

Transfemoral Aortic Valve Implantation in a Renal Transplant Patient With a Dacron Aorto-bi-iliac Bypass
Abstract: Transcatheter aortic valve implantation (TAVI) is becoming the standard of care for inoperable patients with symptomatic severe aortic stenosis and the transfemoral approach is generally the first option chosen. However, transfemoral aortic valve replacement is contraindicated in patients with a Dacron aorto-bi-iliac bypass. To the best of our knowledge, we present the first case report of transfemoral aortic valve implantation in a kidney transplant patient with a history of aorto-bi-iliac bypass. His predicted operative mortality of 45% for aortic valve replacement was prohibitive according to the Society of Thoracic Surgeons score. A 26 mm Sapien XT valve (Edwards) was successfully implanted. Inotropic support was required for the four days following the procedure, after which, he was weaned uneventfully. A permanent pacemaker implantation was necessary at day six to treat a symptomatic paroxysmal complete atrio-ventricular block. The patient made an excellent recovery with no further complications and has remained asymptomatic at six months. This case highlights the importance of a detailed anatomic vascular assessment combined with a multidisciplinary evaluation of the access site in patients evaluated for TAVI. We used multi-slice computed tomography scans of the ilio-femoral arteries, the aorto-bi-iliac bypass and the thoraco-abdominal aorta to predict the potential pitfalls of a fully percutaneous transfemoral aortic valve implantation. The transfemoral approach was finally chosen in this case after considering the patient’s suitable aorto-ilio-femoral vasculature, his patent coronary artery bypass grafts and his predisposition for severe acute kidney injury.
J INVASIVE CARDIOL 2012;24(12):667-670
Key words: aortic stenosis, transcatheter aortic valve implantation, kidney transplantation, abdominal aortic aneurysm surgery
____________________________________________
Transcatheter aortic valve implantation (TAVI) is becoming the standard of care for inoperable patients with symptomatic severe aortic stenosis and is also an alternative for patients at high risk for conventional surgery, particularly in cases of predictably complex redo sternotomies.1-5 The transfemoral approach is generally the first option chosen considering its lower risk of acute kidney injury requiring temporary dialysis and its lower morbidity compared to transapical access that requires general anesthesia.6-11 However, there are still patients whose vasculature is unsuitable for transfemoral TAVI. Such patients include those with a history of aorto-bi-iliac bypass, which is currently a contraindication for a transfemoral approach. However, there is no evidence in the literature to support this assumption.12,13 Trans-axillary, trans-aortic and trans-carotid aortic valve replacements have been developed to make TAVI possible even in cases of severe lower extremity arterial disease, particularly when a transapical approach is not optimal. In recent reports, the TAVI procedures were performed using these alternative access sites because of history of aorto-bi-iliac bypass.14,18 To the best of our knowledge, we report the first case of successful 26 mm Sapien XT transfemoral aortic valve implantation (Edwards Lifesciences) in a kidney transplant patient with a history of Dacron aorto-bi-iliac bypass.
Case Description
A 78-year-old male was evaluated for aortic valve replacement because of severe aortic stenosis responsible for chronic congestive heart failure (NYHA stage III). His past medical history included hypertension, dyslipidemia and an ischemic cardiopathy treated by aorto-coronary artery bypass grafts five years before presentation (a left internal mammary artery to left anterior descending artery with a Y anastomosis of a free right internal mammary artery that sequentially bypassed a marginal branch and the right coronary artery system). The grafts were patent on preoperative coronary angiography. Twenty years prior to presentation, he underwent a Dacron aorto-bi-iliac bypass for an abdominal aortic aneurysm. The last noteworthy clinical element was a 16-year-old kidney graft implanted on his left iliac artery. One year earlier, he underwent angioplasty with stent implantation (Genesis 7 x 24 mm, Johnson and Johnson) on his left common iliac artery upstream of the arterial anastomosis graft due to a significant stenosis that was causing progressive resistant hypertension and kidney function degradation. At referral, transthoracic echocardiography demonstrated a heavily calcified tricuspid aortic valve (mean aortic gradient of 33 mmHg, valve area of 0.59 cm2, peak velocity of 3.7 m/s), a left-ventricular ejection fraction of 35%-40% with global hypokinesia, moderate degenerative organic mitral regurgitation and 66 mm Hg pulmonary hypertension. Contractile reserve was present and the valve area remained unchanged during dobutamine echocardiography. The predicted mortalities calculated by the Logistic European System for Cardiac Operative Risk Evaluation and by the Society of Thoracic Surgery score were 49% and 45%, respectively.
