

Successful Angioplasty of Anomalous Coronary Arteries With Total Occlusions
ABSTRACT: We present 2 cases of successful angioplasty of anomalous coronary arteries with total occlusions. One of our patients had a chronic total occlusion of the right coronary artery and the other had acute total occlusion of the left anterior descending artery with special focus on optimal guide catheter selection.
J INVASIVE CARDIOL 2012;24(10):E228-E232
____________________________________________________
The incidence rate for isolated congenital coronary anomalies is 1% of the general population and right coronary artery (RCA) anomalies account for 0.09% of cases.1 The anomalous RCA located posteriorly high near the left sinus of Valsalva is a very uncommon and technically difficult vessel to cannulate, and to perform interventions.2,3 The abnormal position of the anomalous ostium requires better guiding catheter support compared to the normally located RCA. Several published case studies have described the technical difficulties associated with balloon angioplasty and stenting of anomalous right coronary artery.5-11 However there are very few successful reports involving angioplasty of total occlusion in an anomalous RCA using various techniques.12-15 In this report, we describe 2 patients with anomalous origin of RCA and left anterior descending artery (LAD) and having total occlusion to intervene. Successful stent deployment was eventually performed using an on-table modified 7 Fr Amplatzer 1 guiding catheter, which provided adequate support during the difficult intervention in the first case. In the second case, a patient with acute myocardial infarction (MI) and total occlusion of a separate origin of the LAD was engaged with a standard 7 Fr Judkins Left 4 guiding catheter.
 Case Report 1. A 34-year-old male presented with past history of chronic smoking, alcohol abuse, intermittent angina for 4 months, and significant chest pain 3-4 months prior. ECG revealed old inferior wall MI and mild hypokinesia of the inferior wall with preserved wall thickness and minimal scarring and ejection fraction of 50% (Simpson’s method). Coronary angiogram of the left system revealed insignificant stenosis in the LAD. After several unsuccessful attempts to locate the RCA with standard right catheters, an aortic root shoot was taken. This revealed anomalous RCA originating from left posterior side of midline of aortic root Type D anomalous RCA by Sarkar et al classification.16 Successful cannulation was done with a 6 Fr Amplatzer II diagnostic catheter and the anomalous RCA had total occlusion in the proximal mid junction (Figure 1). Coronary angioplasty was attempted later using a 7 Fr Hockey stick, Amplatzer I, EBU 3.5, Judkins Left 3.5, Multipurpose Amplatzer II, and Amplatzer II guiding catheters without success. We were able to cannulate successfully with AR 2 guiding catheter but due to lack of support during any attempt to cross the lesion with standard chronic total occlusion (CTO) guide wires, the whole guiding system backed off. The procedure was abandoned as during the attempts ≥ 400 mL of contrast was used and procedure time exceeded more than 3 hours.
Case Report 1. A 34-year-old male presented with past history of chronic smoking, alcohol abuse, intermittent angina for 4 months, and significant chest pain 3-4 months prior. ECG revealed old inferior wall MI and mild hypokinesia of the inferior wall with preserved wall thickness and minimal scarring and ejection fraction of 50% (Simpson’s method). Coronary angiogram of the left system revealed insignificant stenosis in the LAD. After several unsuccessful attempts to locate the RCA with standard right catheters, an aortic root shoot was taken. This revealed anomalous RCA originating from left posterior side of midline of aortic root Type D anomalous RCA by Sarkar et al classification.16 Successful cannulation was done with a 6 Fr Amplatzer II diagnostic catheter and the anomalous RCA had total occlusion in the proximal mid junction (Figure 1). Coronary angioplasty was attempted later using a 7 Fr Hockey stick, Amplatzer I, EBU 3.5, Judkins Left 3.5, Multipurpose Amplatzer II, and Amplatzer II guiding catheters without success. We were able to cannulate successfully with AR 2 guiding catheter but due to lack of support during any attempt to cross the lesion with standard chronic total occlusion (CTO) guide wires, the whole guiding system backed off. The procedure was abandoned as during the attempts ≥ 400 mL of contrast was used and procedure time exceeded more than 3 hours.
