

Simultaneous Inflation of Two Drug-Eluting Balloons for the Treatment of Coronary Bifurcation Restenosis: A Concept Series
Abstract: Coronary bifurcation restenoses are especially challenging lesions to treat. In this report, four cases are described in which an innovative approach consisting of the simultaneous inflation of two drug-eluting balloons has been successfully applied to treat different kinds of bifurcation restenoses following both provisional and complex stenting strategies. These selected cases illustrate the concept and the advantages of a kissing drug-eluting balloon strategy for the treatment of virtually any kind of bifurcation restenosis.
J INVASIVE CARDIOL 2011;23(11):474-476
Key words: drug-eluting balloons, kissing balloon, coronary bifurcations; restenosis
_________________________________
Percutaneous coronary interventions (PCI) targeting bifurcation lesions are associated with a higher rate of in-stent restenosis than PCI involving less complex lesions.1 The ensuing revascularization procedures might pose real challenges to the interventional cardiologist, for two reasons mainly. First, bifurcation restenoses are most often drug-eluting stent (DES) restenoses, for which optimal treatment is still undefined. Second, depending on the technique adopted during the first PCI, bifurcation restenosis may already present multiple stent layers, or uncovered struts forming a neocarena or jailing the sidebranch, thus worsening geometrical constraints. Therefore, to avoid compromising the main vessel (MV), sidebranch (SB) restenoses are generally not approached percutaneously.
Recently, drug-eluting balloons (DEB) have shown good results in the treatment of both bare-metal stent (BMS) and DES restenosis.2-4 Moreover, several potential benefits are associated with DEB use in bifurcation restenosis, including homogeneous drug transfer to the vessel wall, drug concentration highest at the time of the injury caused by angioplasty, absence of polymer and new metal layer, and respect of the stented bifurcation geometry, provided simultaneous inflation of two DEB (one in the MV and another one in the SB).5 We previously have shown the feasibility of a kissing DEB approach to treat de novo bifurcation lesions.6 In this report, we present four cases of PCI and their angiographic follow-up (FU), selected to illustrate the concept and the advantages of a kissing DEB strategy in the treatment of different kinds of bifurcation restenosis.
Case Reports
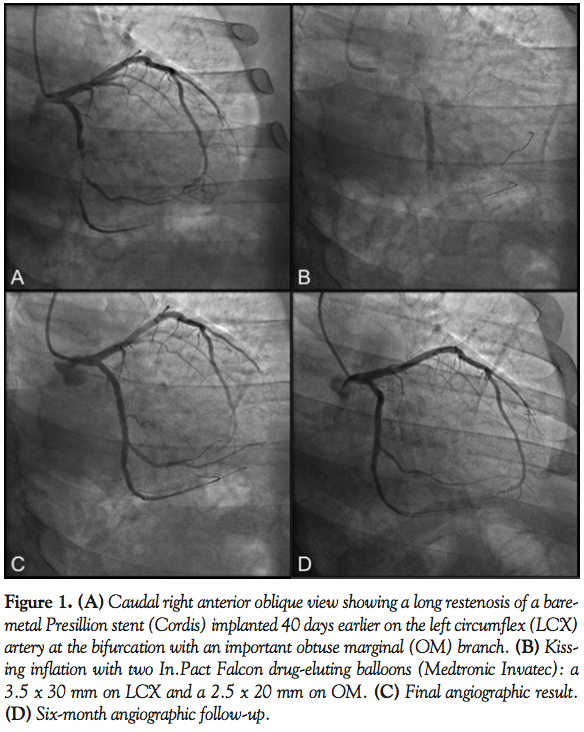 Case 1. A 72-year-old, hypertensive, hypercholesterolemic man was admitted to our institution because of non-ST elevation myocardial infarction occurring 40 days after a 2.75 x 23 mm Presillion BMS (Cordis) was implanted on his left circumflex coronary artery (LCX) jailing an important obtuse marginal branch (OM).
Case 1. A 72-year-old, hypertensive, hypercholesterolemic man was admitted to our institution because of non-ST elevation myocardial infarction occurring 40 days after a 2.75 x 23 mm Presillion BMS (Cordis) was implanted on his left circumflex coronary artery (LCX) jailing an important obtuse marginal branch (OM).
Coronary angiography showed a long subocclusive restenosis on LCX also involving the OM (Figure 1A). The patient underwent PCI. After intravascular-ultrasound guided optimization of the previously implanted stent, kissing balloon was performed (Figure 1B) with two In.Pact Falcon drug-eluting balloons (Medtronic Invatec): a 3.5 x 30 mm on the LCX and a 2.5 x 20 mm on the OM, with a very good final result (Figure 1C) persisting at 6-month angiographic FU (Figure 1D).
