

Successful Percutaneous Coronary Intervention of an Anomalous Right Coronary Artery with High Anterior Takeoff Using a DIO Thrombus Aspiration Catheter
ABSTRACT: Selecting an appropriate guiding catheter is the most important determinant of procedural percutaneous coronary intervention success, especially with an anomalous right coronary artery with high anterior takeoff, which is rather complicated. We present a case of successful stent implantation in an anomalous right coronary artery with high anterior takeoff using DIO thrombus aspiration catheter. This method is useful when selection of the guiding catheter is rather complicated such as in the case of congenital coronary anomalies.
J INVASIVE CARDIOL 2012;24(9):E185-e187
Key words: coronary anomaly, DIO thrombus aspiration catheter
_______________________________________________________
Coronary anomalies are found in 0.2%-1.2% of the population and represent a marked deviation of the normal anatomical pattern.1 Anomalous right coronary arteries (RCA) account for 6%-27% of all cases.2,3 There are currently only a few reports in the literature regarding percutaneous coronary intervention (PCI) in patients with anomalous coronary arteries.
The selection of a guiding catheter to access the anomalous origin and provide good support during PCI is very important. We sometimes must employ the mother-child (or 5 in 6) technique when strong back-up support is necessary for balloon delivery or stent implantation. Recently, the DIO thrombus aspiration catheter (DIO), which is similar to the 5 Fr straight catheter, became available. We report a successful case of PCI of an anomalous RCA with high anterior takeoff using the DIO thrombus aspiration catheter.
 Case Report. A 70-year-old man was admitted to the hospital because of chest pain. His risk factors for coronary artery disease included hypercholesterolemia and type 2 diabetes mellitus. The electrocardiogram taken on admission showed normal sinus rhythm with negative T wave in V1~V5 leads. He was diagnosed with acute coronary syndrome and underwent left coronary artery angiography via the right radial approach using a 4 Fr Judkin’s left 3.5 catheter. The angiography revealed 99% stenosis with a thrombus at the mid portion of the left anterior descending artery (LAD).
Case Report. A 70-year-old man was admitted to the hospital because of chest pain. His risk factors for coronary artery disease included hypercholesterolemia and type 2 diabetes mellitus. The electrocardiogram taken on admission showed normal sinus rhythm with negative T wave in V1~V5 leads. He was diagnosed with acute coronary syndrome and underwent left coronary artery angiography via the right radial approach using a 4 Fr Judkin’s left 3.5 catheter. The angiography revealed 99% stenosis with a thrombus at the mid portion of the left anterior descending artery (LAD).
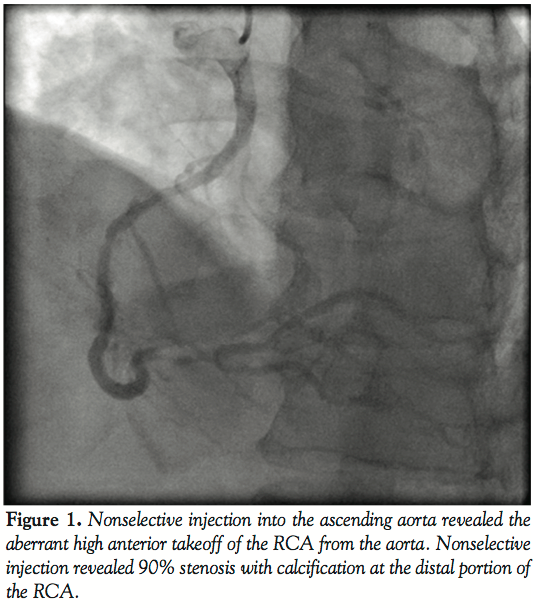
Selective cannulation of the RCA could not be achieved with Judkin’s right 4.0 catheter. Nonselective injection into the ascending aorta revealed the aberrant high anterior takeoff of the RCA from the aorta. Nonselective injection revealed 90% stenosis with calcification at the distal portion of the RCA. Following angiography, we performed PCI of the mid LAD.