We concluded that only Amplatzer catheters would give enough support to cross the total occlusion of this anomalous RCA. We took a standard Amplatzer I guiding catheter and modified it suitably based upon the aortic root angiogram measurements. The catheter was kept in warm water for 15 minutes with both primary and secondary curves modified and then immediately dipped in cold water. The primary curve was modified to make it more coaxially aligned to anomalous RCA and the secondary curve made wider and deeper so that its transverse diameter traverses the 2 opposite walls of the aorta with enough depth to reach the bottom of the aortic cusps. With this modified guide catheter, the RCA was able to cannulate easily and provided enough backup support for further attempts to cross the total occlusion. Initially the 0.014-inch HT Whisper Extra Support wire (Abbott Vascular) was used to cross the lesion but it went into false lumen and offered lot of resistance to wire advancement. We exchanged it with an intermediate wire, 0.014-inch BMW HT wire (Abbott Vascular) along with 1.2 mm x 10 mm Sprinter Rapid Exchange Balloon catheter support (Medtronic). With the guide catheter providing enough support this time, the total occlusion was successfully crossed and multiple predilatations were given initially with the same balloon and later with another 2.0 mm x 10 mm Sprinter Balloon (Medtronic). The proximal lesion was covered with a 3.0 mm x 27 mm Lekton Motion stent (Biotronik) deployed at 16 atm and the distal lesion was covered with the 2.75 mm x 30 mm Lekton Motion stent (Biotronik) at 18 atm. We achieved excellent angiographic result.
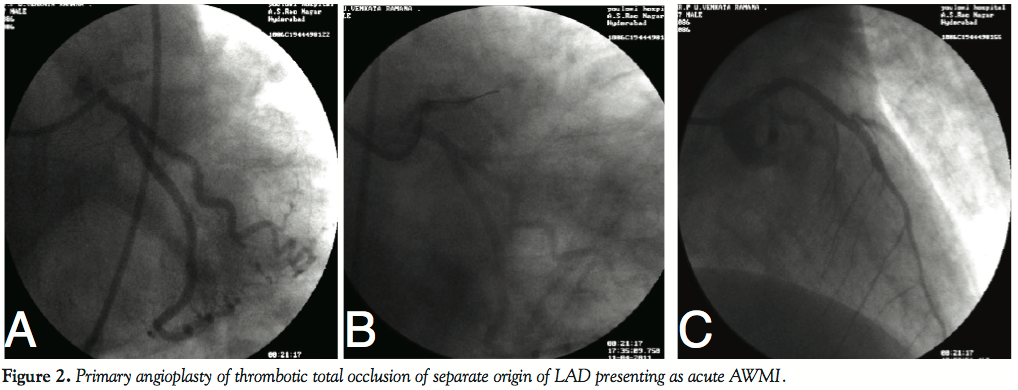 Case Report 2. A 50-year-old male presented with acute anterior wall MI of 8 H duration with persistent chest pain and ST segment elevations in ECG. He was taken up for primary percutaneous transluminal coronary angioplasty (PTCA) after front-loading with GPIIb/IIIa inhibitors and double antiplatelets. Coronary angiogram by Judkins Left 3.5 guiding catheter revealed absent left main and separate origin of LAD and left circumflex (LCx) arteries. LCx was co-dominant and had mild disease. LAD was originating slightly posteriorly and immediately after origin was 100% occluded with a lot of thrombus burden. Initial attempts to cannulate the anomalous LAD with Judkins Left 3.5 guiding catheter and EBU 3.5 mm and 4 mm catheters were not successful. Abnormal LAD was cannulated with considerable manipulation of Judkins Left 4.0 catheter, which was kept in the aorta with its ostium aligned in the direction of the LAD ostium and 0.014-inch HT BMW wire was initially advanced through short stump of LAD and later Judkins Left 4.0 could be engaged. The catheter also provided enough support to cross the thrombotic lesion and after clot extraction with the Export catheter (Medtronic) and multiple balloon predilatations in the LAD, the 3.0 mm x 28 mm Eurocor paclitaxel-eluting Stent (Genius Taxcor) was deployed at 16 atms. We achieved excellent angiographic result. The patient also had mid RCA 70%-80% stenosis, which was stented at a later date.
