fracture and the same variables of interest as above. We performed Kaplan-Meier survival analysis to report and visualize the freedom from spontaneous fracture of the stents, which defined spontaneous fracture as the event and considered unfractured stents as censored. We used a log-rank test to determine whether there was a difference between the survival curves for Cook Formula, Genesis, and Visi-Pro stents.
Results
Demographic and clinical variables of interest. A total of 27 stents were implanted in 25 patients. The median age at original stent implantation was 6 months (interquartile range [IQR], 3.3-15.5 months) and median weight was 6.4 kg (IQR 5.6-9.3 kg). A total of 9 stents (33.3%) developed a spontaneous fracture that was subsequently discovered by chest x-ray or fluoroscopy. All spontaneous fractures were circumferential (ie, transverse) and resulted in separation of the original stent into 2 segments that still retained almost all of their original luminal area. That is to say, there was no significant vessel collapse or intimal proliferation after fracture. Additionally, there were no significant hemodynamic or other clinical complications related to the fractures (including no stent migration, thrombosis, intimal tear, hemorrhage, vessel dissection, or pseudoaneurysm at the time of most recent follow-up). In all cases, the stents were expanded beyond the nominal expansion diameter (manufacturer recommendation); in most cases, they were expanded near or to their experimentally reported6 maximum expansion diameters.
There was no statistically significant association between stent fracture and any of the clinical or demographic variables of interest, ie, patient gender, patient weight at time of original stenting, stent location (aorta vs pulmonary artery), stent type, original diameter of stent, and weight at the time of stent placement (Table 1). Univariate Cox proportional hazard model was used to assess the relationship of time to spontaneous fracture and the same variables of interest as above, and there was no statistical association.
We also report more detailed clinical information for each stent in the cohort, including vascular access, an abbreviated patient history, and a description of the interventions undertaken (Tables 2 and 3).
Kaplan-Meier survival analysis and locally weighted scatterplot smoothing (LOWESS) plot. Kaplan-Meier survival analysis for freedom from spontaneous stent fracture demonstrated that most of the spontaneous fractures occurred within the first 4 years after stent implantation, and that there was no significant difference in survival between the 3 stent types in our cohort (Figure 1). Additionally, we report the LOWESS plot with 95% confidence interval (CI) to visualize the relationship of time from the original stent placement (in months) and stent diameter relative to original (Figure 2).
Discussion
Incidence and overall safety of spontaneous fractures. In this study, we report that during the process of growth-related serial dilation of 27 low-profile stents in human subjects, there was a 33.3% incidence of spontaneous circumferential fracture. Notably, there was no significant loss of lumen or vessel collapse, no dissection, and no other significant adverse events arising from these spontaneous fractures. There was no statistically significant difference between the spontaneous fracture group and the non-fracture group for any of the reported demographic and clinical variables of interest.
Our results indicate that the strategy of implanting low-profile stents through small sheaths and serially dilating the vessels for patient growth is relatively safe, even if the incidence of spontaneous circumferential fracture is relatively high. This is important because serial dilation is a crucial part of the broader strategy, leading to eventual intentional stent fracture once a stent has reached its maximum expansion diameter after dilations. So-called “unzipping” (intentional longitudinal fracturing) of stents using high-pressure balloons inflated above the maximum expansion diameter was initially demonstrated for certain types of stents both in vitro and in vivo in piglet models.7,8 More recently, Crystal et al performed a bench study demonstrating that most low-profile stents in the study could be disrupted with high-pressure balloons, and concluded that “serial dilation aiming toward eventual ‘unzipping’ is a legitimate strategy [to match somatic growth] in growing children.”9 Other recent studies demonstrated hemodynamic improvement and a low number of complications and adverse events using similar intentional fracture techniques in humans.10,11
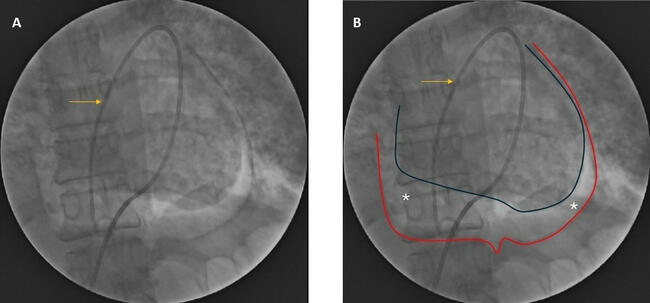
Although those studies examined the efficacy and safety of the unzipping procedure, they did not examine whether or not the requisite serial dilations before intentional fracture resulted in adverse events. Our results suggest that although these serial dilations result in a relatively high incidence of spontaneous fractures, they are free from significant adverse events and therefore should not be a barrier to the overall unzipping strategy. Figure 3 demonstrates detailed imaging of a case with serial dilations, spontaneous fracture, and restenting, all without complications. Furthermore, while serial dilation does lead to a certain number of spontaneous fractures, over time it is theorized to allow for remodeling of the vessel and new intimal tissue formation between dilations, theoretically conferring safety from thrombosis and avoiding uneven expansion, foreshortening, or “napkin-ring” deformations, which are more often seen with a single direct dilation.9,12 Crystal’s findings also suggest that serial dilation confers an advantage if the plan is for eventual intentional fracture after serial dilations, since stents that were not serially dilated were actually less likely to fracture in that bench study.9
Timing and prediction of spontaneous circumferential stent fracture. The relationship between timing of serial dilations and spontaneous stent fracture is still unclear; our Kaplan-Meier analysis showed that most of the stents fractured spontaneously between 15 months and 48 months after original placement, but this analysis does not account for the number or timing of serial dilations in relation to fracture, and our sample size does not have statistical power to test the number or timing of dilations associated with time to fracture. Furthermore, time to fracture was not statistically associated with any of our measured clinical and demographic variables of interest. It is theorized that spontaneous circumferential fractures are the result of torsion and twisting of surrounding tissue, as well as metal fatigue from repetitive forces. This was not tested in all of the in vitro studies, including our group’s recent report,13 and indeed it is very difficult to replicate these theoretical forces in the bench setting. Further study with larger cohorts will be needed to assess that potential association. Nonetheless, it appears that regardless of the rate or incidence of spontaneous fractures, they would not likely be accompanied by an increase in adverse events.