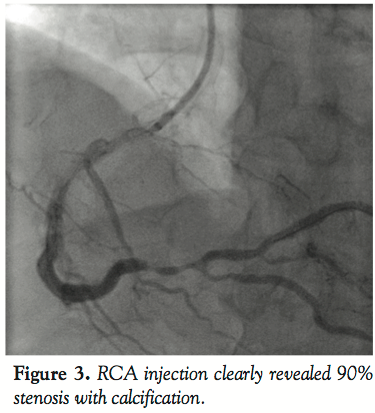
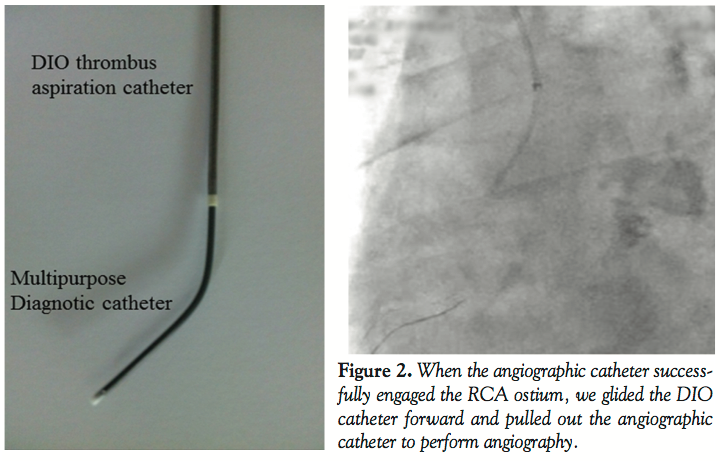 The post-procedural recovery of the patient was uneventful and thus he was discharged from the hospital with double anti-platelet therapy (100 mg of aspirin and 75 mg of clopidogrel sulfate) on the following day. One month later, the patient was re-admitted for PCI because of persistent chest pain on effort despite medical treatment. He was diagnosed 90% stenosis with severe calcification at the distal portion of the RCA by computed tomography. On the other hand, there was no stent thrombosis at the implanted stent lesion of LAD. We performed PCI of the RCA under local anesthesia and a 6 Fr sheath introducer was inserted into the right brachial artery. We inserted a 4 Fr multipurpose angiographic catheter into a DIO thrombus aspiration catheter to deliver it to the ascending aorta. The DIO was functionally stabilized to find the RCA ostium by manipulating the angiographic catheter. When the angiographic catheter successfully engaged the RCA ostium, we glided the DIO catheter forward and pulled out the angiographic catheter to perform angiography. RCA injection clearly revealed 90% stenosis with calcification. The lesion was crossed with a Neo’s Fielder guidewire (Asahi Intech Corporation), and pre-dilated with a 2.0 mm × 15 mm Lacrosse balloon catheter (Goodman Co. Ltd., Aichi) at 10 atm. We tried to deliver an Eagle eye IVUS catheter (Volcano Corporation), but it did not cross the lesion because of insufficient back-up force.
The post-procedural recovery of the patient was uneventful and thus he was discharged from the hospital with double anti-platelet therapy (100 mg of aspirin and 75 mg of clopidogrel sulfate) on the following day. One month later, the patient was re-admitted for PCI because of persistent chest pain on effort despite medical treatment. He was diagnosed 90% stenosis with severe calcification at the distal portion of the RCA by computed tomography. On the other hand, there was no stent thrombosis at the implanted stent lesion of LAD. We performed PCI of the RCA under local anesthesia and a 6 Fr sheath introducer was inserted into the right brachial artery. We inserted a 4 Fr multipurpose angiographic catheter into a DIO thrombus aspiration catheter to deliver it to the ascending aorta. The DIO was functionally stabilized to find the RCA ostium by manipulating the angiographic catheter. When the angiographic catheter successfully engaged the RCA ostium, we glided the DIO catheter forward and pulled out the angiographic catheter to perform angiography. RCA injection clearly revealed 90% stenosis with calcification. The lesion was crossed with a Neo’s Fielder guidewire (Asahi Intech Corporation), and pre-dilated with a 2.0 mm × 15 mm Lacrosse balloon catheter (Goodman Co. Ltd., Aichi) at 10 atm. We tried to deliver an Eagle eye IVUS catheter (Volcano Corporation), but it did not cross the lesion because of insufficient back-up force.
