

Successful Coronary Intervention of Circumflex Artery Originating From an Anomalous Left Main Coronary Artery Using a Novel Support Catheter: A Case Report and Review of Literature
Abstract: Anomalous coronary arteries pose a great challenge during percutaneous intervention due to various technical factors. Inadequate guide support leads to significant obstacles for delivery of interventional devices to stenotic areas. Several methods have been proposed to overcome these obstacles. We present a novel technique where we used the Guideliner support catheter (Vascular Solutions, Inc.) to successfully intervene on a left circumflex coronary artery arising from a left main coronary artery anomalously arising from the right sinus of Valsalva.
J INVASIVE CARDIOL 2011;23(12):536-539
Key words: percutaneous coronary intervention, anomalous coronary artery, Guideliner
______________________________________________
 Congenital anomalies of the coronary arteries pose a challenge for coronary intervention due to multiple factors including the abnormal origin and the course of the artery. Challenges arise frequently from the lack of adequate guide support for delivery of devices to the target lesion. We present the case of a successful intervention performed on a critical stenosis in a left circumflex (LCX) artery that arose from an anomalous left main (LM) coronary artery originating from the right sinus of Valsalva. A novel technique was used that involved the use of the Guideliner support catheter (Vascular Solutions, Inc.).
Congenital anomalies of the coronary arteries pose a challenge for coronary intervention due to multiple factors including the abnormal origin and the course of the artery. Challenges arise frequently from the lack of adequate guide support for delivery of devices to the target lesion. We present the case of a successful intervention performed on a critical stenosis in a left circumflex (LCX) artery that arose from an anomalous left main (LM) coronary artery originating from the right sinus of Valsalva. A novel technique was used that involved the use of the Guideliner support catheter (Vascular Solutions, Inc.).
Case Report
 A 65-year-old male with prior history of coronary artery bypass grafting (CABG) presented with non-ST segment elevation myocardial infarction. Five years prior to presentation, he had undergone a 2-vessel CABG, with vein grafts to the right posterior descending artery (RPDA) and left anterior descending artery (LAD). The LM coronary artery was anomalous, originating from the right sinus of Valsalva. At the time of CABG, he only had severe disease in the right coronary artery (RCA), while the LAD was grafted only because it was thought to be
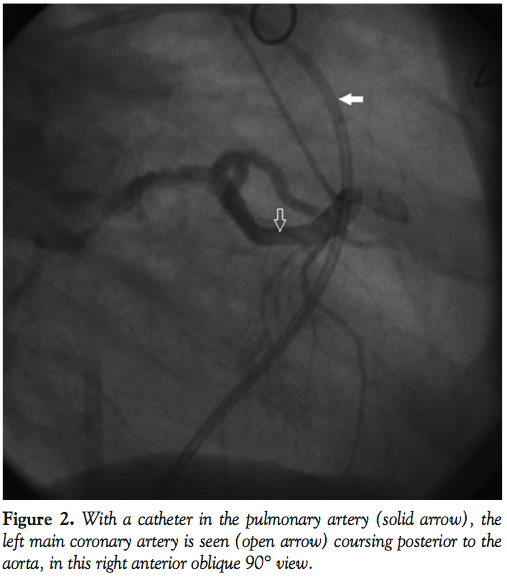
A 65-year-old male with prior history of coronary artery bypass grafting (CABG) presented with non-ST segment elevation myocardial infarction. Five years prior to presentation, he had undergone a 2-vessel CABG, with vein grafts to the right posterior descending artery (RPDA) and left anterior descending artery (LAD). The LM coronary artery was anomalous, originating from the right sinus of Valsalva. At the time of CABG, he only had severe disease in the right coronary artery (RCA), while the LAD was grafted only because it was thought to be 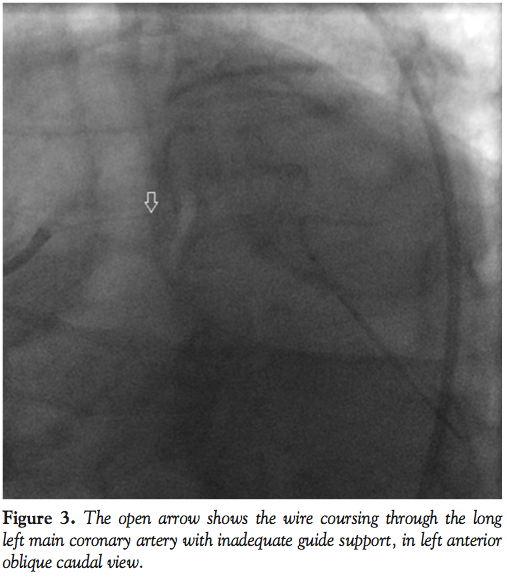 coming off of the LM at a very acute angle, which was felt to be a risk for future stenosis of the LAD. The LM was deemed not to be inter-arterial (running between the aorta and pulmonary artery). During the current admission, cardiac catheterization revealed that both vein grafts were totally occluded. RCA was totally occluded, with filling of the RPDA via collaterals from the left. Additionally, there was a critical 99% stenosis in the proximal LCX (Figure 1). The patient was referred for re-operation CABG. However, the surgeons only considered him a candidate for re-operation if the LM was coursing inter-arterially. Upon repeat cardiac catheterization and by placing a catheter in the pulmonary artery, it was confirmed that the LM actually coursed posterior to the aorta, and not inter-arterially (Figure 2). The LM had an intra-septal course and it gave off large septal branches before bifurcating; however, there was no systolic compression of the LM.
