

Simultaneous Transradial Coronary Angioplasty and Contralateral Coronary Angiography With a Single Guide Catheter for Total Coronary Occlusions
Abstract: Objective. In order to prevent double arterial access for contralateral angiography for percutaneous coronary intervention (PCI) of occluded coronary arteries, a new technique is under development, requiring only one puncture site and one guide catheter (1P1G). Background. Percutaneous intervention for coronary artery occlusions frequently requires visualization of the segment distal to the occlusion via contralateral coronary angiography. This technique requires the use of two catheters and two entry sites. The use of two entry sites increases the risk for entry-site complications and is uncomfortable to the patient. Methods. Careful rotation of a transradial multipurpose guide allows contralateral angiography while a guidewire is maintained in the occluded coronary artery. Results. This report describes 3 patients with successful contralateral angiography with the same guide as used for PCI. Conclusion. Visualizing the contralateral artery with the same guide that is simultaneously used for angioplasty of the occluded coronary artery is feasible.
J INVASIVE CARDIOL 2014;26(2):87-90
Key words: transradial approach, coronary occlusion, percutaneous coronary intervention
__________________________
In order to assess proper intraluminal wire position during percutaneous coronary intervention (PCI) for coronary occlusions, simultaneous contralateral coronary angiography is mandatory.1 Traditionally, this requires two arterial entry sites and two catheters. However, two entry sites and two catheters result in double the risk for entry-site complications, potential risk for radial artery occlusions if two radial arteries are used, need for closure devices if one or two femoral arteries are used, and discomfort to the patient.
Transradial approach for PCI of chronic total occlusion (CTO) with 6 Fr guides (or smaller) is feasible, with high success rates.2,3 With this approach, the risks and inconveniences of double arterial access are minimized, but not absent.4 In order to overcome the limitations of double arterial access, we examined the possibility of visualizing the contralateral coronary artery (CLA) by transradial approach with a multipurpose catheter while a coronary guidewire remained advanced in or beyond the occluded segment of the occluded target artery.
Case Descriptions
Patient #1. A 44-year-old male patient was referred for PCI of a CTO of the left anterior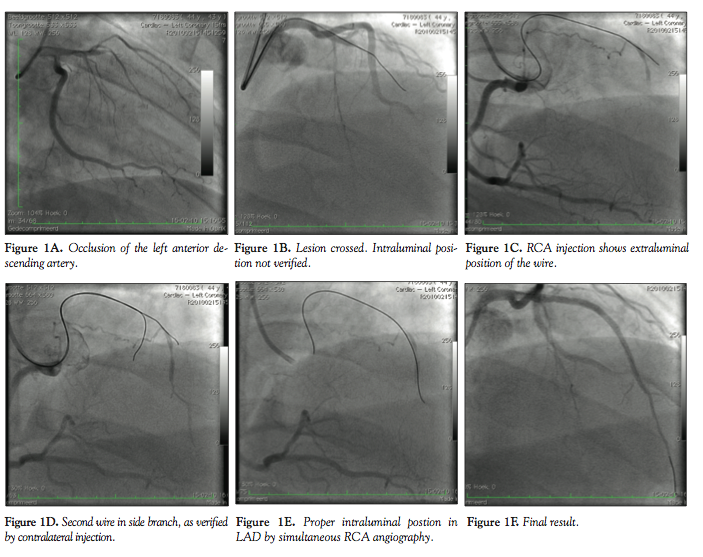 descending (LAD) artery because of stable angina pectoris. The LAD was proximally occluded (Figure 1A) and there was good retrograde filling via collaterals from the right coronary artery (RCA). PCI was performed via the right radial approach (RRA) with a 6 Fr Kimny guide (Boston Scientific). An Asahi Miracle 3 guidewire was advanced to a point distal to the occlusion. However, intraluminal position was not evident (Figure 1B). By carefully rotating the catheter to the RCA, the RCA could be cannulated and filmed, which showed extraluminal position of the wire (Figure 1C). A second Asahi Miracle 3 wire was advanced after recannulation of the left coronary artery. By the same technique, it became evident that the tip of this wire was positioned in a small side branch (Figure 1D). A third attempt with an Asahi Miracle 6 wire resulted in an intraluminal position of the wire (Figure 1E), after which predilatation was performed and 3 drug-eluting stents were placed. The final result was good (Figure 1F).
descending (LAD) artery because of stable angina pectoris. The LAD was proximally occluded (Figure 1A) and there was good retrograde filling via collaterals from the right coronary artery (RCA). PCI was performed via the right radial approach (RRA) with a 6 Fr Kimny guide (Boston Scientific). An Asahi Miracle 3 guidewire was advanced to a point distal to the occlusion. However, intraluminal position was not evident (Figure 1B). By carefully rotating the catheter to the RCA, the RCA could be cannulated and filmed, which showed extraluminal position of the wire (Figure 1C). A second Asahi Miracle 3 wire was advanced after recannulation of the left coronary artery. By the same technique, it became evident that the tip of this wire was positioned in a small side branch (Figure 1D). A third attempt with an Asahi Miracle 6 wire resulted in an intraluminal position of the wire (Figure 1E), after which predilatation was performed and 3 drug-eluting stents were placed. The final result was good (Figure 1F).
