

Transradial Retrograde Recanalization of Totally Occluded Left Anterior Descending Artery Using a Single 7 Fr Guiding Catheter
Download a PDF of this article.
Abstract: The retrograde approach for percutaneous coronary intervention (PCI) of chronic total occlusion (CTO) has helped to improve the success rate. It is usually performed through collateral connections that originate from the contralateral coronary artery to the occluded one and by using two arterial accesses and two guiding catheters, most commonly from the femoral approach.
A first reported case of epsilateral retrograde PCI to CTO of the left anterior descending artery (LAD) via the radial approach, using a single guiding catheter and through epsilateral collaterals originating from the LAD itself, is presented.
J INVASIVE CARDIOL 2013;25(1):57–60
Key words: chronic total occlusion, percutaneous coronary intervention, radial artery intervention, femoral intervention, coronary artery disease, septal collaterals, retrograde approach
_______________________________________________________
Percutaneous treatment of coronary total occlusion (CTO) remains one of the major challenges in percutaneous coronary intervention (PCI). Due to the perceived procedural complexity of PCI in CTOs, it still represents the most common reason for referral to bypass surgery, or for choosing medical treatment.1,2 Over the past few years, tremendous improvements in PCI equipment and materials, as well as the growth of new treatment strategies, have allowed us to tackle more complex CTO cases with success.
Percutaneous recanalization of CTO was first attempted in the 1980s. With increased operator experience and improved PCI materials and techniques, a success rate of between 50 and 70% could be achieved with the use of standard techniques. With the development of new equipment and techniques, the success rate is on the rise.3-6
In order to improve this still suboptimal success rate, the retrograde approach through collateral channels was introduced and is one of the most promising current techniques. It was used for the first time via a bypass graft7 and different strategies for this approach have been developed for successful outcome.8-11 The first technique introduced that used the retrograde approach was the retrograde wire technique, then the kissing wire technique, and more recently, the controlled antegrade and retrograde subintimal tracking (CART) technique. The retrograde approach requires a channel between the occluded coronary artery and another patent coronary artery, which enables the distal CTO site to be reached retrogradely. This intercoronary channel can be either an epicardial collateral, a septal collateral, or a bypass graft. Meticulous review of the angiography, frame by frame, frequently allows a suitable collateral channel to be identified. In most cases, septal collaterals are considered to be the most suitable.
The author reports a case of mid left anterior descending (LAD) artery CTO recanalization performed successfully via the radial artery, using a single guiding catheter and through epsilateral septal collateral to the distal LAD. This case is believed to be the first reported successful case of such an approach.
Case Report
A 63-year-old patient who is a smoker with a history of dyslipidemia and previous myocardial infarction was previously admitted with troponin-positive acute coronary syndrome (ACS) in early 2010; subsequent coronary angiography showed 3-vessel disease with occluded LAD in the mid course, severe stenosis in obtuse marginal (OM)1 and OM2, and a small non-dominant right coronary artery (RCA). His left ventricular function was moderately impaired and dobutamine stress echocardiogram showed viability in the LAD territory and ischemia in the left circumflex (LCX) territory; he was referred for coronary artery bypass grafting (CABG). He underwent CABG with left internal mammary artery (LIMA) to diagonal 1 (D1) as the LAD was deemed small and occluded, and vein graft (SVG) to OM1 and OM2. Three months later, he was re-admitted with ACS and repeat angiography showed all grafts to be occluded, of which SVG to OM1 appeared acute with a thrombus. This was recanalized and treated with drug-eluting stent (DES), with further DES at the insertion site with excellent results and a planned re-admission for PCI to the LAD/CTO.
The patient was re-admitted later and the procedure for LAD/CTO was performed from the radial artery using a 7 Fr Q4 guiding catheter (Boston Scientific) with clopidogrel 600 mg and aspirin 300 mg loading doses. Heparin 100 U/Kg was given at the start of the procedure with regular activated clotting time (ACT) monitoring during the procedure.