coming off of the LM at a very acute angle, which was felt to be a risk for future stenosis of the LAD. The LM was deemed not to be inter-arterial (running between the aorta and pulmonary artery). During the current admission, cardiac catheterization revealed that both vein grafts were totally occluded. RCA was totally occluded, with filling of the RPDA via collaterals from the left. Additionally, there was a critical 99% stenosis in the proximal LCX (Figure 1). The patient was referred for re-operation CABG. However, the surgeons only considered him a candidate for re-operation if the LM was coursing inter-arterially. Upon repeat cardiac catheterization and by placing a catheter in the pulmonary artery, it was confirmed that the LM actually coursed posterior to the aorta, and not inter-arterially (Figure 2). The LM had an intra-septal course and it gave off large septal branches before bifurcating; however, there was no systolic compression of the LM.
 Therefore, we proceeded with percutaneous coronary intervention (PCI) of the subtotal occlusion of the LCX. A 6 Fr JR 5 guide catheter was used to engage the ostium of the LM. A Fielder wire (Abbott Vascular) was used to cross the critical stenosis in the LCX with the support of a 1.5 x 8 mm over-the-wire apex balloon (Boston Scientific Corporation). The Fielder wire was exchanged for a Grand Slam wire (Abbott Vascular). Then, the 1.5 mm balloon was used to perform angioplasty in the LCX. Attempts to advance a larger balloon or a stent were
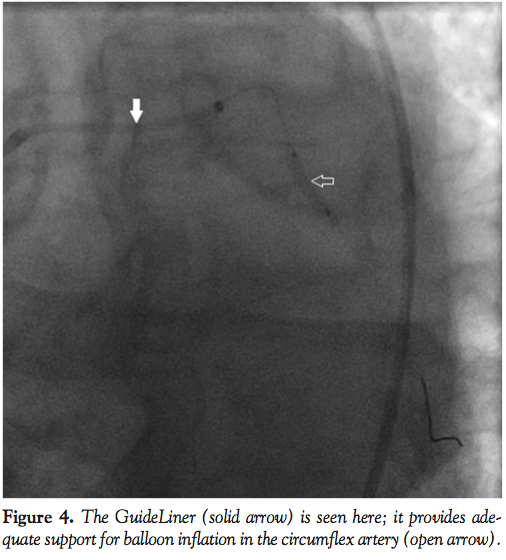
Therefore, we proceeded with percutaneous coronary intervention (PCI) of the subtotal occlusion of the LCX. A 6 Fr JR 5 guide catheter was used to engage the ostium of the LM. A Fielder wire (Abbott Vascular) was used to cross the critical stenosis in the LCX with the support of a 1.5 x 8 mm over-the-wire apex balloon (Boston Scientific Corporation). The Fielder wire was exchanged for a Grand Slam wire (Abbott Vascular). Then, the 1.5 mm balloon was used to perform angioplasty in the LCX. Attempts to advance a larger balloon or a stent were 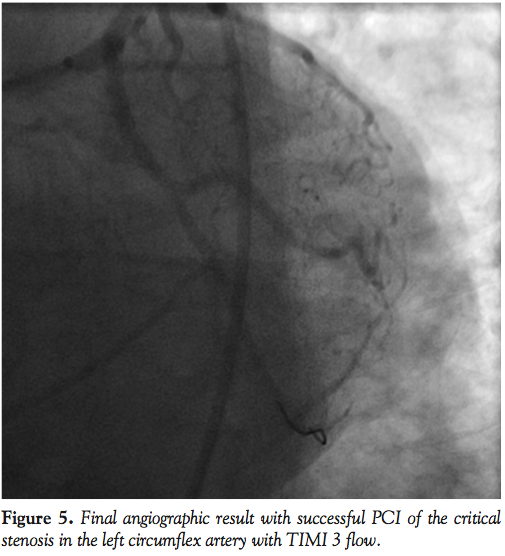 unsuccessful, as the guide catheter continued to disengage from the LM, resulting in pulling back of the guidewire (Figure 3). At this point, we decided to use a 6 Fr GuideLiner catheter (Vascular Solutions, Inc.) for additional support. The GuideLiner catheter was placed in the distal LM immediately proximal to its bifurcation (Figure 4). Subsequently, we were able to deliver a 2.5 x 12 mm Quantum balloon (Boston Scientific Corporation) to the stenosis without difficulty, which was used to perform angioplasty. Finally, a 2.75 x 15 mm Promus drug-eluting stent (Boston Scientific Corporation) was deployed at 13 atm. Final angiography revealed TIMI 3 flow without residual stenosis or dissection (Figure 5). Notably, once the GuideLiner catheter was positioned in the distal LM, not only was there excellent guiding catheter support and much easier advancement of interventional devices into the stenosis, but the quality of angiography improved due to improved ability to inject contrast directly into the distal LM. The patient continues to do well almost a year after the procedure.