Case Report 2. A 50-year-old male presented with acute anterior wall MI of 8 H duration with persistent chest pain and ST segment elevations in ECG. He was taken up for primary percutaneous transluminal coronary angioplasty (PTCA) after front-loading with GPIIb/IIIa inhibitors and double antiplatelets. Coronary angiogram by Judkins Left 3.5 guiding catheter revealed absent left main and separate origin of LAD and left circumflex (LCx) arteries. LCx was co-dominant and had mild disease. LAD was originating slightly posteriorly and immediately after origin was 100% occluded with a lot of thrombus burden. Initial attempts to cannulate the anomalous LAD with Judkins Left 3.5 guiding catheter and EBU 3.5 mm and 4 mm catheters were not successful. Abnormal LAD was cannulated with considerable manipulation of Judkins Left 4.0 catheter, which was kept in the aorta with its ostium aligned in the direction of the LAD ostium and 0.014-inch HT BMW wire was initially advanced through short stump of LAD and later Judkins Left 4.0 could be engaged. The catheter also provided enough support to cross the thrombotic lesion and after clot extraction with the Export catheter (Medtronic) and multiple balloon predilatations in the LAD, the 3.0 mm x 28 mm Eurocor paclitaxel-eluting Stent (Genius Taxcor) was deployed at 16 atms. We achieved excellent angiographic result. The patient also had mid RCA 70%-80% stenosis, which was stented at a later date.
Topaz et al4 described various aspects of orifice configuration, anatomy of the artery, location of atherosclerotic lesions, and guiding catheter selection. Proper guiding catheter selection decreases procedure time in PTCA involving anomalous coronary arteries and thus increases success rates. We were able to cannulate the anomalous RCA and LAD in our case with relative ease and had good backup support using the modified Amplatzer I and standard Judkins Left 4.0 guiding catheters, respectively.
Discussion. The association of anomalous RCA with the onset of significant atherosclerosis at a younger age has been described previously.7 Yip et al10 found that the incidence of infarct-related anomalous RCA is higher in patients who underwent primary angioplasty. Thus, early recognition and precise cannulation are important for early mechanical reperfusion in this scenario.
The ostia of anomalous coronary arteries are difficult to reach with guiding catheters designed for normal coronary anatomy. Moreover, the ectopic ostium is usually juxta-commissural, and the proximal course of the anomalous artery is tangential to the aortic wall.12 These anatomical features prevent the institution of coaxiality of guiding catheters. The two main hindrances for successful angioplasty of anomalous arteries are delayed recognition of abnormal origin and technical difficulty in cannulating them with conventional catheters leading to wastage of fluoroscopic time and contrast; and poor guiding support encountered during interventions. Sometimes taking different projections like a right anterior oblique view can provide useful information.10
There are several case reports on percutaneous coronary intervention (PCI) performed for anomalous RCA originating from the left sinus of Valsalva.5,7-9 Most of these describe the experience with balloon angioplasty alone using 8 Fr guiding catheters of different configurations. The Amplatzer I guiding catheter was successfully used in 2 cases.8,9 In 2 other cases, a balloon-on-a-wire system was used to treat the target lesion because of poor guiding catheter support.8,9 Oral et al7 reported that stable support could not be accomplished with the use of an Amplatzer II guiding catheter, and that they were unable to advance the balloon catheter into the anomalous coronary artery. Cohen at al5 reported successful stenting in 2 cases of anomalous RCA with the use of a 6 Fr Judkins left 5.0 cm guiding catheter.