Finally, a set of demographic or clinical variables that are shown to be predictive of which stents are most likely to undergo spontaneous fracture would be helpful clinically, potentially guiding the timing between follow-up, imaging, further catheterizations, etc. Our study did not reveal any such predictive variables.
Study limitations. Detecting small fractures in stents can be difficult by chest x-ray or even by fluoroscopy, so it is possible that we are underestimating the number of spontaneous fractures in the cohort. Additionally, the exact amount of intimal build-up or lumen loss within a fractured stent can be difficult to assess by the conventional methods (angiography), as there is really only an ability to offer qualitative, graded assessments (mild, medium, significant, etc). In 1 case, we performed intravascular ultrasound (IVUS) interrogation of a fractured stent before placing an additional stent, and found only minimal intimal buildup (Figure 4). IVUS has the potential to allow for quantitative analysis of intimal build-up and will be an avenue of further study. Finally, the numbers in our cohort are relatively small and therefore it is difficult to extrapolate for the entire population, as is the case with most pediatric interventional studies.
Conclusion
In our cohort, serial balloon dilation of low-profile stents placed in pediatric patients in the aorta or pulmonary arteries beyond the nominal expansion diameter for patient growth resulted in spontaneous circumferential fractures in 33% of stents; nevertheless, patients with a spontaneous circumferential stent fracture did not experience any significant complications. Clinical and/or demographic factors predicting which stents are more likely to fracture or a more precise timeline for fracture are not well understood. Further study is needed to confirm these initial observations.
From the 1Division of Pediatric Cardiology and 2Department of Pediatrics, Rady Children’s Hospital, University of California San Diego, San Diego, California; and 3UCSD School of Medicine, Department of Family Medicine and Public Health, Division of Biostatistics, UCSD Altman Clinical and Translational Research Institute. All work for this manuscript was performed at Rady Children’s Hospital.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript accepted March 31, 2020.
Address for correspondence: Howaida El-Said, MD, PhD, Department of Pediatrics, Division of Pedatric Cardiology, Rady Children’s Hospital, 3020 Children’s Way, MC 5004, San Diego, CA 92123. Email: helsaid@ucsd.edu
- Mullins CE, O’Laughlin MP, Vick GW, et al. Implantation of balloon-expandable intravascular grafts by catheterization in pulmonary arteries and systemic veins. Circulation. 1988;77:188-199.
- Rosenthal E, Qureshi SA. Stent implantation in congenital heart disease. Br Heart J. 1992;67:211-212.
- O’Laughlin MP, Slack MC, Grifka RG, Perry SB, Lock JE, Mullins CE. Implantation and intermediate-term follow-up of stents in congenital heart disease. Circulation. 1993;88:605-614.
- McElhinney DB, Bergersen L, Marshall AC. In situ fracture of stents implanted for relief of pulmonary arterial stenosis in patients with congenitally malformed hearts. Cardiol Young. 2008;18:405-414.
- Breinholt JP, Nugent AW, Law MA, Justino H, Mullins CE, Ing FF. Stent fractures in congenital heart disease. Catheter Cardiovasc Interv. 2008;72:977-982.
- Bratincsak A, Moore JW, Gulker B, Choules B, Koren L, El-Said HG. Breaking the limit: mechanical characterization of overexpanded balloon expandable stents used in congenital heart disease. Congenit Heart Dis. 2015;10:51-63.
- Sathanandam SK, Haddad LM, Subramanian S, Wright D, Philip R, Waller BR. Unzipping of small diameter stents: an in vitro study: unzipping small diameter stents. Catheter Cardiovasc Interv. 2015;85:249-258.
- Sathanandam SK, Kumar TKS, Hoskoppal D, et al. Feasibility and safety of unzipping small diameter stents in the blood vessels of piglets. JACC Cardiovasc Interv. 2016;9:1138-1149.
- Crystal MA, Morgan GJ, Danon S, et al. Serial versus direct dilation of small diameter stents results in a more predictable and complete intentional transcatheter stent fracture: a PICES Bench Testing Study. Pediatr Cardiol. 2018;39:120-128.
- Morray BH, McElhinney DB, Marshall AC, Porras D. Intentional fracture of maximally dilated balloon-expandable pulmonary artery stents using ultra–high-pressure balloon angioplasty: a preliminary analysis. Circ Cardiovasc Interv. 2016;9:e003281.
- Agrawal H, Qureshi AM, Justino H. Intentional longitudinal and side-cell stent fractures: intermediate term follow-up. Catheter Cardiovasc Interv. 2018;91:1110-1118.
- Danon S, Gray RG, Crystal MA, et al. Expansion characteristics of stents used in congenital heart disease: serial dilation offers improved expansion potential compared to direct dilation: results from a Pediatric Interventional Cardiology Early Career Society (PICES) investigation. Congenit Heart Dis. 2016;11:741-750.
- Bratincsák A, Van Alstine W, Koren L, et al. Intentional fracture of previously placed stents: impact of pre-stenting in a piglet model. J Structural Heart Dis. 2017;3:165-175.