unsuccessful, as the guide catheter continued to disengage from the LM, resulting in pulling back of the guidewire (Figure 3). At this point, we decided to use a 6 Fr GuideLiner catheter (Vascular Solutions, Inc.) for additional support. The GuideLiner catheter was placed in the distal LM immediately proximal to its bifurcation (Figure 4). Subsequently, we were able to deliver a 2.5 x 12 mm Quantum balloon (Boston Scientific Corporation) to the stenosis without difficulty, which was used to perform angioplasty. Finally, a 2.75 x 15 mm Promus drug-eluting stent (Boston Scientific Corporation) was deployed at 13 atm. Final angiography revealed TIMI 3 flow without residual stenosis or dissection (Figure 5). Notably, once the GuideLiner catheter was positioned in the distal LM, not only was there excellent guiding catheter support and much easier advancement of interventional devices into the stenosis, but the quality of angiography improved due to improved ability to inject contrast directly into the distal LM. The patient continues to do well almost a year after the procedure.
Discussion
Anomalous coronary arteries. Normal coronary artery anatomy is characterized by the origins of the RCA and left coronary artery (LCA) from ostia from the respective sinuses of Valsalva in the aortic root. Congenital anomalies of the coronary arteries occur either in isolation as primary anomalies or as secondary anomalies in association with other congenital disease.1 Primary congenital anomalies of the coronary arteries are rather rare. Reports of their incidence vary from 0.3-1.6% in various case series.2 They are of the following types: a) ectopic origin from the aortic sinus; b) stenosis of coronary arteries; c) absence of a coronary artery; d) anomalous origin of the LCA or RCA from the pulmonary artery; and e) congenital coronary artery fistula.1 Our patient had a primary congenital coronary anomaly as no other associated anomaly was identified.
The most common anomaly is an LCX arising from the RCA, with an incidence as high as 50% of all coronary anomalies in one case series.3 An anomalous LM is among the rarest, with an incidence of 2.5-12% of all congenital coronary arterial anomalies, and is commonly associated with other congenital defects.4,5 However, in our patient, origin of the LM from the right sinus occurred in isolation.
When the LM originates from the right sinus of Valsalva, it may be classified into one of four types: a) the LM passes between the aorta and pulmonary trunk, posteriorly and adjacent to the pulmonary trunk; b) the LM passes anteriorly over the right ventricular outflow tract; c) the LM courses along the crista supraventricularis intramyocardially or subendocardially, surfacing in the proximal interventricular sulcus; and d) the LM may rise to the right of the RCA and pass posteriorly to the aortic root or anterior to the pulmonary trunk.1 In our patient, the LM coursed posterior to the aorta (Figure 2).