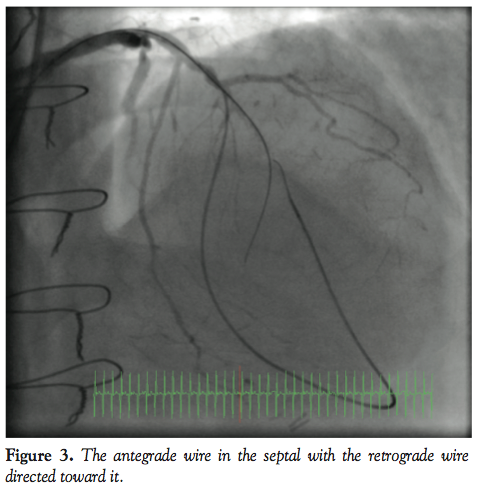
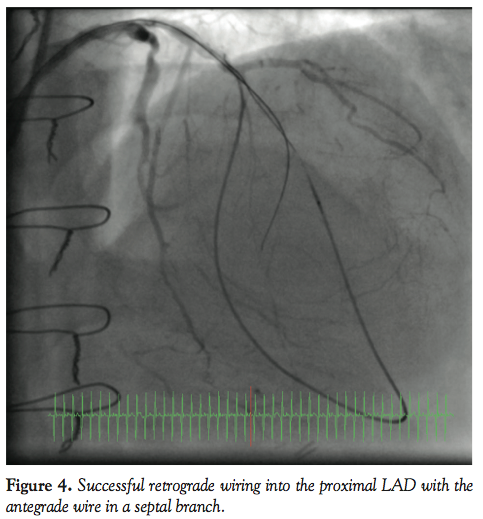
 Angiogram showed the LAD occlusion in the mid course with a septal collateral filling the distal LAD retrogradely (Figure 1). An angioplasty Sion wire with a Corsair catheter (Asahi Intecc Co Ltd) was introduced into the LAD and the septal collateral and distal LAD retrogradely and a Confianza Pro12 (Asahi Intecc) antegradely through the proximal occlusion cap (Figure 2). The anterograde wire was passed into a septal branch, which gave a road map for the retrograde wire. The retrograde Sion wire was exchanged for a Pilot 200 wire (Abbott) which was navigated retrogradely (Figure 3) and crossed the proximal occlusion cap followed by the Corsair catheter (Figure 4). Following that, a 300 cm RG3
Angiogram showed the LAD occlusion in the mid course with a septal collateral filling the distal LAD retrogradely (Figure 1). An angioplasty Sion wire with a Corsair catheter (Asahi Intecc Co Ltd) was introduced into the LAD and the septal collateral and distal LAD retrogradely and a Confianza Pro12 (Asahi Intecc) antegradely through the proximal occlusion cap (Figure 2). The anterograde wire was passed into a septal branch, which gave a road map for the retrograde wire. The retrograde Sion wire was exchanged for a Pilot 200 wire (Abbott) which was navigated retrogradely (Figure 3) and crossed the proximal occlusion cap followed by the Corsair catheter (Figure 4). Following that, a 300 cm RG3 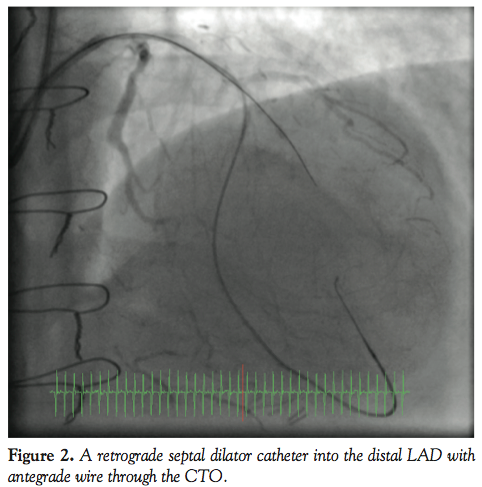 wire (Asahi Intecc) was externalized and the Corsair catheter removed with initial 1.5 balloon dilatation performed retrogradely (Figure 5). Further 2.0 balloon dilatation was performed antegradely and subsequently 2 Promus Element DESs (Boston Scientific) were deployed and the distal LAD was treated with plain old balloon angioplasty with the 2.0 balloon, with excellent final results (Figure 6). The patient tolerated the procedure well with no complications and was monitored on the ward and allowed home in a stable condition.
wire (Asahi Intecc) was externalized and the Corsair catheter removed with initial 1.5 balloon dilatation performed retrogradely (Figure 5). Further 2.0 balloon dilatation was performed antegradely and subsequently 2 Promus Element DESs (Boston Scientific) were deployed and the distal LAD was treated with plain old balloon angioplasty with the 2.0 balloon, with excellent final results (Figure 6). The patient tolerated the procedure well with no complications and was monitored on the ward and allowed home in a stable condition.