Patient #2. A 56-year-old male patient was admitted for PCI of a CTO of the proximal left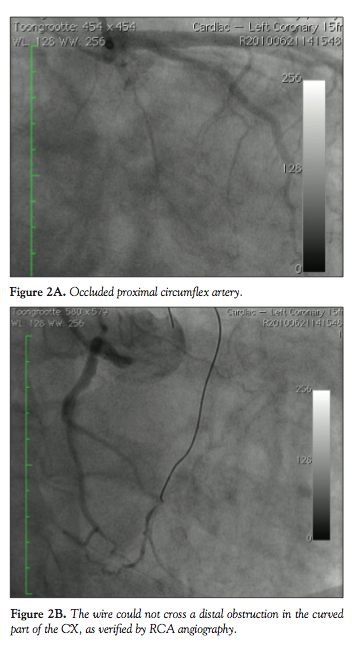 circumflex (CX) coronary artery (Figure 2A). The distal CX was collaterally filled by the RCA. PCI was performed via RRA with a 6 Fr Kimny guide. Multiple attempts to cross the lesions with several wires (Asahi Miracle 3, Miracle 6 and Confianza) failed. Contralateral injections of the RCA showed that the tip of the wire could not cross the very distal part of the long occlusion (Figure 2B). Attempts to perforate the occlusion by increasing support with a Finecross and with a 1 mm over-the-wire balloon also failed.
circumflex (CX) coronary artery (Figure 2A). The distal CX was collaterally filled by the RCA. PCI was performed via RRA with a 6 Fr Kimny guide. Multiple attempts to cross the lesions with several wires (Asahi Miracle 3, Miracle 6 and Confianza) failed. Contralateral injections of the RCA showed that the tip of the wire could not cross the very distal part of the long occlusion (Figure 2B). Attempts to perforate the occlusion by increasing support with a Finecross and with a 1 mm over-the-wire balloon also failed.
Patient #3. A 69-year-old man was referred for PCI of a recent occlusion of the RCA (Figure 3A). PCI was performed via RRA with a 6 Fr Kimny guide. A Runthrough coronary guidewire (Biotronik) easily crossed the lesion. Proper position of the wire was verified by LCA injection with the same catheter (Figure 3B). A good result was obtained after predilatation and placement of a drug-eluting stent (Figure 3C).
Technique
Several catheters are suitable for transradial intervention (TRI) of both the RCA and LCA. The first multipurpose catheter designed for transradial coronary angioplasty was the Kimny catheter. Other examples of multipurpose curves for TRI are the Barbeau (Cordis) and Ikari (Terumo). Conventional “femoral” curves are also suitable for multipurpose use (for example, Judkins Left 3.5, Amplatz Left 1, Multipurpose). In all cases, manipulating the catheter from one side to the other has to be performed with care in order to prevent tip dissections or inadvertent and uncontrolled deep intubation.
A multipurpose catheter is turned from LCA to RCA by clockwise rotation while the catheter is gently pushed to the right coronary sinus. Turning the catheter from RCA to LCA is achieved by counter-clockwise rotation of the guide while the catheter is gently pulled to the left coronary sinus.
A coronary guidewire that has crossed a CTO partially or completely is relatively “anchored” in the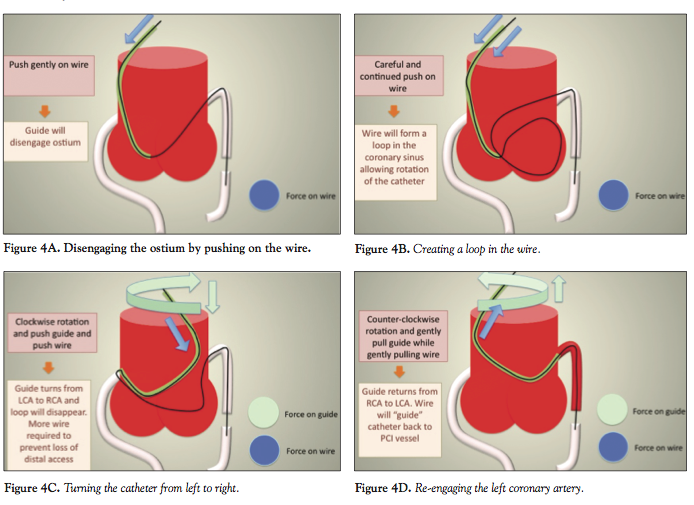 occluded segment. Pushing the guidewire results in forward directed force and stabilization of the wire in the occluded segment (Figure 4A). Pushing excessively also results in disengagement of the guide from the coronary artery. In addition, this results in the creation of a loop of the wire in the coronary sinus and ascending aorta (Figure 4B). This looped wire allows the catheter to be turned toward the contralateral artery without disengagement of the wire (Figure 4C). On the way to the LCA, the catheter needs to be pulled back in a counter-clockwise fashion with slight pull on the guidewire (Figure 4D).