In order for PCI to be successful in anomalous coronary arteries, optimal guiding catheter seating and catheter backup support should be achieved, both of which may require modifications in the kind of guiding catheter used. We believe that the method described here for cannulation of an aberrant RCA arising from the left sinus of Valsalva will increase the likelihood of technical success. The use of a multipurpose Hockey Stick catheter may be considered when the usual techniques fail to visualize an anomalous RCA. Ikari et al quantitatively measured the backup force of guiding catheters for the RCA and found 3 factors to be significant: 1) catheter size; 2) the area of contact made by the catheter on the aorta; and 3) the angle [theta] of the catheter on the reverse side of the aorta.17
Anomalous RCAs can be classified based on:
 Abnormal position of ostium within right sinus: can be high takeoff (>1.5 cm from aortic valves), low takeoff (<1 cm from valves) and either anterior (common) or posterior displacement of ostium at normal level;
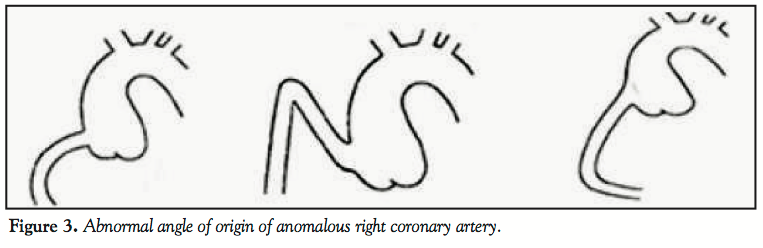
Abnormal position of ostium within right sinus: can be high takeoff (>1.5 cm from aortic valves), low takeoff (<1 cm from valves) and either anterior (common) or posterior displacement of ostium at normal level;- Abnormal angle of origin: horizontal angle, upward angle, and downward angle (Figure 3)
- Abnormal position from different sinus: left sinus (common), posterior sinus, aortic wall, and single coronary artery.20
Usually anomalies occur in combinations of the above listed variations.
Upward angle origin of RCA (<90° angle from aortic wall) is particularly challenging to engage and attain coaxially. Judkins or Amplatzer catheters can be tried. For downward pointing RCAs, multipurpose, Amplatzer, or venous bypass catheters can be used.
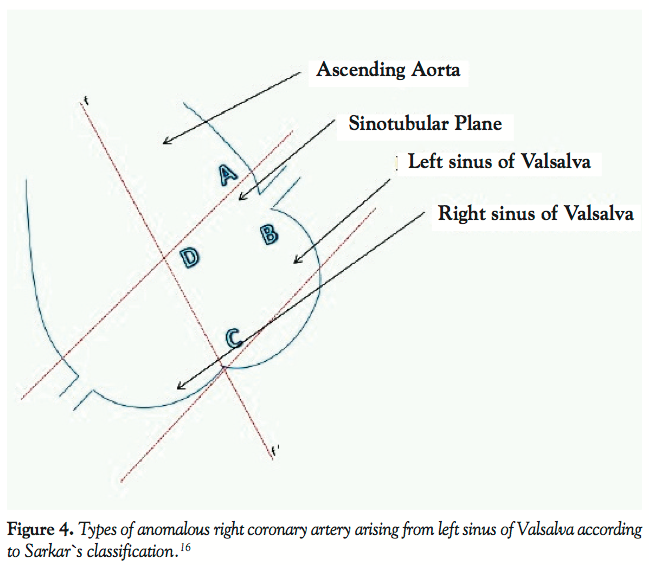 Anomalous origin of RCA from left sinus of Valsalva, which is common and most challenging to intervene, can be further classified into 4 parts by 2 imaginary lines drawn in the aortic root shoot in the left anterior oblique view. This was done by Sarkar et al based on 24 patients with anomalous RCAs from left sinus out 40,000 consecutive angiograms performed during their study (Figure 4).16
Anomalous origin of RCA from left sinus of Valsalva, which is common and most challenging to intervene, can be further classified into 4 parts by 2 imaginary lines drawn in the aortic root shoot in the left anterior oblique view. This was done by Sarkar et al based on 24 patients with anomalous RCAs from left sinus out 40,000 consecutive angiograms performed during their study (Figure 4).16
Type A - Origin from the aorta above the sinotubular plane: forward takeoff Judkins was the best.
Type B - Origin just below the ostium of the left coronary artery forward curve: Left Judkins was best.