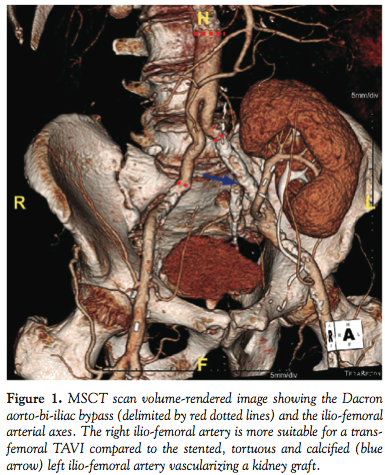
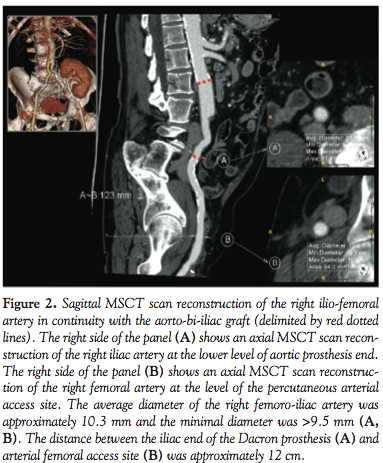
Laboratory results were notable for serum creatinine, with a value of 120 µmol/l. Because of his prohibitive high surgical risk and patent aorto-coronary grafts, the patient was scheduled for TAVI by the cardiovascular team. A multidisciplinary case meeting was held to determine the best approach. The team had experience with percutaneous transfemoral, direct aortic, transcarotid, and transapical approaches of aortic valve implantations. For this case, the transfemoral option with a percutaneous closure device was selected according to a properly-sized (>9.5 mm), straight and slightly calcified right common femoral artery and aorto-bi-iliac bypass (Figures 1 and 2).
As determined by a baseline multislice computed tomography scan (MSCT scan), the aortic annulus size measured 22 x 23 mm (Figure 3) and was suitable for a 26 mm Sapien XT aortic valve, as previously described.19 The patient was informed about the procedure and provided his consent. The procedure was performed under mild systemic sedation and local anesthesia by a completely percutaneous approach. A transvenous pacing wire (St Jude 6 Fr) was secured into the right ventricular apex before the TAVI. Puncture of the anterior wall of the right common femoral artery was ensured by non-selective ilio-femoral angiography from the contralateral side. After dilation of the tract to the right femoral artery with an 8 Fr dilator, the 10 Fr Prostar closure device (Abbott Vascular) was advanced over a 0.035-inch guidewire and deployed at a 45° angle. Heparin (70 IU/kg) was 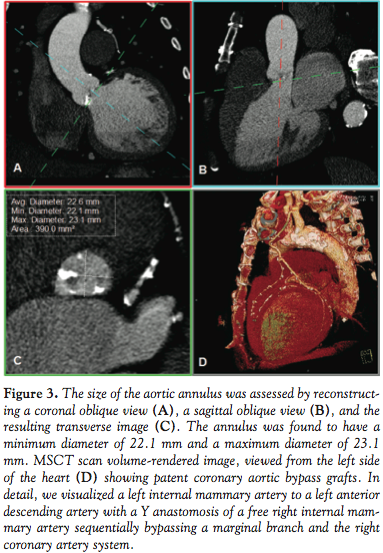 administeredintravenously before retrograde crossing of the aortic valve by the straight guidewire. A balloon catheter was inserted, and valvuloplasty was performed under rapid burst pacing using a 23-mm Edwards balloon. After balloon deflation, the rapid pacing was stopped and the balloon catheter was withdrawn. We then achieved progressive artery dilatation using dilatators with progressively larger diameters (14 Fr, 16 Fr, and 18 Fr). A 19 Fr sheath was then carefully inserted, and its progression was followed using fluoroscopic guidance. The 26 mm balloon-expandable Sapien XT valve was implanted during an episode of rapid ventricular pacing monitored by angiography real-time imaging and without the requirement for post-dilatation (Figure 4). The procedure lasted 80 min, with a fluoroscopy time of 29 min and an administered contrast volume of 154 cc (Iomeprol). The procedure was well-tolerated and the patient’s hemodynamics remained stable throughout. Control aortic angiography showed an
