

A Simple Technique to Facilitate Right Heart Catheter Placement From Right Atrium to Right Ventricle: The Virtual Hydraulic Guidewire Technique
Abstract: Right heart catheter advancement from right atrium (RA) to right ventricle (RV) is frequently difficult in patients with large and geometrically deformed RAs. We describe a simple technique, using no additional equipment, that significantly improves the probability of successful passage of right heart catheter from RA to RV.
J INVASIVE CARDIOL 2016;28(2):74-76
Key words: new technique, right heart catheter advancement
_________________________________________
Right heart catheterization is an integral part of hemodynamic assessment of patients in a variety of cardiovascular disease states, especially when non-invasive testing is not able to answer the clinical question conclusively.1 Several access sites are used to enter the venous circulation. While central venous access, either jugular or subclavian, is traditionally used in the intensive care setting, femoral venous access has been the more frequently used access site in the cardiac catheterization laboratory. Due to its benefit of safety,2 upper-extremity venous access is gaining more popularity in the cardiac catheterization laboratory. Typically, once the right heart catheter (RHC) passes proximal to the superior vena cava, simple forward advancement of the catheter allows successful passage from the right atrium (RA) to the right ventricle (RV) and pulmonary artery (PA), assisted by flow, with balloon-tipped catheters. Not infrequently, in patients with large RA dimensions and distorted non-uniform enlargement, advancement of the RHC from RA to RV becomes challenging, requiring guidewire assistance and real-time fluoroscopic guidance, increasing cost and radiation burden. A technique using 1 mL of cold (4 °C) saline injection in the catheter lumen has been described, although it is infrequently used, likely because of lack of immediate availability of cold saline in the catheterization laboratory.3 We describe a simple technique using room-temperature saline bolus injection to facilitate RHC passage from RA to RV.
Case Reports
Case #1. A 78-year-old female was referred for a left and right heart catheterization in view of recurrent heart failure admissions, severe aortic stenosis, and a history of left ventricular systolic dysfunction with biventricular defibrillator implantation. A 6 Fr hydrophilic introducer sheath was placed in the right radial artery. Through a previously placed right antecubital intravenous catheter, a 5 Fr hydrophilic introducer was placed in the vein. A 5 Fr balloon-tipped catheter was advanced through the venous introducer into the basilic vein and placed in the RA without much difficulty. Fifty U/kg unfractionated heparin was given intravenously and 2.5 mg of verapamil was administered in the arterial introducer sheath. Nitroglycerin was withheld in view of echocardiographic evidence of severe aortic stenosis. After obtaining RA pressure recording, the catheter was advanced blindly from 60 cm onward, with an intention to enter the RV. After advancement of a significant length of the catheter, the pressure tracing continued to show RA tracing. Repeat attempts were made with fairly aggressive catheter manipulation, including application of torque, deflation of balloon, and formation of loop-shaped configurations in the RA cavity under fluoroscopic guidance without successful passage from RA to RV. At this point, a 0.025˝ guidewire placement was contemplated. While the staff was bringing the guidewire, the technique described below was used, with prompt passage of the RHC from the RA through the tricuspid valve and into the RV. The rest of the procedure was completed in an uncomplicated and standard fashion.
Case #2. An 81-year-old male presenting with flash pulmonary edema with history of atrial fibrillation and chronic kidney disease was referred for cardiac catheterization. Five Fr right radial artery access was obtained and a hydrophilic introducer sheath was placed. A 5 Fr hydrophilic introducer sheath was placed in the right antecubital vein, and a RHC was advanced via right cephalic vein into the SVC and RA. After recording RA pressure tracing, entry into the RV was difficult. The catheter demonstrated a tendency to either enter the RA appendage or the isthmus area below the tricuspid annulus repeatedly. Once again, fairly persistent efforts to manipulate the catheter under fluoroscopic guidance were unsuccessful. At this point, the technique described below was used with immediate and successful passage of the RHC into the RV.