Type C - Origin below the sinotubular plane between the midline and the left coronary artery: Voda Left (VL) was the best catheter.
Type D - Origin along the midline: Amplatzer catheters were best for intervention.
Our cases belonged to the type D anomalous RCA origin and for such arteries Amplatzer I, II, and III were the best catheters to cannulate. Though angiogram was successfully done by an Amplatzer II diagnostic catheter, for PTCA, a simple Amplatzer guiding catheter was not sufficient and it required on-table modification of an Amplatzer I catheter by making it broader, wider, and deeper so that the base of U shape of catheter sat on the aortic cusp and the area of contact on the aorta is maximum. The primary curve of the Amplatzer I guiding catheter was also modified based on coronary artery curve angle and this allowed easy cannulation of the anomalous RCA. Also this configuration provided adequate backup force during intervention of the total occlusion.
The anomalies of the left coronary system include absent left main with separate origin as in our case report and also have similar variations in origin, which include high or low takeoffs, abnormal angulation/proximal course, and anomalous sinuses of origin. Some have used the trial and error approach for these anomalies but there is no clear scientific method described for optimum catheter selection.4,21 What we propose in this paper is to develop patient-specific catheter selection depending upon angiogram measurements, later compared with the database on available catheter types and sizes in the cath lab, and arrive at a logical conclusion as to which is the best suited catheter for these difficult interventions.
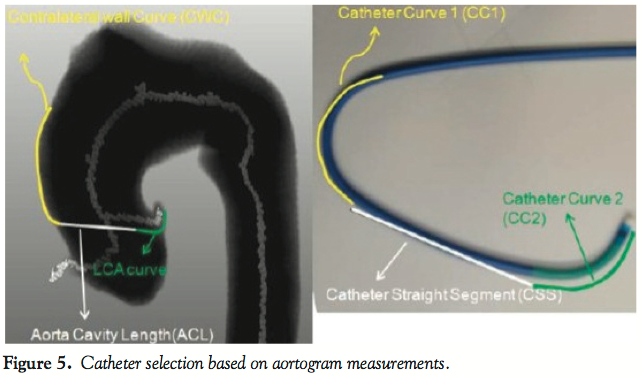 Rahman18 and others provided a solution for catheter selection based on a patient’s imaging data and guide catheters with appropriate curve length and curve angles suitable for difficult cases. This approach includes segmentation of the aorta and both arteries through MRI or CT angiography or conventional angiography images; computing coronary arteries curve angle, distance of the ostium from the aortic valves, and the aorta diameter near the ostium; and suggest a suitable catheter of appropriate dimensions that fits closest to the patient’s artery geometry (Figures 5 and 6).19
Rahman18 and others provided a solution for catheter selection based on a patient’s imaging data and guide catheters with appropriate curve length and curve angles suitable for difficult cases. This approach includes segmentation of the aorta and both arteries through MRI or CT angiography or conventional angiography images; computing coronary arteries curve angle, distance of the ostium from the aortic valves, and the aorta diameter near the ostium; and suggest a suitable catheter of appropriate dimensions that fits closest to the patient’s artery geometry (Figures 5 and 6).19