administeredintravenously before retrograde crossing of the aortic valve by the straight guidewire. A balloon catheter was inserted, and valvuloplasty was performed under rapid burst pacing using a 23-mm Edwards balloon. After balloon deflation, the rapid pacing was stopped and the balloon catheter was withdrawn. We then achieved progressive artery dilatation using dilatators with progressively larger diameters (14 Fr, 16 Fr, and 18 Fr). A 19 Fr sheath was then carefully inserted, and its progression was followed using fluoroscopic guidance. The 26 mm balloon-expandable Sapien XT valve was implanted during an episode of rapid ventricular pacing monitored by angiography real-time imaging and without the requirement for post-dilatation (Figure 4). The procedure lasted 80 min, with a fluoroscopy time of 29 min and an administered contrast volume of 154 cc (Iomeprol). The procedure was well-tolerated and the patient’s hemodynamics remained stable throughout. Control aortic angiography showed an 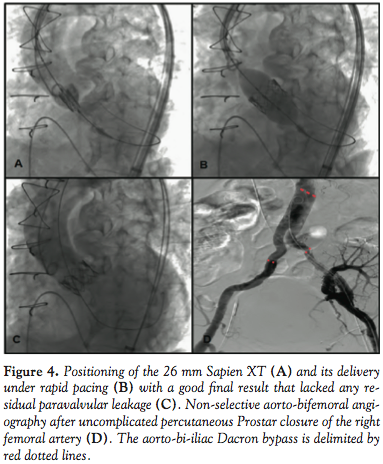 absence of any aortic leaks or complications (Figure 4). Following heparin reversal, the valve delivery sheath was removed and the arteriotomy site was closed efficiently with the Prostar sutures. Control non-selective aorto-bi-iliac arteriography was normal (Figure 4). The diagnostic arterial sheath on the left side was then removed and hemostasis was achieved by manual compression. Due to a per-procedure transient atrio-ventricular block, the venous sheath remained in-situ to provide pacing backup and the patient was referred to the intensive care unit. Transthoracic echocardiography performed after the procedure showed no periprosthetic aortic regurgitation, a low transprosthetic gradient (mean gradient of 5 mm Hg), and a lower ejection fraction of 15%. Dobutamine was necessary for four days, after which the patient was weaned uneventfully. The pacing wire was retrieved on day three. On day five, control echocardiography showed a 40% ejection fraction with a 9 mm Hg transprosthetic mean gradient. On day six, before being discharged, he presented with symptomatic paroxysmal complete atrioventricular block, which required implantation of a dual chamber permanent pacemaker (Sorin Reply DR). The patient was discharged to recover at home ten days after the procedure. He made an excellent recovery with no further complications and has remained asymptomatic during six months of follow-up.