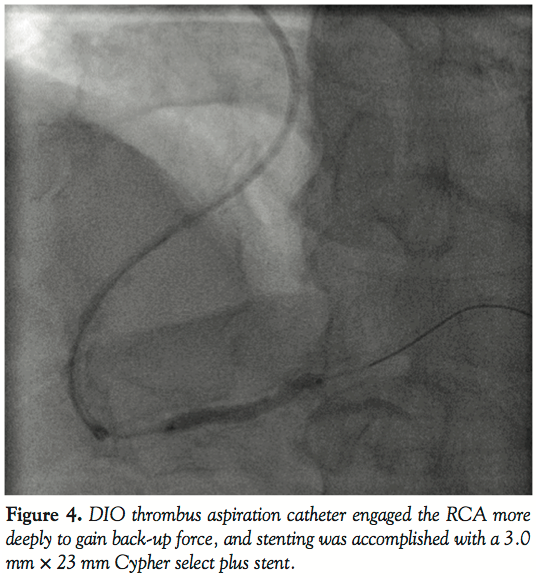
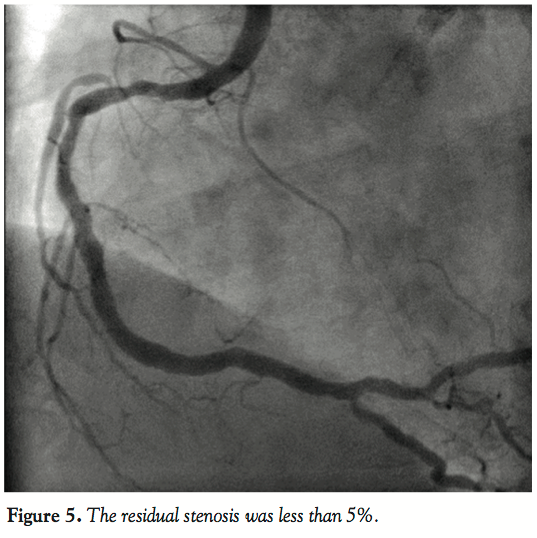
 In an effort to insert the intravascular ultrasound catheter up to the mid portion of the RCA, we engaged the RCA more deeply using the DIO thrombus aspiration catheter to gain back-up force. Stenting was accomplished with a 3.0 mm × 23 mm Cypher select plus stent (Cordis, Johnson and Johnson Interventional System) delivered at 14 atm. The residual stenosis was less than 5%. This excellent result was accomplished by deep engagement using a DIO thrombus aspiration catheter.
In an effort to insert the intravascular ultrasound catheter up to the mid portion of the RCA, we engaged the RCA more deeply using the DIO thrombus aspiration catheter to gain back-up force. Stenting was accomplished with a 3.0 mm × 23 mm Cypher select plus stent (Cordis, Johnson and Johnson Interventional System) delivered at 14 atm. The residual stenosis was less than 5%. This excellent result was accomplished by deep engagement using a DIO thrombus aspiration catheter.
 Discussion. Challenging an anomalous RCA, especially with high anterior takeoff, is rather complicated. Selective cannulation of aberrant arteries can be difficult and time-consuming. Knowledge of the variations in coronary artery origin can help in selecting the appropriate catheters for diagnostic and therapeutic interventions.4 Selecting an appropriate guiding catheter is the most important determinant of procedural success. In several case reports describing successful PCI of anomalous RCA, Amplatz curve guiding catheters were used,5-7 but Amplatz catheters are usually too short or too long. In fact, there is a lot of variation in Amplatz catheters, which makes finding a suitable size difficult. If it is too short, the tip may not reach the ostium; if it is too long, the catheter may prolapse into the left ventricle. A few authors used Judkin’s left curve guiding catheters,8-9 but these reports describe experiences with balloon angioplasty alone.
Discussion. Challenging an anomalous RCA, especially with high anterior takeoff, is rather complicated. Selective cannulation of aberrant arteries can be difficult and time-consuming. Knowledge of the variations in coronary artery origin can help in selecting the appropriate catheters for diagnostic and therapeutic interventions.4 Selecting an appropriate guiding catheter is the most important determinant of procedural success. In several case reports describing successful PCI of anomalous RCA, Amplatz curve guiding catheters were used,5-7 but Amplatz catheters are usually too short or too long. In fact, there is a lot of variation in Amplatz catheters, which makes finding a suitable size difficult. If it is too short, the tip may not reach the ostium; if it is too long, the catheter may prolapse into the left ventricle. A few authors used Judkin’s left curve guiding catheters,8-9 but these reports describe experiences with balloon angioplasty alone.
 Benjamin et al performed percutaneous coronary artery stenting of anomalous RCA with high takeoff using Judkin’s left guiding catheter.10 In their patient the origin of RCA was anterior and superior. Recently, the DIO thrombus aspiration catheter that includes a 4 Fr angiographic catheter became available. Therefore, it is possible to engage the coronary artery by sliding the angiographic catheter. Tortuosity of the subclavian artery is a severe problem when using the transradial approach. In the case of a very tortuous subclavian artery, it is not uncommon to kink the angiographic catheter, and DIO can provide strong support of the catheter without kinking. By inserting DIO into the subclavian artery, it is possible to operate the angiographic catheter more delicately. Sometimes a series of treatments from coronary angiography to PCI become complex, which prolongs the duration of the procedure because of the time required for selecting an adequate guiding catheter. By inserting a 4 Fr angiographic catheter into DIO, it is possible to perform the sequence of treatments safer using the 4 Fr angiographic catheter only. Therefore, DIO is useful when selection of the guiding catheter is rather complicated such as in the case of congenital coronary anomalies.
