

Use of Orbital Atherectomy Treatment in a High-Volume Clinical Practice Modifies Non-Compliant Plaque to Deliver Durable Long-Term Results
Abstract: Background. Resistant fibrotic calcified plaque is a major limitation in treating peripheral arterial disease (PAD). Percutaneous transluminal angioplasty (PTA) balloon pressures of 8-16 atm are typically required in these lesions. Ultrasound has detected significant dissection or plaque fracture immediately after balloon dilation in 76% of patients. Endovascular techniques are available that remove calcified plaque and alter lesion compliance, which minimizes dissection and stenting. A single-center experience evaluating the long-term durability of calcified plaque removal utilizing orbital atherectomy is presented. Methods. Patients with PAD underwent primary intervention with orbital atherectomy followed by low-pressure balloon angioplasty. Lesion compliance markers, including balloon inflation pressures and times, dissection rates, and bail-out stent rates, were recorded. Twelve-month re-intervention rates were also tracked. Results. Forty-six patients (57 lesions) were treated. Average age was 71 years and 74% of the patients were male. Rutherford classification was 3 to 5 for all patients. Lesion locations were in the common femoral artery (9%), superficial femoral artery (56%), popliteal artery (19%), and tibial/peritoneal arteries (16%). Average pretreatment stenosis was 90%. Adjunctive PTA was utilized in 82.5% of the lesions. Mean maximum inflation pressure was 5 atm for a mean of 2.3 minutes. Mean residual stenosis was 11%. One dissection occurred and no bailout stenting was required. Five patients (10.9%) returned for target lesion re-treatment. Conclusion. Orbital atherectomy modifies calcified lesion compliance in resistant peripheral arterial plaques as demonstrated by low balloon inflation pressures of short duration. Bail-out stenting was eliminated. Results were durable and the re-intervention rate was low.
J INVASIVE CARDIOL 2013;25(2):85-88
Key words: atherosclerosis, critical limb ischemia, peripheral arterial disease, vascular disease
____________________________________________
Peripheral arterial disease (PAD) is an occlusive vascular condition typically caused by atherosclerosis. Atherosclerosis is one of the most common causes of preventable myocardial infarction, ischemic stroke, lower extremity amputations, and cardio-vascular death.1 An estimated 8 to 10 million Americans live with PAD, but only 25% are undergoing treatment.2,3 Because the prevalence of PAD increases progressively with age, PAD is a growing clinical problem.4 Mortality in patients with PAD is four times that of the age-adjusted non-PAD population.5
Studies of various arterial beds have demonstrated that plaque composition is strongly linked with plaque progression, vulnerability, and subsequent symptoms.6 Calcium deposits are frequent in PAD patients with advanced age, diabetes, renal insufficiency, hypertension, and a history of smoking.7 Calcified lesions are challenging to treat with traditional endovascular therapy such as percutaneous transluminal angioplasty (PTA). Balloon angioplasty and treatment with stents, which are prone to fracture, are often insufficient for the treatment of calcified lesions.8 Frequently, to displace the calcified plaque, PTA balloon inflation pressures of 8 to 16 atm are required. Ultrasound has detected significant localized calcium deposits in up to 74% of lesions and significant dissection or plaque fracture immediately after balloon dilation in up to 76% of patients.9 With dissection requiring an increased number of peripherally placed stents, particularly in femoropopliteal and infrapopliteal arteries, the number of in-stent restenosis (ISR) interventions is also increasing. ISR is an increasing clinical and technical problem in daily practice since there is no adequate treatment yet designed for ISR.
In recent years, atherectomy has emerged as an effective and safe procedure to modify various types of plaque in diseased peripheral arteries. The primary goal of lesion modification is enhancement of patency6 and elimination of bail-out stenting in order to preserve the opportunity for future treatment options. Atherectomy procedures are particularly helpful for treating blockages in arteries that occur around branches or in vessels that are not easily treated with stents.
A single-center experience investigating the safety and long-term efficacy of orbital atherectomy as the primary intervention for revascularization in non-compliant, calcified PAD lesions follows.
Methods
Patients diagnosed with PAD were enrolled in a prospective, single-center study at Community Hospital in Munster, Indiana. Patients were referred to our institution for claudication (ie, Rutherford classification 1 through 3) or critical limb ischemia (ie, Rutherford classification 4 and 5). Each patient’s PAD severity was evaluated at baseline according to the Rutherford classification. Lesion locations and characteristics were assessed by angiography and lesion severity was qualitatively determined by the investigator.
Orbital atherectomy was performed as the primary intervention utilizing the second generation Predator 360° Diamondback Orbital Atherectomy System (OAS; Cardiovascular Systems, Inc). The procedure was performed according to the manufacturer’s recommendations under fluoroscopic guidance. Crown size selection was determined by the severity of stenosis, lesion location, and the presence of adequate distal run-off (ie, ≥1 vessel). Nitroglycerin boluses of 200-400 mcg through the sheath were administered prior to initial crown rotation and after every treatment interval. Low speed (60,000 to 80,000 rpm) was utilized to initially pass the crown across the lesion. Subsequently, medium speed (90,000 to 130,000 rpm) and high speed (120,000 to 180,000 rpm) were utilized to improve lesion compliance, as needed. Treatment intervals were limited to 25-30 seconds and total treatment duration was limited to 5 minutes. When deemed necessary by the investigator, adjunctive low-pressure PTA was performed after the primary orbital atherectomy procedure. Monitored lesion compliance markers included maximum postorbital treatment balloon inflation pressures, balloon inflation times, dissection rates, and bail-out stent rates. Re-intervention rates were also tracked. All patients were followed for 12 months post procedure.