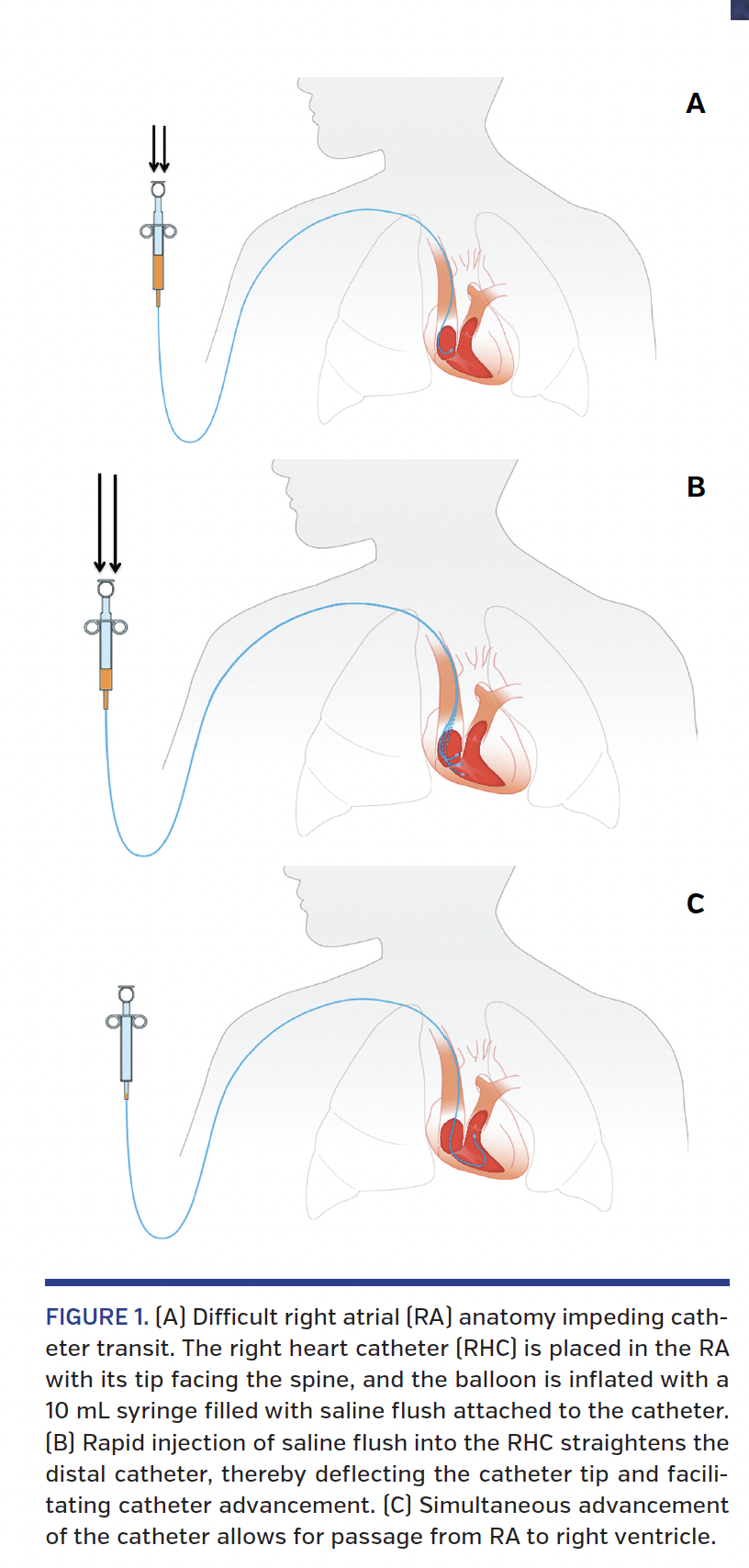
The virtual hydraulic guidewire technique. A 10 or 20 mL syringe (in most cases, the syringe with the manifold) is filled with room-temperature normal saline and attached via luer-lock mechanism to the hub of the RHC. The RHC with the balloon inflated is placed in the RA, with the tip facing the spine, in the vicinity of the presumed tricuspid valve (TV) orifice under fluoroscopic guidance (Figure 1A). A rapid injection of at least 10 mL of saline solution is performed (Figure 1B) and the catheter is simultaneously advanced 5-10 cm. The catheter usually passes into the RV (Figure 1C). The technique is demonstrated in Videos 1A and 1B.