Anomalous LM arising from the right sinus of Valsalva having an intraseptal course is an extremely rare and potentially fatal congenital anomaly, with a reported incidence of 0.017% in one large series.6-8 The septal course of the LM has also been referred to as “intra-myocardial” or “tunneled” anomalous origin.9,10 The angulation of the artery after its origin from the aortic sinus determines the risk of occlusion. An acute angulation results in a slit-like ostium. With increased cardiac output and the accompanying dilation of the aortic root, this slit-like ostium narrows even further, resulting in ischemia. Acute myocardial infarction and even sudden death have been reported both in cases where the anomalous artery coursed in between the great vessels and in those where it coursed anterior to the pulmonary trunk or posterior to the aorta.11,12
Regardless of the course of the coronary arteries, recognition of coronary anomalies is important prior to cardiac surgery as the accidental incision or exclusion of an anomalous vessel from perfusion during bypass can cause grave problems.13 Accurate identification of the origin and course of anomalous coronary arteries can prove decisive in the successful completion of interventional procedures, helping in the selection of appropriate guide catheters, guidewires and balloons.4
Technical difficulties in procedures on anomalous coronary arteries. PCI of anomalous coronary arteries poses several technical challenges. When a single coronary artery is given off from the aortic sinus which then bifurcates into RCA and LCA from a common ostium, the coronary arteries have an unusual direction and a tortuous angle making cannulation difficult. A potential complication of PCI in such cases is dissection that occurs with advancing the equipment. The retrograde extension of such a dissection may involve the origins of the LCA and RCA, with potentially catastrophic consequences.14
PCI in anomalous coronary arteries: proposed methods. In view of the increased technical difficulty of PCI in anomalous arteries, selection of the appropriate equipment assumes greater importance, ranging from successfully engaging the ostium of the anomalous coronary artery with adequate support to advance interventional devices and ultimately, concluding the procedure with minimal exposure to contrast agents and radiation. Various angiographic features such as aortic root dimensions, ostial configuration, takeoff angle and initial trajectory of the anomalous vessel, as well as the type of procedure planned, are factors that influence the selection of guide catheters.15 Another major hurdle experienced during PCI of extensively calcified or tortuous arteries is the lack of adequate back-up support from the guiding catheter, when advancing interventional devices. Use of buddy wires has been reported.16 Our case provides a novel technique that is an alternative to those previously described.
The GuideLiner system is a flexible coaxial catheter that is intended to be used in conjunction with any standard guide catheter and works as a “mother and child” system. It provides additional back-up support and coaxial alignment to access discrete regions of coronary vasculature and to facilitate delivery of devices as in our case. It has the convenience of rapid exchange with the ability to use standard length guidewires, balloons, or stents. However, it is important to avoid the use of the GuideLiner system in vessels that are less than 2.5 mm in diameter. A few recent cases have reported the use of GuideLiner support catheter for successful intervention of very tortuous or rigid (owing to prior stenting or extensive calcification) coronary arteries, mainly for distal delivery of balloons or stents.17 There has been a reported case of PCI of an anomalous LM in the setting of acute myocardial infarction.18 To our knowledge, this is the first report where a GuideLiner catheter has been successfully used for PCI of a very rare variety of anomalous LM coronary artery.
Our technique has certain advantages over the ones previously used. For instance, in comparison to the buddy wire technique, use of the GuideLiner system results in avoidance of rewiring of the target artery, which requires having to cross the tight stenosis with another wire, which can be difficult to achieve and also worsens ischemia or even worse, causes a dissection. Furthermore, lack of support from the guide catheter would also be an obstacle to advancement of a buddy wire as well, like in our case, where trying to advance a buddy wire with poor support from the JR5 catheter would have been difficult to achieve. We even experienced difficulty in trying to get the first wire across the critical stenosis in the circumflex artery. Additionally, due to the fact that with a GuideLiner, injection of contrast is closer to the site of intervention, contrast exposure would be reduced. The GuideLiner system can be advanced over the wire as simple as a monorail balloon, and does not involve manipulation of two guide catheters, as would be required in the actual “mother and child” technique.
Conclusion
Anomalous LM coronary arteries are extremely rare and percutaneous revascularization can be a great challenge because of the lack of support from the most commonly used guide catheters. Our use of the GuideLiner catheter for revascularization of the LCX arising from an anomalous LM coronary artery is a novel technique that can be utilized in similar cases.