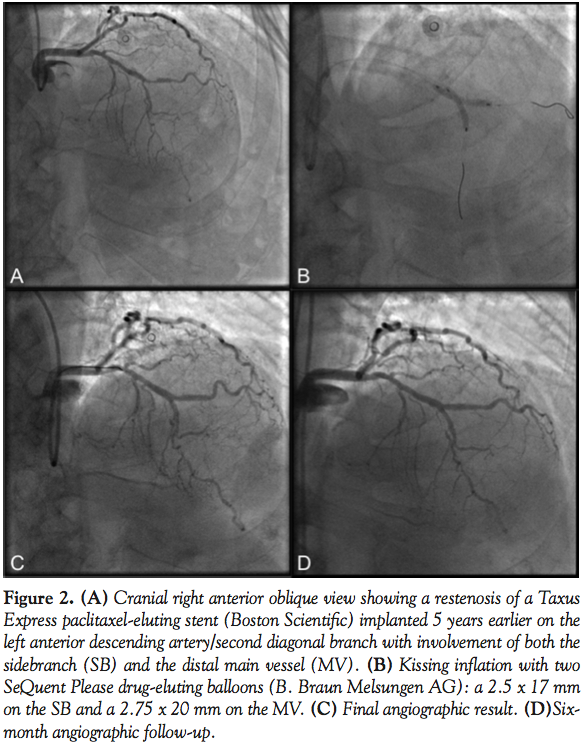 Case 2. A 72-year-old, hypertensive, dyslipidemic man with a family history of cardiovascular disease was referred to our hospital because of effort-induced angina and positive exercise stress myocardial perfusion scintigraphy. Five years earlier, the patient had undergone PCI on his left anterior descending (LAD) coronary artery at the bifurcation with its second diagonal (D2) branch. Since there was a chronic total occlusion of the LAD distal to this bifurcation, a 2.75 x 18 mm paclitaxel-eluting Taxus Express stent (Boston Scientific) was cross-over implanted on the D2, assumed to be the distal MV.
Case 2. A 72-year-old, hypertensive, dyslipidemic man with a family history of cardiovascular disease was referred to our hospital because of effort-induced angina and positive exercise stress myocardial perfusion scintigraphy. Five years earlier, the patient had undergone PCI on his left anterior descending (LAD) coronary artery at the bifurcation with its second diagonal (D2) branch. Since there was a chronic total occlusion of the LAD distal to this bifurcation, a 2.75 x 18 mm paclitaxel-eluting Taxus Express stent (Boston Scientific) was cross-over implanted on the D2, assumed to be the distal MV.
In our cath lab, coronary angiography showed diffuse LAD disease with a critical in-stent restenosis on LAD-D2 and a critical stenosis on the SB ostium (Figure 2A). The diagnostic procedure was continued by PCI: after optimal preparation of the lesion, a kissing-balloon was performed (Figure 2B) with a 2.75 x 20 mm and a 2.5 x 17 mm paclitaxel-coated SeQuent Please DEB (B. Braun Melsungen AG) implanted on the MV and the SB, respectively. The result was very nice (Figure 2C) and proved to be essentially unchanged at 6-month FU (Figure 2D).
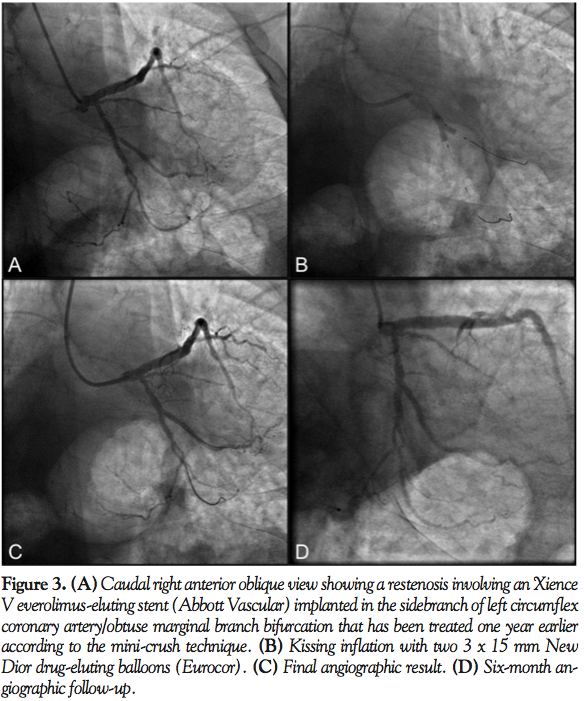 Case 3. A 67-year-old man with a history of hypertension and hypercholesterolemia was admitted to our institution because of effort angina and positive exercise stress test. One year earlier, the patient underwent PCI on LCX at the bifurcation with an important OM with two everolimus-eluting Xience V stents (Abbott Vascular): a 3 x 15 mm on the LCX and a 2.5 x 18 mm on the OM1 implanted according to the mini-crush technique.
