Successful Percutaneous Closure of Periprosthetic Mitral Pseudoaneurysm Using a Duct Occluder Device
Ainhoa Pérez Guerrero, MD1; Gabriel Galache Osuna, MD1; Georgina Fuertes Ferre, MD1; Eva Moreno Esteban, MD2; Jose Antonio Diarte De Miguel, MD1
Key words: infective endocarditis, percutaneous closure, pseudoaneurysm
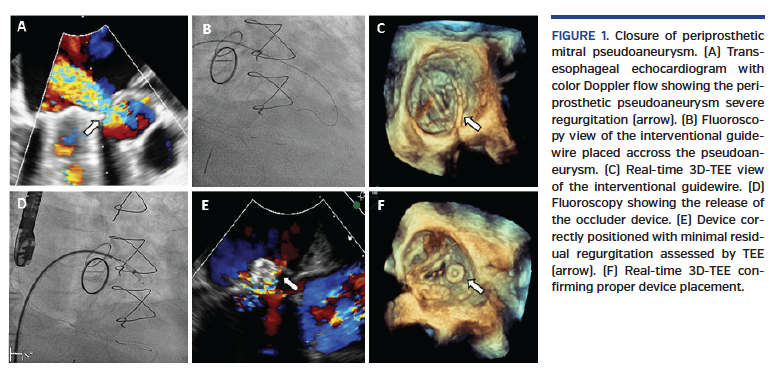
We describe the case of a 63-year-old man with infective endocarditis (IE) due to Streptococcus bovis on a native aortic valve replaced with a bioprosthesis. Despite culture-directed antibiotics, new relapse of IE occurred on the aortic bioprosthesis and the native mitral valve 2 months later. The patient underwent another mitral-aortic valve replacement with mechanical prosthesis. He presented a torpid clinical course, resulting in acute heart failure. Transesophageal echocardiography (TEE) showed a neocavity on the lateral margin of the anterior mitral annulus that connected to the left ventricle, producing a severe periprosthetic regurgitation (Figure 1A). Surgical reintervention was rejected and it was decided to attempt a percutaneous closure after 2 months of antibiotic therapy, with a negative blood culture result. The procedure was performed under general anesthesia. A 10 x 12 mm Amplatzer Duct Occluder device (Abbott Vascular) was chosen. Real-time three-dimensional (3D) TEE was used to guide the percutaneous closure. We followed an anterograde approach. After transseptal puncture, the guidewire was placed throughout the pseudoaneurysm (Figures 1B, 1C). The device was positioned to occlude the neocavity, and periprosthetic regurgitation was significantly reduced. After confirmation, there was no interference with the mitral prosthetic valve disc and the device was released (Figures 1D, 1E, 1F). The final real-time 3D-TEE showed minimal residual regurgitation. Antimicrobial therapy was continued for 7 days after the procedure. The patient remained clinically stable during a total follow-up of 3 years.
From the 1Interventional Cardiology Unit, Miguel Servet University Hospital, Zaragoza, Spain; and 2Image Cardiology Unit, Miguel Servet University Hospital, Zaragoza, Spain.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
The authors report that patient consent was provided for publication of the images used herein.
Manuscript accepted February 7, 2020.
Address for correspondence: Ainhoa Pérez Guerrero, MD, Interventional Cardiology Unit, Miguel Servet University Hospital, Paseo Isabel la Católica 1-2, 50001 Zaragoza, Spain. Email: ainhoaperezguerrero@gmail.com