absence of any aortic leaks or complications (Figure 4). Following heparin reversal, the valve delivery sheath was removed and the arteriotomy site was closed efficiently with the Prostar sutures. Control non-selective aorto-bi-iliac arteriography was normal (Figure 4). The diagnostic arterial sheath on the left side was then removed and hemostasis was achieved by manual compression. Due to a per-procedure transient atrio-ventricular block, the venous sheath remained in-situ to provide pacing backup and the patient was referred to the intensive care unit. Transthoracic echocardiography performed after the procedure showed no periprosthetic aortic regurgitation, a low transprosthetic gradient (mean gradient of 5 mm Hg), and a lower ejection fraction of 15%. Dobutamine was necessary for four days, after which the patient was weaned uneventfully. The pacing wire was retrieved on day three. On day five, control echocardiography showed a 40% ejection fraction with a 9 mm Hg transprosthetic mean gradient. On day six, before being discharged, he presented with symptomatic paroxysmal complete atrioventricular block, which required implantation of a dual chamber permanent pacemaker (Sorin Reply DR). The patient was discharged to recover at home ten days after the procedure. He made an excellent recovery with no further complications and has remained asymptomatic during six months of follow-up.
Discussion
This case highlights that transfemoral TAVI is possible in a patient with a history of Dacron aorto-bi-iliac bypass. Considering the risk of blocked progression of the transcatheter valve through the aortic-bi-iliac prosthesis and the fragile zone of suture between the Dacron material and the diseased arterial tissue, a history of aortic bypass has been considered to be a contraindication for transfemoral TAVI.12,13 This has led to the application of alternative vascular approaches such as transaxillary, transcarotid, transapical or direct aortic procedures.14-17 Aortic valve stenosis is essentially a disease of the elderly, who usually present with concomitant calcification and disease of the abdominal aorta and the peripheral arteries. Associations between frank aortic stenosis and abdominal aortic aneurysms were present in approximately 5% of the 3195 patients treated by TAVI in the FRANCE registry.20 Surgical aorto-bi-iliac bypass is a therapeutic option to cure abdominal aortic aneurysms and in the management of obstructive arterial disease in the lower extremities.21 Thus, patients referred for TAVI who have patent aorto-bi-iliac protheses are likely to be encountered in clinical practice. To date, the management of inoperable patients with symptomatic aortic stenosis and concomitant untreated abdominal aortic aneurysm has been the focus of several case reports.22-26 In all these cases, the cardiac burden was treated first. The transfemoral TAVI approach was avoided in almost all of these patients as other access sites were used. Nevertheless, the abdominal aortic aneurysms were subsequently cured. In one case, a percutaneous endovascular repair was performed in the same operation.26 In three others, the abdominal aortic aneursym was treated surgically or by endovascular repair and was cured after a few weeks.22,24,25 In fact, the systolic and mean arterial pressure increases that occur after aortic stenosis treatment produce high levels of strain on the aneurysm walls, aggravating the risk of dilatation and rupture. Bruschi et al reported the case of a patient who died of an aneurysm rupture within hours after transfemoral aortic valve replacement.23 In this context, our report of successful transfemoral TAVI in an elderly patient with a history of aortic abdominal aneurysm cured by Dacron aorto-bifemoral bypass is relevant. MSCT scanning was a key element in the pre-TAVI assessment and provided unique 3D visualization of the arterial vasculature. In our patient, the right ilio-femoral artery and the aorto-iliac graft were not heavily calcified, were without significant tortuosity and were of accurate sizes. The sheath outer diameter-to-femoral artery diameter ratio27 was only 0.8, considering that a 19 Fr sheath was necessary to deliver the 26 mm Sapien XT bioprosthesis. The distal part of the Dacron prosthesis was approximately 12 cm from the right femoral arterial access site (Figure 2). This allowed a correct hemostasis to be performed using the Prostar closure device on the native arterial tissue. We avoided a transapical procedure in this case due to the patient’s altered ejection fraction and to the risk of acute kidney injury exacerbated by the presence of his kidney graft.
Conclusion
TAVI is becoming a care standard for inoperable patients with symptomatic severe aortic stenosis. When possible, a transfemoral approach is generally the favored option but it is considered to be contraindicated in patients with a history of aorto-bi-iliac bypass. In clinical practice, encountering patients with frank aortic stenosis and a history of aorto-bi-iliac bypass is not unusual. This case report demonstrates that transfemoral TAVI can be performed in a patient bearing a patent aorto-bi-iliac bypass after the vasculature has been thoroughly and accurately assessed by imaging.