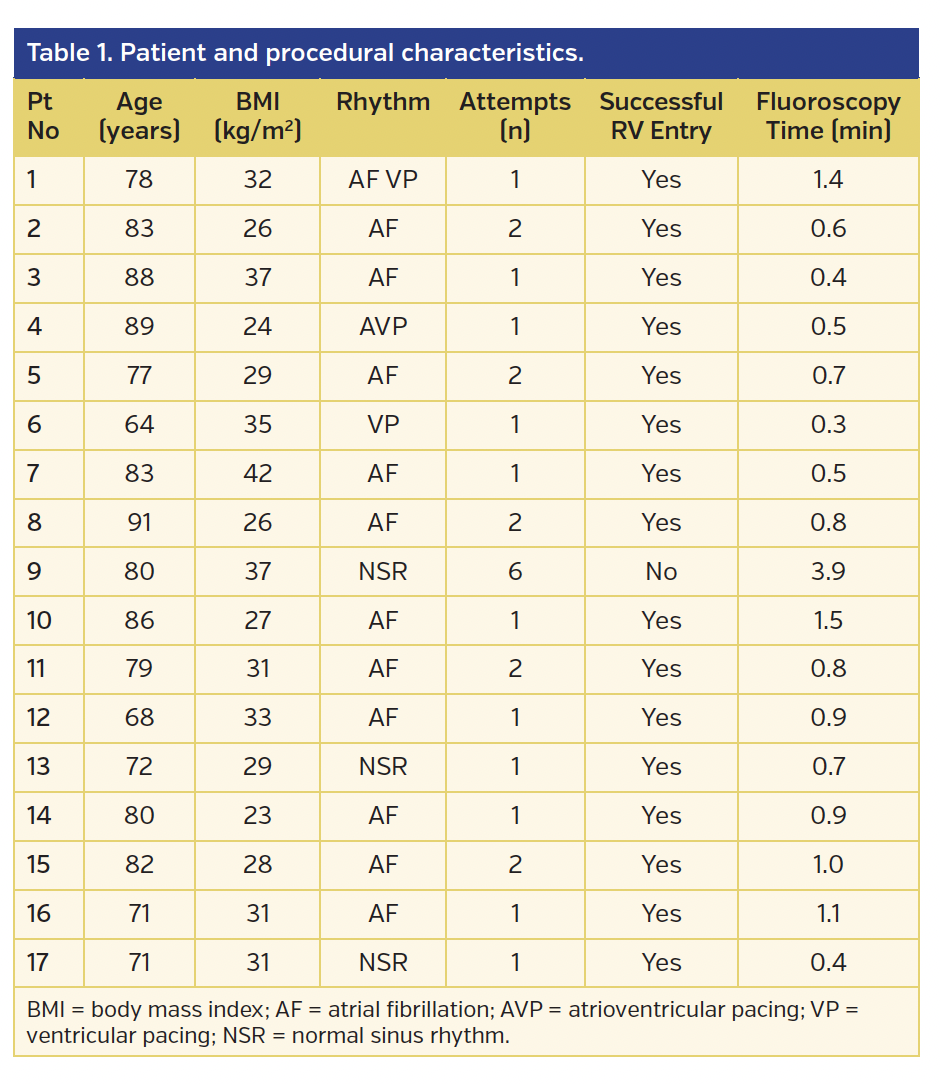
Patient and procedural characteristics of our initial series of 17 patients are detailed in Table 1. Successful passage from RA to RV was achieved in 16 out of 17 patients, with a maximum of two attempts using the virtual hydraulic guidewire technique.
Discussion
Enlargement of cardiac chambers is fairly frequent in a variety of cardiac pathologic conditions, especially in patients with severe valvulopathy and pulmonary hypertension.4 Right heart catheterization in the modern cardiac catheterization laboratory is usually performed in this patient subset. The occurrence of atrial fibrillation (AF) leads to further enlargement of the atria.5 TV inflow, which normally “funnels” blood and catheters into the tricuspid orifice, significantly changes in an enlarged RA, with loss of the truncated conical shape of the inflow. Frequently, due to enlargement of the supraannular and subannular portions of the RA, the tricuspid annular plane migrates inward into the RA cavity, with outpouching of the area around the RA appendage and isthmus. This leads to catheter passage into the pouch-like enlarged paraannular region of the RA, and impedes catheter advancement. This anatomic change, associated with tricuspid regurgitation, further compromises catheter passage to the RV. This is especially a challenge with the smaller-caliber RHCs that are now frequently used. The default technique for facilitation of RHC passage from RA to RV is to use a guidewire to deflect the tip of the RHC and to stiffen the shaft. Our technique, which uses the injection of room-temperature fluid through the catheter shaft, likely achieves these two goals by transiently stiffening the shaft due to increase in pressure in the shaft caused by rapid injection, and the dynamic increase and decrease in stiffness causes a change in the shape of the distal portion of the catheter, hence increasing the probability of finding the TV orifice. This technique does not require any additional equipment or special fluid and hence decreases costs compared with the guidewire-based technique, and is convenient. Although fluoroscopic guidance is a must, the brevity of the technique does not lead to a significant increase in fluoroscopy time. The pressurized injection of fluid into a catheter with its tip embedded in the endocardium holds the risk of potential complications; hence, the balloon must be inflated at the time of injection, and specific attention to this issue is recommended.