Case 3. A 67-year-old man with a history of hypertension and hypercholesterolemia was admitted to our institution because of effort angina and positive exercise stress test. One year earlier, the patient underwent PCI on LCX at the bifurcation with an important OM with two everolimus-eluting Xience V stents (Abbott Vascular): a 3 x 15 mm on the LCX and a 2.5 x 18 mm on the OM1 implanted according to the mini-crush technique.
The day after admission, coronary angiography revealed critical in-stent restenosis involving the ostium of the OM (Figure 3A) and a PCI was performed: after optimal preparation, kissing-balloon was easily done (Figure 3B) with two 3 x 15 mm New Dior DEB (Eurocor), yielding an excellent final result (Figure 3C) that persisted at 6-month angiographic FU (Figure 3D).
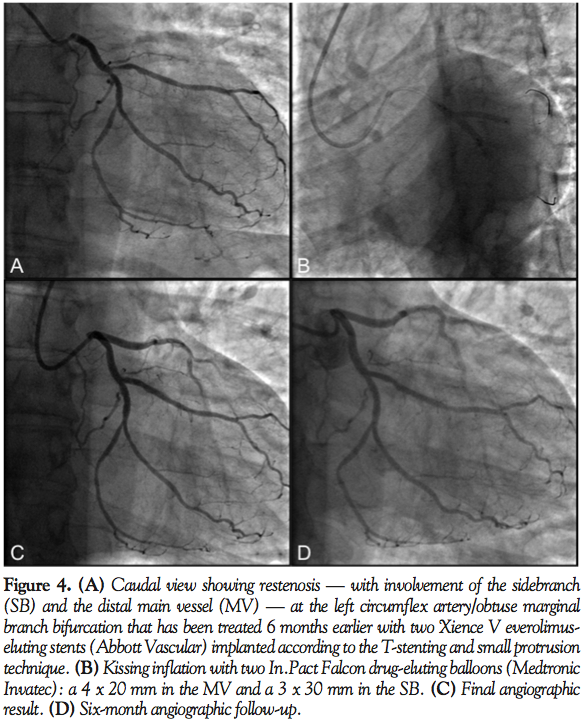 Case 4. A 65-year-old man with a history of hypertension and type II diabetes mellitus was referred to our unit because of a restenosis at the LCX-OM bifurcation pointed out by a coronary CT that was performed as a screening test prior to surgical repair of an abdominal aortic aneurysm. Six months earlier, the patient underwent a PCI with two everolimus-eluting Xience V stents implanted according to the T-stenting and small protrusion (TAP) technique: a 3 x 23 mm on the MV and a 2.5 x 12 mm on the SB.
Case 4. A 65-year-old man with a history of hypertension and type II diabetes mellitus was referred to our unit because of a restenosis at the LCX-OM bifurcation pointed out by a coronary CT that was performed as a screening test prior to surgical repair of an abdominal aortic aneurysm. Six months earlier, the patient underwent a PCI with two everolimus-eluting Xience V stents implanted according to the T-stenting and small protrusion (TAP) technique: a 3 x 23 mm on the MV and a 2.5 x 12 mm on the SB.
Coronary angiography confirmed restenosis of the SB that also involved the distal MV (Figure 4A). After careful preparation of the lesion, a kissing DEB (Figure 4B) was performed with two In.Pact Falcon DEBs: a 4 x 20 mm in the MV and a 3 x 30 mm in the SB with a very good result (Figure 4C) that persisted at 5-month FU (Figure 4D).
Discussion
In this report, we describe an innovative approach to the treatment of bifurcation restenosis consisting in the simultaneous kissing inflation of two DEBs, one in the MV and another in the SB. This strategy appears suitable in every pattern of lesion following different bifurcation-specific stenting techniques. Indeed, the possibility of a mechanical dilatation of the lesion coupled to the concurrent drug transfer to the vessel wall is extremely appealing in this challenging setting.