Discussion
 The most common cause of PCI failure in CTO is the inability of the wire to cross the CTO.12 The retrograde approach was introduced to overcome this difficulty and several strategies have been developed, demonstrating the efficacy and feasibility of the retrograde technique.8-11
The most common cause of PCI failure in CTO is the inability of the wire to cross the CTO.12 The retrograde approach was introduced to overcome this difficulty and several strategies have been developed, demonstrating the efficacy and feasibility of the retrograde technique.8-11
The art and technique of CTO PCI have been growing at an astounding rate and have led to the increase in the success rate into 90% among dedicated CTO operators.13
 The retrograde approach requires a special step in which a wire is passed retrogradely through the collateral channels with the support of a small size balloon or a microcatheter until it reaches the distal end of the CTO. The presence of suitable collateral is the key to the success of this approach. Collaterals for retrograde access can be septal or epicardial, and in the majority of cases they come from the contralateral artery.14 Epsilateral collaterals from the same artery are less common. Epicardial collaterals are seen in up to one-half of cases of CTO;15 they are very tortuous and make advancement of balloons or catheters difficult. Furthermore, even small perforations can lead to tamponade quickly. On the other hand, septal collaterals have generally shorter course and are less tortuous, and more importantly, their perforation does not pose a major risk as with epicardial ones. Therefore, septal channels are considered the ideal retrograde access.13-15
The retrograde approach requires a special step in which a wire is passed retrogradely through the collateral channels with the support of a small size balloon or a microcatheter until it reaches the distal end of the CTO. The presence of suitable collateral is the key to the success of this approach. Collaterals for retrograde access can be septal or epicardial, and in the majority of cases they come from the contralateral artery.14 Epsilateral collaterals from the same artery are less common. Epicardial collaterals are seen in up to one-half of cases of CTO;15 they are very tortuous and make advancement of balloons or catheters difficult. Furthermore, even small perforations can lead to tamponade quickly. On the other hand, septal collaterals have generally shorter course and are less tortuous, and more importantly, their perforation does not pose a major risk as with epicardial ones. Therefore, septal channels are considered the ideal retrograde access.13-15
 The majority of CTO PCIs are performed through the femoral approach with larger-sized guiding catheters due to the perception of inability to use such guiding catheters and the lack of support during the procedure via radial approach.16 There have been, however, publications showing the feasibility and safety of the radial artery approach for complex PCI with excellent results and outcomes.16
The majority of CTO PCIs are performed through the femoral approach with larger-sized guiding catheters due to the perception of inability to use such guiding catheters and the lack of support during the procedure via radial approach.16 There have been, however, publications showing the feasibility and safety of the radial artery approach for complex PCI with excellent results and outcomes.16
In this case, a 7 Fr radial approach was used and no continuous contralateral septal channel could be identified, but an epsilateral septal collateral was seen supplying the distal LAD. A single guiding catheter was used to advance the retrograde wire inside a septal dilatation 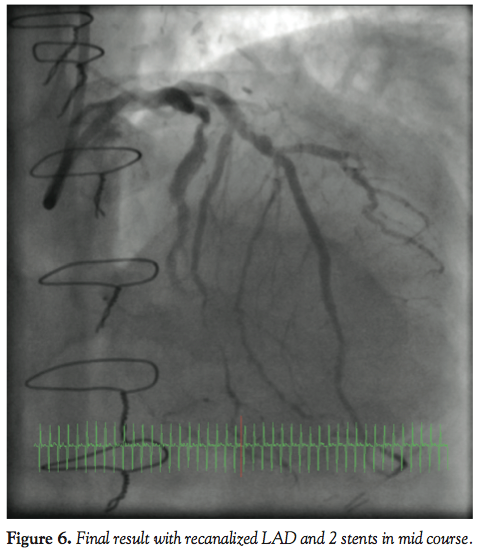 catheter, as well as an antegrade wire to help direct the retrograde one. The difficulty with this case and approach was encountered when advancing the septal dilator catheter back into the guiding catheter after crossing the distal CTO cap. The septal dilator catheter had to be stopped where it entered the septal channel antegradely (Figure 7), and this may lead to difficulty in externalizing the guidewire into the guiding catheter. Furthermore, when delivering balloons or stents, in the normal contralateral collaterals, the septal catheter is left in place to protect the ostium of the septal branch used and prevent cheese cutting into the coronary artery. In this case, however, this was not possible since the septal dilator needed to be removed to allow the delivery of balloons and stents and the wire needed to be monitored closely to prevent this side effect.
catheter, as well as an antegrade wire to help direct the retrograde one. The difficulty with this case and approach was encountered when advancing the septal dilator catheter back into the guiding catheter after crossing the distal CTO cap. The septal dilator catheter had to be stopped where it entered the septal channel antegradely (Figure 7), and this may lead to difficulty in externalizing the guidewire into the guiding catheter. Furthermore, when delivering balloons or stents, in the normal contralateral collaterals, the septal catheter is left in place to protect the ostium of the septal branch used and prevent cheese cutting into the coronary artery. In this case, however, this was not possible since the septal dilator needed to be removed to allow the delivery of balloons and stents and the wire needed to be monitored closely to prevent this side effect.