Acknowledgment. We thank our multidisciplinary TAVI team: Dr N. Amabile, Dr A. Azmoun, Dr S. Ghostine, Mme S. Guiquerro, Dr R. Nottin, Dr R Ramadan, Dr F. Raoux, Dr X Troussier, Dr NT. To and Dr A Veugeois
References
- Leon MB, Smith CR, Mack M et al. Transcatheter aortic-valve implantation for aortic stenosis in patients who cannot undergo surgery. N Engl J Med 2010;363(17):1597-607.
- Smith CR, Leon MB, Mack MJ, et al. Transcatheter versus surgical aortic-valve replacement in high-risk patients. N Engl J Med. 2011;364(23):2187-2198.
- Kodali SK, Williams MR, Smith CR, et al. Two-year outcomes after transcatheter or surgical aortic-valve replacement. N Engl J Med. 2012;366(18):1686-1695.
- Makkar RR, Fontana GP, Jilaihawi H, et al. Transcatheter aortic-valve replacement for inoperable severe aortic stenosis. N Engl J Med. 2012;366(18):1696-1704.
- Holmes DR, Mack MJ, Kaul S, et al. 2012 ACCF/AATS/SCAI/STS expert consensus document on transcatheter aortic valve replacement: Developed in collaboration with the American Heart Association, American Society of Echocardiography, European Association for Cardio-Thoracic Surgery, Heart Failure Society of America, Mended Hearts, Society of Cardiovascular Anesthesiologists, Society of Cardiac Computed Tomography, and Society for Cardiovascular Magnetic Resonance. Catheter Cardiovasc Interv. 2012;79(7):1023-1082.
- Jilaihawi H, Chakravarty T, Weiss RE, et al. Meta-analysis of complications in aortic valve replacement: comparison of Medtronic-Corevalve, Edwards-Sapien and surgical aortic valve replacement in 8,536 patients. Catheter Cardiovasc Interv. 2012;80(1):128-138.
- Thomas M, Schymik G, Walther T, et al. One-year outcomes of cohort 1 in the Edwards SAPIEN Aortic Bioprosthesis European Outcome (SOURCE) registry: the European registry of transcatheter aortic valve implantation using the Edwards SAPIEN valve. Circulation. 2011;124(4):425-433,
- Figulla L, Neumann A, Figulla HR, et al. Transcatheter aortic valve implantation: evidence on safety and efficacy compared with medical therapy. A systematic review of current literature. Clin Res Cardiol. 2011;100(4):265-276.
- Lefèvre T, Kappetein AP, Wolner E, et al. One year follow-up of the multi-centre European PARTNER transcatheter heart valve study. Eur Heart J. 2011;32:148-57.
- Moat NE, Ludman P, de Belder MA, et al. Long-term outcomes after transcatheter aortic valve implantation in high-risk patients with severe aortic stenosis: the U.K. TAVI (United Kingdom Transcatheter Aortic Valve Implantation) Registry. J Am Coll Cardiol 2011;58(20):2130-2138.
- Kong WY, Yong G, Irish A. The incidence, risk factors and prognosis of acute kidney injury after transcatheter aortic valve implantation (TAVI). Nephrology. 2012;17(5):445-451.
- Vahanian A, Alfieri O, Al-Attar N, et al. Transcatheter valve implantation for patients with aortic stenosis: a position statement from the European Association of Cardio-Thoracic Surgery (EACTS) and the European Society of Cardiology (ESC), in collaboration with the European Association of Percutaneous Cardiovascular Interventions (EAPCI). Eur Heart J. 2008;29(11):1463-1470.
- Da Gama Ribeiro V, Vouga L, Markowitz A, et al. Vascular access in transcatheter aortic valve implantation. Int J Cardiovasc Imaging. 2011;27(8):1235-1243.