In the first described case, an early restenosis of a BMS involved the whole stented segment on the MV as well as the proximal tract of the SB. The current approach to this kind of lesion would consist of placing a DES inside the previously implanted BMS,7 thus ensuring optimal result on the MV. However, this strategy implies a second metallic layer that would potentially jeopardize the SB, especially if final kissing balloon was not performed during the first PCI. The second case shows bifurcation restenosis following a provisional approach with DES. Implantation of a new DES presents the same limitation as in the first case, but also the uncertainties related to the treatment of DES restenosis.8 Indeed, the optimal treatment of DES restenosis among conventional balloon angioplasty, cutting or scoring balloon, same or different DES, and excimer laser angioplasty is still undetermined.
The third and fourth cases describe a bifurcation restenosis with exclusive SB involvement following a PCI in which a complex strategy has been implemented. In such circumstances, the insertion of a new metallic layer might represent a real issue, because of the presence of multiple stent layers as in the cullote technique or crush techniques and its derivatives, or a neocarena as in the kissing stent or TAP. Despite implementation of a more complex technique aiming at an optimal result on the SB, restenoses involving the SB are paradoxically only treated quite seldom, as reflected by the striking difference between the incidence of SB binary restenosis and the rate of target lesion revascularization observed in major bifurcation trials.9 The main advantages of DEB use in bifurcation are linked to the effectiveness of drug transfer to the vessel wall without the need of a new metallic layer or polymer, thus perfectly respecting the bifurcation geometry and allowing a safe and effective treatment of isolated SB restenosis, as in the last two cases, or dedicated bifurcation stent restenosis. However, the simultaneous inflation of two DEBs has to be pursued to avoid major geometrical distortion of the previously implanted stent(s).5 Moreover, the need for only 3 months of dual antiplatelet therapy is particularly relevant in circumstances not allowing for a longer duration.
Overall, the kissing-DEB approach appears a very straightforward procedure for the treatment of virtually any kind of bifurcation restenosis.
References
- Al Suwaidi J, Berger PB, Rihal CS, et al. Immediate and long-term outcome of intracoronary stent implantation for true bifurcation lesions. J Am Coll Cardiol. 2000;35(4):929-936.
- Scheller B, Hehrlein C, Bocksch W, et al. Treatment of coronary in-stent restenosis with a paclitaxel-coated balloon catheter. N Engl J Med. 2006;355(20):2113-2124. Epub 2006 Nov 13.
- Unverdorben M, Vallbracht C, Cremers B, et al. Paclitaxel-coated balloon catheter versus paclitaxel-coated stent for the treatment of coronary in-stent restenosis. Circulation. 2009;119(23):2986-2994. Epub 2009 Jun 1.
- Habara S, Mitsudo K, Kadota K, et al. Effectiveness of paclitaxel-eluting balloon catheter in patients with sirolimus-eluting stent restenosis. JACC Cardiovasc Interv. 2011;4(2):149-154.
- Ormiston JA, Webster MW, El Jack S, et al. Drug-eluting stents for coronary bifurcations: bench testing of provisional sidebranch strategies. Catheter Cardiovasc Interv. 2006;67(1):49-55.
- Sgueglia GA, Todaro D, Bisciglia A, Conte M, Stipo A, Pucci E. Kissing inflation is feasible with all second-generation drug-eluting balloons. Cardiovasc Revasc Med. 2011;12(5):280-285. Epub 2011 Jan 26.
- Kastrati A, Mehilli J, von Beckerath N, et al. Sirolimus-eluting stent or paclitaxel-eluting stent vs balloon angioplasty for prevention of recurrences in patients with coronary in-stent restenosis: a randomized controlled trial. JAMA. 2005;293(2):165-171.
- Dangas GD, Claessen BE, Caixeta A, Sanidas EA, Mintz GS, Mehran R. In-stent restenosis in the drug-eluting stent era. J Am Coll Cardiol. 2010;56(23):1897-1907.
- Hakeem A, Khan FM, Bhatti S, et al. Provisional vs complex stenting strategy for coronary bifurcation lesions: meta-analysis of randomized trials. J Invasive Cardiol. 2009;21(11):589-595.
_________________________________
From Ospedale Santa Maria Goretti, Latina, Italy.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript submitted June 22, 2011 and accepted July 25, 2011.
Address for correspondence: Gregory A. Sgueglia, MD, PhD, Ospedale Santa Maria Goretti, UOC Emodinamica e Cardiologia Interventistica via Canova, 3, Latina, 04100, Italy. Email: g.a.sgueglia@gmail.com