 To the author’s knowledge, this is the first reported case of using the radial approach for epsilateral retrograde approach for CTO PCI using a single guiding catheter and the simple retrograde wire approach.
To the author’s knowledge, this is the first reported case of using the radial approach for epsilateral retrograde approach for CTO PCI using a single guiding catheter and the simple retrograde wire approach.
There have been publications of ipsilateral retrograde approach, but with 2 guiding catheters,15 and another 2 cases of femoral approach and using CART and reverse CART techniques.16,17 No radial cases have been published with this approach.
Conclusion
In suitable anatomy, an epsilateral retrograde approach for CTO PCI is possible and can be performed safely through the radial approach with successful outcome as presented in this case.
References
- Bourassa MG, Roubin GS, Detre KM, et al. Bypass angioplasty revascularisation investigation: patient screening, selection, and recruitment. Am J Cardiol. 1995;75(9):3C-8C.
- King SB 3rd, Lembo NJ, Weintraub WS, et al. A randomised trial comparing coronary angioplasty with coronary bypass surgery. Emory angioplasty versus surgery trial (EAST). N Engl J Med. 1994;331(16):1044-1050).
- Hoye A, van Domgurg RT, Sonnenschien K, et al. Percutaneous coronary intervention for chronic total occlusion: the Thoraxcenter experience 1992-2002. Eur Heart J. 2005;26(24):2630-2636
- Saito S, Tanaka S, Hiroe Y, et al. Angioplasty for chronic total occlusion by using tapered-tip guidewires. Catheter Cardiovasc Interv. 2003;59(3):305-311.
- Hirokami M, Saito S, Muto H. Anchoring technique to improve guiding catheter support in coronary angioplasty of chronic total occlusion. Catheter Cardiovasc Interv. 2006;18(3):334-338.
- Lee NH, Cho YH, Seo HS. Successful recanalisation of in-stent coronary chronic total occlusion by subintimal tracking. J Invasive Cardiol. 2008;20(4):E129-E132.
- Kahn JK, Hartzler GO. Retrograde coronary angioplasty of isolated arterial segments through saphenous vein bypass grafts. Cathet Cardiovasc Diagn. 1990;20(2):88-93.
- Kukreja N, Serruys PW, Sianos G. Retrograde recanalisation of chronically occluded coronary arteries: illustration and description of the technique. Catheter Cardiovasc Interv. 2007;69(6):833-841.
- Surmely JF, Tsuchikane E, Katoh O, et al. New concept for CTO recanalisation using controlled antegrade and retrograde subintimal tracking. J Invasive Cardiol. 2006;18(7):334-338.
- Ozawa N. A new understanding of chronic total occlusion from a novel PCI technique that involves a retrograde approach to the right coronary artery via a septal branch and passing of the guidewire to a guiding catheter on the other side of lesion. Catheter Cardiovasc Intervent. 2006;68(6):907-913.
- Saito S. Different strategies of retrograde approach in coronary angioplasty for chronic total occlusion. Catheter Cardiovasc Interv. 2008;71(1):8-19.
- Noguchi T, Miyazaki S, Morii I, et al. Percutaneous transluminal coronary angioplasty of chronic total occlusions; determinants of primary success and long term clinical outcome. Catheter Cardiovasc Interv. 2000;49(3):258-264.
- Lombardi WL. Retrograde PCI: what will they think of next? J Invasive Cardiol. 2009;21(10):543.
- Surmely JF, Katoh O, Tsuchikane E, et al. Coronary septal collaterals as an access for the retrograde approach in the percutaneous treatment of coronary chronic total occlusions. Catheter Cardiovasc Interv. 2007;69(6):826-832.
- Lee NH, Suh J, Cho YH, et al. Recanalisation of a coronary chronic total occlusion by a retrograde approach using ipsilateral double guiding catheters. Korean Circ J. 2009;39:42-45.
- Egred M. Feasibility and safety of 7-Fr radial approach for complex PCI. J Interv Cardiol. 2011;24(5):383-388.
________________________________________
From the Cardiac Department, Freeman Hospital, Newcastle upon Tyne, United Kingdom.
Disclosure: The author has completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The author reports no conflicts of interest regarding the content herein.
Manuscript submitted April 30, 2012, final version accepted June 25, 2012.
Address for correspondence: Dr Mohaned Egred, BSc (Hons), MB ChB, MD, FRCP, FESC, Consultant Interventional Cardiologist & Honorary Senior Lecturer, Freeman Hospital & Newcastle University, Newcastle upon Tyne, NE7 7DN, United Kingdom. Email: m.egred@nuth.nhs.uk











