

Transcatheter Closure of Patent Arterial Duct With Amplatzer Duct Occluder II Additional Sizes in Children
Download a PDF of this article.
Abstract: Amplatzer Duct Occluder II Additional Sizes is a new generation of device for arterial duct closure, appropriate for infants and older children. We report the successful transcatheter closure of the arterial duct in an infant and two older children with the above-mentioned device.
J INVASIVE CARDIOL 2013;25(2):96-97
Key words: patent duct, closure, device
________________________________________
Over the last two decades, there has been available large clinical experience on transcatheter closure of patent duct. Non-surgical closure of the duct remains challenging, especially in small infants. The Amplatzer Duct Occluder II is convenient for some cases, but the large retention discs can cause stenosis or partial obstruction of the pulmonary artery or the aorta.
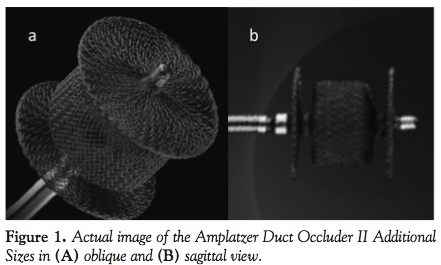 The Amplatzer Duct Occluder II Additional Sizes device has been designed to overcome these limitations in some cases. It is the next-generation device for arterial duct closure, with low-profile features, end screw, and a delivery system designed to accommodate smaller vasculature. It is made of a single-layer, flexible nitinol wire mesh shaped into a cylindrical waist with retention discs on either end (Figure 1). It can treat ducts at least 3 mm in length and less than 4 mm in diameter.
The Amplatzer Duct Occluder II Additional Sizes device has been designed to overcome these limitations in some cases. It is the next-generation device for arterial duct closure, with low-profile features, end screw, and a delivery system designed to accommodate smaller vasculature. It is made of a single-layer, flexible nitinol wire mesh shaped into a cylindrical waist with retention discs on either end (Figure 1). It can treat ducts at least 3 mm in length and less than 4 mm in diameter.
Case 1
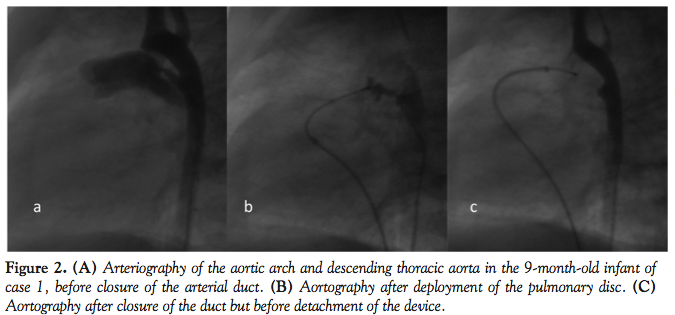 A 9-month-old, 5.6 kg, male infant was symptomatic, with recurrent chest infections and failure to thrive. Clinical examination revealed a loud systolic murmur audible over the upper left sternal edge and left subclavian border. Chest x-ray revealed cardiomegaly with increased pulmonary vascularity and echocardiogram showed dilated left atrium and ventricle. Cardiac catheterization revealed a moderate patent arterial type A, 6-mm long duct. The aortic end diameter was 5 mm and pulmonary end diameter was 2.5 mm (Figure 2A). Main pulmonary artery pressure was mild to moderately increased (systolic-diastolic-mean): 42-14-26 mm Hg, while the ascending aortic pressure was 86-38-54 mm Hg.
A 9-month-old, 5.6 kg, male infant was symptomatic, with recurrent chest infections and failure to thrive. Clinical examination revealed a loud systolic murmur audible over the upper left sternal edge and left subclavian border. Chest x-ray revealed cardiomegaly with increased pulmonary vascularity and echocardiogram showed dilated left atrium and ventricle. Cardiac catheterization revealed a moderate patent arterial type A, 6-mm long duct. The aortic end diameter was 5 mm and pulmonary end diameter was 2.5 mm (Figure 2A). Main pulmonary artery pressure was mild to moderately increased (systolic-diastolic-mean): 42-14-26 mm Hg, while the ascending aortic pressure was 86-38-54 mm Hg.