Benjamin et al performed percutaneous coronary artery stenting of anomalous RCA with high takeoff using Judkin’s left guiding catheter.10 In their patient the origin of RCA was anterior and superior. Recently, the DIO thrombus aspiration catheter that includes a 4 Fr angiographic catheter became available. Therefore, it is possible to engage the coronary artery by sliding the angiographic catheter. Tortuosity of the subclavian artery is a severe problem when using the transradial approach. In the case of a very tortuous subclavian artery, it is not uncommon to kink the angiographic catheter, and DIO can provide strong support of the catheter without kinking. By inserting DIO into the subclavian artery, it is possible to operate the angiographic catheter more delicately. Sometimes a series of treatments from coronary angiography to PCI become complex, which prolongs the duration of the procedure because of the time required for selecting an adequate guiding catheter. By inserting a 4 Fr angiographic catheter into DIO, it is possible to perform the sequence of treatments safer using the 4 Fr angiographic catheter only. Therefore, DIO is useful when selection of the guiding catheter is rather complicated such as in the case of congenital coronary anomalies.
Strong back-up support is one of the important determinants of PCI success. Generally, interventionists obtain back-up support by selecting the most appropriate French size or shape of the guiding catheter. In previous reports this was accomplished with a 7 or 8 Fr guiding catheter or a back-up shape (ie, Amplatz curve) guiding catheter.5-10 The 7 or 8 Fr guiding catheter is rigid and it cannot be manipulated well; also, an Amplatz guiding catheter may not be injected coaxially in this case. The DIO allows coronary angiography and engages the coronary artery coaxially because of its softness. Moreover, strong back-up support can be obtained by engaging it deeply. The DIO catheter enables balloon delivery, intravascular ultrasound, and stenting of the distal portion of a vessel.
Successful PCI of anomalous coronary arteries relies on optimal guiding catheter seating and back-up support. The method described here will increase the likelihood of technical success when coming across different cases of RCA takeoff. This DIO guiding catheter method is less rigid than the 8 Fr guiding system, and it allows for greater manipulation of the guiding catheter. Deep engagement can provide strong back-up support.
Conclusion
The DIO thrombus aspiration catheter is useful when selection of a guiding catheter is rather complicated such as in the case of congenital coronary anomalies.
References
- Click RL, Holmes DR Jr, Vlietstra RE, Kosinski AS, Kronmal RA. Anomalous coronary arteries: location, degree of atherosclerosis and effect on survival--a report from the Coronary Artery Surgery Study. J Am Coll Cardiol. 1989;13(3):531-537.
- Kimbiris D, Iskandrian AS, Segal BL, Bemis CE. Anomalous aortic origin of coronary arteries. Circulation. 1978;58(4):606-615.
- Engel HJ, Torres C, Page HL Jr. Major variations in anatomical origin of the coronary arteries: angiographic observations in 4,250 patients without associated congenital heart disease. Cathet Cardiovasc Diagn. 1975;1(2):157-169.
- Leberthson RR, Dinsmore RE, Bharati S, et al. Aberrant coronary artery origin from the aorta. Diagnosis and clinical significance. Circulation. 1974;50(4):774-779.
- Topaz O, DiSciascio G, Goudreau E, et al. Coronary angioplasty of anomalous coronary arteries: notes on technical aspects. Cathet Cardiovasc Diagn. 1990;21(2):106-111.
- Musial B, Schob A, de Marchena E, Kessler KM. Percutaneous transluminal coronary angioplasty of anomalous right coronary artery. Cathet Cardiovasc Diagn. 1991;22(1):39-41.
- Charney R, Spindola-Franco H, Grose R. Coronary angioplasty of anomalous right coronary arteries. Cathet Cardiovasc Diagn. 1993;29(3):233-235.
- Cohen MG, Tolleson TR, Peter RH, Harrison JK, Sketch MH Jr. Successful percutaneous coronary intervention with stent implantation in anomalous right coronary arteries arising from the left sinus of valsalva: a report of two cases. Catheter Cardiovasc Interv. 2002;55(1):105-108.
- Khambekar S, Hudson I, Kovac J. Percutaneous coronary intervention to anomalous right coronary artery and retained piece of guidewire in the coronary vasculature. J Interv Cardiol. 2005;18(3):201-204.
- Lee BI, Gist HC Jr, Morris EI. Percutaneous coronary artery stenting of an anomalous right coronary artery with high anterior takeoff using standard size 7 French left Judkins guiding catheters. J Invasive Cardiol. 2003;15(11):682-684.
_______________________________________________________
From the Department of Cardiology, Dokkyo Medical University Koshigaya Hospital, Koshigaya City, Saitama, Japan.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript submitted November 4, 2011, provisional acceptance given November 22, 2011, final version accepted December 5, 2011.
Address for correspondence: 2-1-50 Minami-koshigaya, Koshigaya City, Saitama, Japan. Email: takaaki_km2@yahoo.co.jp