References
- Hauser M. Congenital anomalies of the coronary arteries. Heart. 2005;91(9):1240-1245.
- Alexander RW, Griffith GC. Anomalies of the coronary arteries and their clinical significance. Circulation. 1956;14(5):800-805.
- Kimbiris D, Iskandrian AS, Segal BL, Bemis CE. Anomalous aortic origin of coronary arteries. Circulation. 1978;58(4):606-615.
- Garg N, Tewari S, Kapoor A, Gupta DK, Sinha N. Primary congenital anomalies of the coronary arteries: a coronary arteriographic study. Int J Cardiol. 2000;74(1):39-46.
- Topaz O, DeMarchena EJ, Perin E, Sommer LS, Mallon SM, Chahine RA. Anomalous coronary arteries: angiographic findings in 80 patients. Int J Cardiol. 1992;34(2):129-138.
- Yamanaka O, Hobbs RE. Coronary artery anomalies in 126,595 patients undergoing coronary arteriography. Cathet Cardiovasc Diagn. 1990;21(1):28-40.
- Cheitlin MD, De Castro CM, McAllister HA. Sudden death as a complication of anomalous left coronary origin from the anterior sinus of Valsalva, a not-so-minor congenital anomaly. Circulation. 1974;50(4):780-787.
- Mustafa I, Gula G, Radley-Smith R, Durrer S, Yacoub M. Anomalous origin of the left coronary artery from the anterior aortic sinus: a potential cause of sudden death. Anatomic characterization and surgical treatment. J Thorac Cardiovasc Surg. 1981;82(2):297-300.
- Vazquez-Jimenez JF, Haager PK, Genius M, et al. Anomalous origin of the left main coronary artery from the right aortic sinus with intramyocardial tunneling through the septum with free portion in the right ventricular cavity. J Thorac Cardiovasc Surg. 1999;118(5):963-965.
- Schiele TM, Weber C, Rieber J, et al. Images in cardiovascular medicine. Septal course of the left main coronary artery originating from the right sinus of Valsalva. Circulation. 2002;105(12):1511-1512.
- Murphy DA, Roy DL, Sohal M, Chandler BM. Anomalous origin of left main cononary artery from anterior sinus of Valsalva with myocardial infarction. J Thorac Cardiovasc Surg. 1978;75(2):282-285.
- Roberts WC, Kragel AH. Anomalous origin of either the right or left main coronary artery from the aorta without coursing of the anomalistically arising artery between aorta and pulmonary trunk. Am J Cardiol. 1988;62(17):1263-1267.
- Longenecker CG, Reemtsma K, Creech O Jr. Surgical implications of single coronary artery. A review and two case reports. Am Heart J. 1961;61:382-386.
- Kang WC, Ahn TH, Shin EK. Successful percutaneous coronary intervention for severe stenosis of an anomalous left coronary artery originating from the proximal right coronary artery. J Invasive Cardiol. 2006;18(5):E154-E156.
- Sarkar K, Sharma SK, Kini AS. Catheter selection for coronary angiography and intervention in anomalous right coronary arteries. J Interv Cardiol. 2009;22(3):234-239.
- Jafary FH. When one won’t do it, use two-double “buddy” wiring to facilitate stent advancement across a highly calcified artery. Catheter Cardiovasc Interv. 2006;67(5):721-723.
- Mamas MA, Fath-Ordoubadi F, Fraser DG. Distal stent delivery with Guideliner catheter: first in man experience. Catheter Cardiovasc Interv. 2010;76(1):102-111.
- Duran M, Ornek E, Murat SN, et al. Coronary stenting for acute myocardial infarction in a patient with an anomalous origin of the left main coronary artery. J Cardiovasc Med (Hagerstown). 2011;12(6):436-438.
______________________________________________
From the 1Department of Internal Medicine, and 2Cardiovascular Section, Department of Internal Medicine, University of Oklahoma Health Sciences Center, Oklahoma City, Oklahoma.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript submitted April 20, 2011, provisional acceptance given June 27, 2011, final version accepted August 17, 2011.
Address for correspondence: Faisal Latif, MD, FACC, FSCAI, Assistant Professor of Medicine, Cardiovascular Section, University of Oklahoma Health Sciences Center, 920 Stanton L. Young Blvd., WP#3010, Oklahoma City, OK 73104. Email: faisal-latif@ouhsc.edu