occluded segment. Pushing the guidewire results in forward directed force and stabilization of the wire in the occluded segment (Figure 4A). Pushing excessively also results in disengagement of the guide from the coronary artery. In addition, this results in the creation of a loop of the wire in the coronary sinus and ascending aorta (Figure 4B). This looped wire allows the catheter to be turned toward the contralateral artery without disengagement of the wire (Figure 4C). On the way to the LCA, the catheter needs to be pulled back in a counter-clockwise fashion with slight pull on the guidewire (Figure 4D).
For rotation from the RCA to the LCA, first pushing the wire will result in disengagement from the catheter out of the ostium of the RCA and in loop formation. Then, while pulling gently under careful counter-clockwise rotation, the left coronary sinus can be reached. The way back to the RCA requires slight pull on the wire and clockwise rotation while pushing gently on the guide.
Discussion
This unique experience, which has not been described before, shows that it is possible to visualize the contralateral coronary artery, filling the occluded segment of the target coronary artery subject to PCI, with the catheter used for PCI while maintaining distal access with the coronary guidewire in the target vessel. There is, of course, a risk for loss of distal wire access by uncontrolled dislodgment or rotation of the catheter tip. Loss of distal wire access can occur if the tip of the catheter makes a fast and uncontrolled rotation toward the contralateral side and during difficulties in reaching the opposite coronary sinus. This can be prevented by performing a contralateral angiogram just before a guidewire is advanced in the occluded coronary artery. If this is impossible or very cumbersome, a more suitable catheter should be selected or it should be decided not to perform this maneuver. With further refinement of the procedure and materials, and with increasing experience, this risk might diminish. Perhaps use of more flexible catheters (5 Fr) can overcome this problem.
The advantages of this technique are obvious. Only one puncture site is required, increasing safety of the procedure by minimizing additional risk for arterial bleeding. This technique is much more comfortable for the patient as well. Cost is also reduced because fewer catheters, pressure lines, and hemostasis devices are used.
However, this approach has not been validated by other interventional cardiologists. The technique has not been applied in patients with abnormal ostia of LCA and RCA or in patients with a dilated aortic root. As discussed, the risk of loss of distal access during catheter manipulations is certainly present. This, of course, should be prevented because it impairs procedural success and prolongs the procedure. Therefore, this approach must be performed with meticulous care and catheter handling. The operator should be familiar not only with the characteristics and the performance of the guide catheter used, but also with TRI and PCI for CTO. This certainly is not a technique for operators in their early phase of development.
In experienced hands, however, this technique makes (antegrade) treatment of a CTO less complex. The wider applicability of this approach needs to be validated and the possible offset of losing distal antegrade wire access and thus reduced procedural success needs further evaluation.
References
- Weisz G, Moses JW. Contemporary principles of coronary chronic total occlusion recanalization. Catheter Cardiovasc Interv. 2010;75(S1):S21-S27
- Rathore S, Hakeem A, Pauriah M, Roberts E, Beaumont A, Morris JL. A comparison of the transradial and the transfemoral approach in chronic total occlusion percutaneous coronary intervention. Catheter Cardiovasc Interv. 2009;73(7):883-887.
- Yu CW, Gwon H-Y, Chun WJ, et al. The feasibility of 5-French transradial coronary intervention, as compared with a 6-French approach, for treating chronic total occlusion. Korean Circ J. 2007;37:298-303.
- Jolly SS, Amlani S, Hamon M, et al. Radial versus femoral access for coronary angiography or intervention and the impact on major bleeding and ischemic events: a systematic review and meta-analysis of randomized trials. Am Heart J. 2009;157(1):132-140.
From the Department of Cardiology, Tergooi Blaricum, The Netherlands.
Disclosure: The author has completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. He reports no conflicts of interest regarding the content herein.
Manuscript submitted August 13, 2013 and accepted September 9, 2013.
Address for correspondence: F. Kiemeneij, MD, PhD, Back Office Interventional Cardiology, Tergooi Blaricum, Rijksstraatweg 1, 1261 AN Blaricum, The Netherlands. Email: fkiemeneij@tergooi.nl