- Asgar AW, Mullen MJ, Delahunty N, et al. Transcatheter aortic valve intervention through the axillary artery for the treatment of severe aortic stenosis. J Thorac Cardiovasc Surg. 2009;137(3):773-775.
- Latsios G, Gerckens U, Grube E. Transaortic transcatheter aortic valve implantation: a novel approach for the truly “no-access option” patients. Catheter Cardiovasc Interv. 2010;75(7):1129-1136.
- Modine T, Lemesle G, Azzaoui R, Sudre A. Aortic valve implantation with the CoreValve ReValving System via left carotid artery access: first case report. J Thorac Cardiovasc Surg. 2010;140(4):928-929.
- Mouillet G, Desgranges P, Teiger E. Transcatheter aortic valve implantation when classical access routes are unavailable. Catheter Cardiovasc Interv. 2011;78(7):1004-1007.
- Latib A, Ielasi A, Montorfano M, et al. Transcatheter valve-in-valve implantation with the Edwards SAPIEN in patients with bioprosthetic heart valve failure: the Milan experience. EuroIntervention. 2012;7(11):1275-1284.
- Amabile N, Ramadan R, Ghostine S, et al. Early and mid-term cardiovascular outcomes following TAVI: Impact of pre-procedural transvalvular gradient. Int J Cardiol. 2012 Mar 27. [Epub ahead of print]
- Gilard M, Eltchaninoff H, Iung B, et al. Registry of transcatheter aortic valve implantation in high-risk patients. N Engl J Med. 2012;366(18):1705-1715.
- Tendera M, Aboyans V, Bartelink M-L, et al. ESC Guidelines on the diagnosis and treatment of peripheral artery diseases: Document covering atherosclerotic disease of extracranial carotid and vertebral, mesenteric, renal, upper and lower extremity arteries: the Task Force on the Diagnosis and Treatment of Peripheral Artery Diseases of the European Society of Cardiology (ESC). Eur Heart J. 2011;32(22):2851-2906.
- Taramasso M, Giacomini A, Maisano F. Transcatheter aortic valve implantation through the left subclavian artery with a patent LIMA graft. Catheter Cardiovasc Interv. 2010;76:153-155.
- Bruschi G, De Marco F, Fratto P, et al. Alternative approaches for trans-catheter self-expanding aortic bioprosthetic valves implantation: single-center experience. Eur J Cardiothorac Surg. 2011;39:151-158.
- Drury-Smith M, Garnham A, Khogali S. Sequential trans-catheter aortic valve implantation and abdominal aortic aneurysm repair. Catheter Cardiovasc Interv. 2012;79(5):784-788.
- Drury-Smith M, Garnham A, Khogali S. Critical aortic stenosis in a patient with a large saccular abdominal aortic aneurysm: simultaneous transcatheter aortic valve implantation and drive-by endovascular aortic aneurysm repair. Catheter Cardiovasc Interv. 2012 Mar 15. doi: 10.1002/ccd.23452. [Epub ahead of print]
- Ghosh-Dastidar M, Dworakowski R, Lioupis C, et al. The combined treatment of aortic stenosis and abdominal aortic aneurysm using transcatheter techniques: a case report. J Cardiovasc Surg (Torino). 2011;52(6):895-898.
- Hayashida K, Lefèvre T, Chevalier B, et al. Transfemoral aortic valve implantation new criteria to predict vascular complications. JACC Cardiovasc Interv. 2011;4(8):851-858.
___________________________________________
From the Departments of 1Interventional Cardiology and 2Radiology, Université Paris Sud, Centre Marie Lannelongue, Le Plessis Robinson, France.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript submitted May 7, 2012 and accepted July 6, 2012.
Address for correspondence: Joe-Elie Salem, MD, Department of Interventional Cardiology, Université Paris Sud, Centre Marie Lannelongue, 133 Av de la résistance, 92350 Le Plessis Robinson, France. Email: joeelie.salem@gmail.com