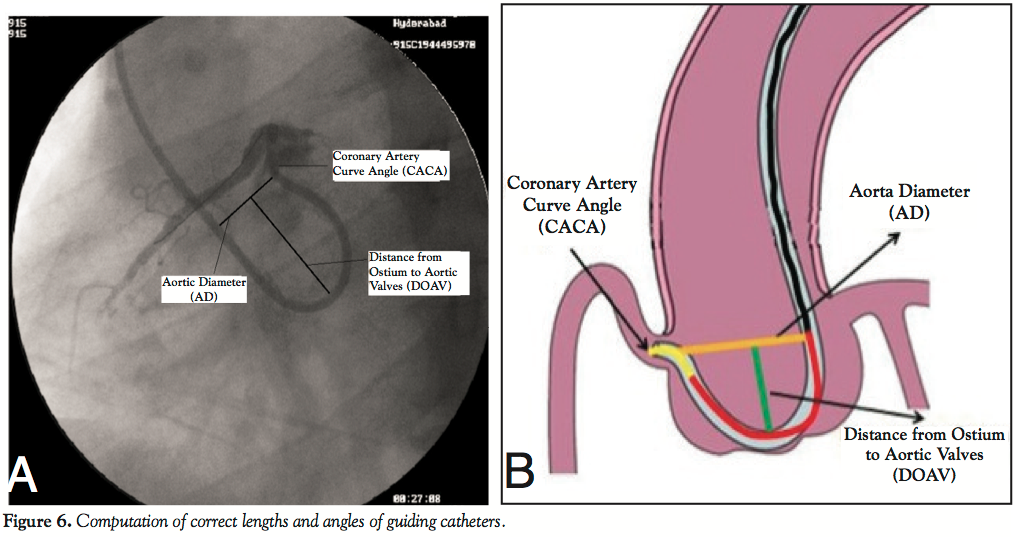 Calculation of various angles and lengths from angiograms and comparing with various catheter parameters for optimal catheter selection in anomalous artery origins is pertinent. This technique avoids testing of many catheters during catheterization. The interventionist already gets a recommendation about the optimal catheter for the patient prior to the start of the procedure and saves lot of procedure time. In the future, it is useful to utilize this method more instead of opting for more complicated techniques for crossing CTOs such as the double anchoring balloon technique by antegrade route, retrograde technique with balloon-on-a-wire-system, mother and child technique, and penetration catheters as described earlier in case reports.13,15
Calculation of various angles and lengths from angiograms and comparing with various catheter parameters for optimal catheter selection in anomalous artery origins is pertinent. This technique avoids testing of many catheters during catheterization. The interventionist already gets a recommendation about the optimal catheter for the patient prior to the start of the procedure and saves lot of procedure time. In the future, it is useful to utilize this method more instead of opting for more complicated techniques for crossing CTOs such as the double anchoring balloon technique by antegrade route, retrograde technique with balloon-on-a-wire-system, mother and child technique, and penetration catheters as described earlier in case reports.13,15
In this case we dealt with several technical challenges, such as the posterior location of the ostium in the left sinus, and the tortuous proximal portion and extremely angulated rightward and backward course of the anomalous artery, followed by total occlusion, which requires sufficient backup support during PCI.
Conclusion
For successful PCI of anomalous coronary arteries with total occlusions, optimal guiding catheter seating and catheter backup support should be achieved, both of which may require appropriate modifications of existing catheters. Computing approximate dimensions of guiding catheters before beginning a procedure by newer methods will reduce procedure time and increase the likelihood of technical success without resorting to more complicated intervention techniques.
References
- Click RL, Holmes DR Jr, Vlietstra RE, Kosinski AS, Kronmal RA. Anomalous coronary arteries: location, degree of atherosclerosis and effect on survival — a report from the Coronary Artery Surgery Study. J Am Coll Cardiol. 1989;13(3):531-537.
- Yamanaka O, Hobbs RE. Coronary artery anomalies in 126,595 patients undergoing coronary arteriography. Cathet Cardiovasc Diagn. 1990;21(1):28-40.
- Leberthson RR, Dinsmore RE, Bharati S, et al. Aberrant coronary artery origin from the aorta: Diagnosis and clinical significance. Circulation. 1974;50(4):774-779.
- Topaz O, DiSciascio G, Goudreau E, et al. Coronary angioplasty of anomalous coronary arteries: notes on technical aspects. Cathet Cardiovasc Diagn. 1990;21(2):106-111.
- Musial B, Schob A, de Marchena E, Kessler KM. Percutaneous transluminal coronary angioplasty of anomalous right coronary artery. Cathet Cardiovasc Diagn. 1991;22(1):39-41.
- Charney R, Spindola-Franco H, Grose R. Coronary angioplasty of anomalous right coronary arteries. Cathet Cardiovasc Diagn. 1993;29(3):233-235.