We used the Amplatzer Duct Occluder II Additional Sizes 5-4, which was placed via the venous route through a 4 Fr sheath. Device length was 4 mm, waist diameter was 5 mm, and diameter of each retention disc was 6.5 mm. There was no residual shunt immediately after placement of the device (Figure 2B). After deployment, we recorded withdrawal pressure in the descending aorta and pulmonary artery to rule out stenosis (Figure 2C). Total fluoroscopy time was 12 minutes. The infant was discharged 1 day after implantation and chemoprophylaxis for bacterial endocarditis was suggested for 1 year after.
Case 2
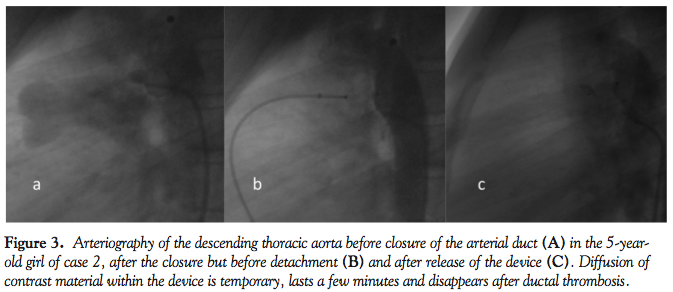 A 5-year-old asymptomatic girl presented with continuous murmur at left subclavian border and clinical examination otherwise unremarkable. Her chest x-ray was normal upon admission and transthoracic echocardiogram showed normal left atrial and left ventricular dimensions. Aortography revealed a patent, type E duct, 5.9-mm long with 3.8 mm internal diameter and narrowed pulmonary end with 2 mm diameter (Figure 3A).
A 5-year-old asymptomatic girl presented with continuous murmur at left subclavian border and clinical examination otherwise unremarkable. Her chest x-ray was normal upon admission and transthoracic echocardiogram showed normal left atrial and left ventricular dimensions. Aortography revealed a patent, type E duct, 5.9-mm long with 3.8 mm internal diameter and narrowed pulmonary end with 2 mm diameter (Figure 3A).
Use of the Amplatzer Duct Occluder II Additional Sizes 5-4 from the pulmonary side successfully closed the duct. An aortogram immediately after the release of the pulmonary disc with the device still attached to the delivery cable showed no residual shunt (Figure 3B).
Pull-back pressure measurements were obtained in the aortic arch and pulmonary artery before ending the procedure (Figure 3C). Total fluoroscopy time was 13 minutes.
Case 3
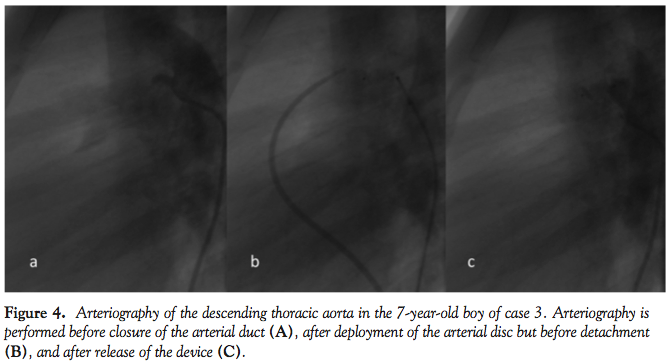 A 7-year-old boy presented with non-silent patent duct, but normal chest x-ray and normal left cardiac cavity dimensions. Aortography showed a long, tubular patent duct, type E, with narrowing at the pulmonary end. Duct length was 6.9 mm, maximal internal diameter was 3.1 mm, and diameter at pulmonary end was 1.5 mm (Figure 4A).