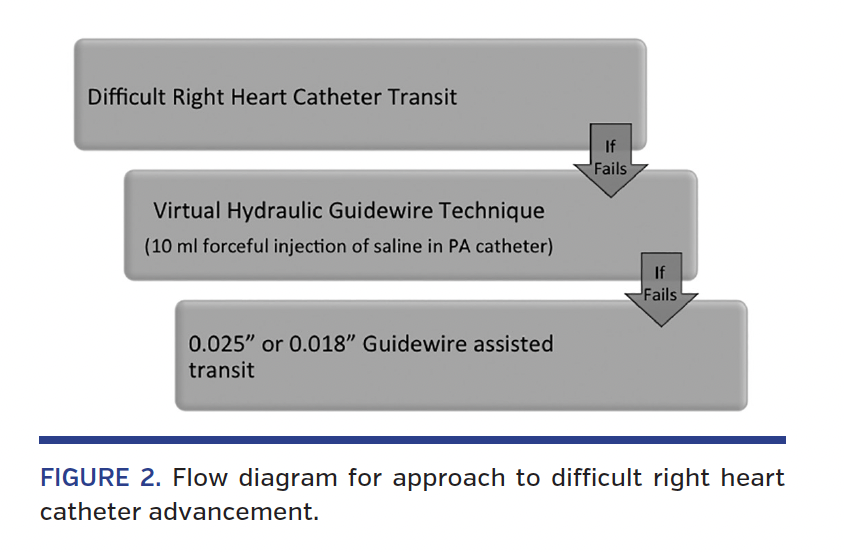
In our case series, this technique succeeded in 16 out of 17 cases and failed in 1 patient despite multiple attempts. In 1 patient, the technique was used successfully to advance the catheter from the RV to the pulmonary artery. The patient in whom the technique failed had a large thoracic aneurysm, and was undergoing preoperative invasive evaluation, with severe distortion of mediastinal anatomy. Several attempts with a 0.025˝ guidewire were also unsuccessful, and a 0.018˝ hydrophilic guidewire was placed in the RV cavity followed by RHC advancement. Our current strategy for difficult RHC procedures is outlined in Figure 2.
Conclusion
RHC passage from RA to RV in difficult cases can be facilitated by rapid injection of room-temperature saline through a balloon-tipped RHC, which acts as a “hydraulic guidewire” and is frequently successful.
References
1. Nishimura RA, Carabello BA. Hemodynamics in the cardiac catheterization laboratory of the 21st century. Circulation. 2012;125:2138-2150.
2. Gilchrist IC. Radial approach to right heart catheterization and intervention. Indian Heart J. 2010;62:245-250.
3. Forrest JB, Todd MH, Cragg DJ. A simple method of percutaneous cannulation of the pulmonary artery in small mammals. Can Anaesth Soc J. 1979;26:58-60.
4. Dauw J, De Meester P, Van de Bruaene A, Gabriels C, Troost E, Budts W. Right heart morphology in elevated pulmonary artery pressure: relationship between echocardiographic and right heart catheterization data. Acta Cardiol. 2014;69:371-375.
5. Sanfilippo AJ, Abascal VM, Sheehan M, et al. Atrial enlargement as a consequence of atrial fibrillation. A prospective echocardiographic study. Circulation. 1990;82:792-797.
____________________________________________
From the 1The Wright Center for Graduate Medical Education, Scranton, Pennsylvania; and 2Apex Heart Institute, Ahmedabad, India.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. Dr Pancholy reports honoraria from the Terumo speaker’s bureau. The remaining authors report no conflicts of interest regarding the content herein.
Manuscript submitted April 8, 2015, provisional acceptance given April 9, 2015, final version accepted June 16, 2015.
Address for correspondence: Samir B. Pancholy, MD, 401 North State Street, Clarks Summit, PA 18411. Email: pancholys@gmail.com