- Oral D, Dağalp Z, Pamir G, et al. Percutaneous transluminal coronary angioplasty of anomalous coronary arteries. Case reports. Angiology. 1996;47(1):77-82.
- Mooss AN, Heintz MH. Percutaneous transluminal angioplasty of anomalous right coronary artery. Cathet Cardiovasc Diagn. 1989;16(1):16-18.
- Chakraborty B, Chan CN, Tan A. Percutaneous transluminal coronary angioplasty of an anomalous right coronary artery arising from a separate ostium in the left sinus of Valsalva. A case report. Angiology. 1995;46(7):629-632.
- Yip H, Chen MC, Wu CJ, et al. Primary angioplasty in acute inferior myocardial infarction with anomalous-origin right coronary arteries as infarct-related arteries: focus on anatomic and clinical features, outcomes, selection of guiding catheters and management. J Invasive Cardiol. 2001;13(4):290-297.
- Lorin JD, Robin B, Lochow P, Lorenzo A, Sedlis SP. The right radial approach for stenting of lesions in the right coronary artery with anomalous take-off from the left sinus of valsalva. J Invasive Cardiol. 2000;12(9):478-480.
- Agarwala R, Kapoor A. The mystery of the lost and found right coronary artery. Catheter Cardiovasc Interv. 2010;76(7):969-972.
- Fang HY, Wu CC, Wu CJ. Successful transradial antegrade coronary intervention of a rare right coronary artery high anterior downward takeoff anomalous chronic total occlusion by double-anchoring technique and retrograde guidance. Int Heart J. 2009;50(4):531-538.
- Turgut O, Tandogan I, Dizman R. Use of the RCB guide in PCI of a chronic total occlusion in an anomalous right coronary artery with high anterior takeoff. J Invasive Cardiol. 2009;21(4):E70-E72.
- Utunomiya M, Katoh O, Nakamura S. Percutaneous coronary intervention for a right coronary artery stent occlusion using retrograde delivery of a sirolimus-eluting stent via a septal perforator. Catheter Cardiovasc Interv. 2009;73(4):475-480.
- Sarkar K, Sharma SK, Kini AS. Catheter selection for coronary angiography and intervention in anomalous right coronary arteries. J Interv Cardiol. 2009;22(3):234-239. Epub 2009 Apr 2.
- Ikari Y, Ochiai M, Hangaishi M, et al. Novel guide catheter for left coronary intervention via a right upper limb approach. Cathet Cardiovasc Diagn. 1998;44(2):244-247.
- Rahman S, Wesarg S, Voelker W. Patient specific optimal catheter selection for right coronary artery. Proceedings of SPIE Medical Imaging 2011, Florida.
- Rauf U. Optimal catheter selection for anomalous Right Coronary Arteries (RCA). Thesis Number: MEE10:115: Blekinge Institute of technology, Germany. January 2011.
- Jim MH, Ko RL, Chan CW, Cheung SC, Chow WH. Angioplasty on an infarct-related anomalous right coronary artery arising from posterior coronary sinus. Ann Acad Med Singapore. 2010;39(3):258-260.
- Lee JJ, Kim DH, Byun SS, et al. A case of acute myocardial infarction with the anomalous origin of the right coronary artery from the ascending aorta above the left sinus of Valsalva and left coronary artery from the posterior sinus of Valsalva. Yonsei Med J. 2009;50(1):164-168.
____________________________________________________
From the Interventional Cardiology Consultant in Global Hospitals Hyderabad, Head of Unit II Department of Cardiology ESI Hospitta Sanathnagar, Formerly HOD of Department of Cardiology Poulomi Hospitals, India.
Disclosure: The author has completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The author reports no conflicts of interest regarding the content herein.
Manuscript submitted April 5, 2012, provisional acceptance given May 22, 2012, final version accepted June 4, 2012.
Address for correspondence: Ponangi Udaya Prashant, MD, DM, Plot No:- 306, Near Life Spring Hospital, Jawaharnagar, Moulali, Hyderabad. Pin – 500040. Andhra Pradesh, India. Email: udayaprashant_p@yahoo.co.in