A 7-year-old boy presented with non-silent patent duct, but normal chest x-ray and normal left cardiac cavity dimensions. Aortography showed a long, tubular patent duct, type E, with narrowing at the pulmonary end. Duct length was 6.9 mm, maximal internal diameter was 3.1 mm, and diameter at pulmonary end was 1.5 mm (Figure 4A).
We selected the Amplatzer Duct Occluder II Additional Sizes 5-6 (device length, 6 mm; waist diameter, 5 mm; diameter of each retention disc, 6.5 mm). Due to suboptimal insertion of the duct in the main pulmonary artery, it was difficult to introduce the catheter from the pulmonary side. Instead of making an arteriovenous loop, we preferred to deliver the device from the arterial end of the ampulla (Figure 4B). After detachment, there was no residual shunt and no withdrawal pressure gradient at the isthmus (Figure 4C). Total fluoroscopy time was 8 minutes.
Discussion
Thirty-four years after the first report for non-surgical closure of patent arterial duct,2 it is now a routine first choice method. Every duct in adults and children beyond the first year of life, or the seventeenth month according to some authors, can be closed by intervention.
Nevertheless, large ducts in small children less than 8 kg remain a challenge. Their treatment may be difficult due to mismatch of introducers and/or occluders to the small anatomic dimensions.3 An answer to this problem has been given in some cases of children with body weight more than 6.3 kg and duct wider than 3 mm by the Amplatzer Duct Occluder II.4
The Amplatzer Duct Occluder II Additional Sizes has retention discs with very low profile and is especially useful in small infants, less than 6 kg, with ductal length more than 3 mm and diameter less than 4 mm, as with the infant in case 1.
In older children with duct diameter more than 3 mm, coils are not an effective treatment.5 Amplatzer Duct Occluder II is a safe and effective occluder, with advantages of its use including smaller sheath sizes and softer shape than other occluders. In some cases, though, the aortic disc protrudes into the aortic isthmus and can cause stenosis.6 In our cases of older children, the discs and screw of the Amplatzer Duct Occluder II Additional Sizes did not protrude into the great arteries even after deployment from the aortic end. It has gained the CE mark for use in Europe, but is not yet approved by the Food and Drug Administration for use in the United States.
Conclusion
The present cases illustrate that the Amplatzer Duct Occluder II Additional Sizes is a new-generation ductal occluder with low-profile discs that do not protrude in the aorta and pulmonary artery when properly positioned. The softer shape and small delivery system make it suitable for low body weight infants.
References
1. Amplatzer duct occluder. AGA Medical Corporation. URL:https://www.amplatzer.com/USProducts/PDADevice/tabid/193/Default.aspx
2. Porstmann W, Wiemy L, Warnke H. Closure of the persistent ductus arteriosus without thoracotomy. Ger Med Mon. 1967;12Q:259-261.
3. Ewert P. Challenges encountered during closure of patent ductus arteriosus. Pediatric Cardiol. 2005;26(3):224-229.
4. Dua J, Chessa M, Piazza L, et al. Initial experience with the new Amplatzer duct occluder II. J Invasive Cardiol. 2009;21(8):401-405.
5. Fu YC, Hwang B, Jan SL, et al. Influence of ductal size on the results of transcatheter closure of patent ductus arteriosus with coils. Jpn Heart J. 2003;44(3):395-401.
6. Saliba Z, El-Rassi I, Abi-Warde MT, et al. The Amplatzer duct occluder II: a new device for percutaneous ductus arteriosus closure. J Interv Cardiol. 2009;22(6):496-502.
__________________________________________
From the Department of Pediatric Cardiology, ‘Agia Sofia’ Children’s Hospital, Athens, Greece.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript submitted April 14, 2012, provisional acceptance given July 13, 2012, final version accepted July 26, 2012.
Address for correspondence: Nikolaos G. Eleftherakis, Department of Pediatric Cardiology, ‘Agia Sofia’ Children’s Hospital, Thivon and Papadiamantopoulou St, 115 27, Goudi, Athens, Greece. Email: ngeleftherakis@hotmail.com