Results
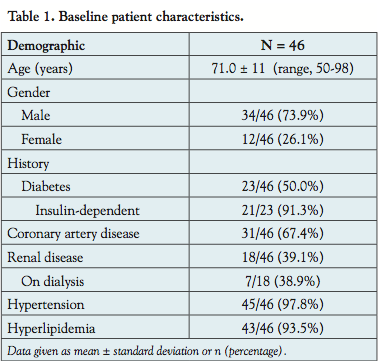 During the study period, a total of 57 fibrocalcific lesions were treated in 46 patients. Baseline patient characteristics are presented in Table 1. Most patients were male and the average age was 71 years. More than 90% of the patients had hypertension and hyperlipidemia. Half of all patients had diabetes and approximately two-thirds had coronary artery disease. The majority of patients (31/46; 67.4%) were Rutherford classification 3 with severe claudication, 5/46 (10.9%) were Rutherford classification 4 with ischemic pain at rest, and 10/46 (21.7%) exhibited tissue ulceration and were assigned Rutherford classification 5.
During the study period, a total of 57 fibrocalcific lesions were treated in 46 patients. Baseline patient characteristics are presented in Table 1. Most patients were male and the average age was 71 years. More than 90% of the patients had hypertension and hyperlipidemia. Half of all patients had diabetes and approximately two-thirds had coronary artery disease. The majority of patients (31/46; 67.4%) were Rutherford classification 3 with severe claudication, 5/46 (10.9%) were Rutherford classification 4 with ischemic pain at rest, and 10/46 (21.7%) exhibited tissue ulceration and were assigned Rutherford classification 5.
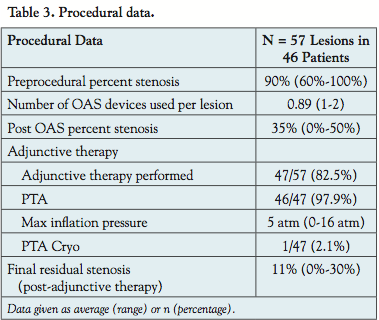
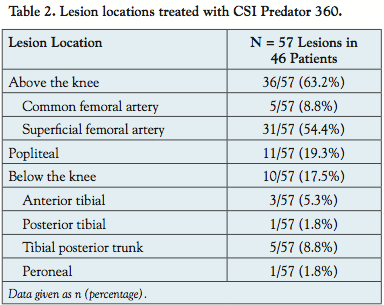 All patients had fluoroscopic evidence of calcified peripheral lesions. Arterial lesion locations undergoing orbital atherectomy treatment are presented in Table 2. On average, pre-treatment stenosis was 90% and ranged from 60% to 100%. The average number of OAS devices utilized per lesion was 0.89. The 2.00 mm Predator 360° crown was used in the superficial femoral artery (SFA) or popliteal region and the 1.5 mm and 1.25 mm crowns were used in all infrapopliteal lesions. Average stenosis after the primary OAS procedure was 35%. Use of a filter or distal protection was not needed. Adjunctive balloon PTA was necessary in 47/57 lesions (82.5%). Mean maximum balloon inflation pressure was 5 atm for a mean duration of 2.3 minutes (Table 3). Overall, final mean residual stenosis of 11% was achieved.
All patients had fluoroscopic evidence of calcified peripheral lesions. Arterial lesion locations undergoing orbital atherectomy treatment are presented in Table 2. On average, pre-treatment stenosis was 90% and ranged from 60% to 100%. The average number of OAS devices utilized per lesion was 0.89. The 2.00 mm Predator 360° crown was used in the superficial femoral artery (SFA) or popliteal region and the 1.5 mm and 1.25 mm crowns were used in all infrapopliteal lesions. Average stenosis after the primary OAS procedure was 35%. Use of a filter or distal protection was not needed. Adjunctive balloon PTA was necessary in 47/57 lesions (82.5%). Mean maximum balloon inflation pressure was 5 atm for a mean duration of 2.3 minutes (Table 3). Overall, final mean residual stenosis of 11% was achieved.
 Adverse events. Procedural complications occurred in 2/57 (3.5%) of the treated lesions (1 dissection, 1 spasm). The dissection successfully resolved after treatment with balloon inflation and the spasm resolved after administration of nitroglycerin. None of the patients experienced perforations, slow flow, closure, embolism, or thrombus. No bail-out stenting was required. Five patients (10.9%) returned for re-treatment of the target lesion within the 12-month follow-up period.
Adverse events. Procedural complications occurred in 2/57 (3.5%) of the treated lesions (1 dissection, 1 spasm). The dissection successfully resolved after treatment with balloon inflation and the spasm resolved after administration of nitroglycerin. None of the patients experienced perforations, slow flow, closure, embolism, or thrombus. No bail-out stenting was required. Five patients (10.9%) returned for re-treatment of the target lesion within the 12-month follow-up period.
Discussion
This single-center, prospective study investigated the safety and efficacy of primary OAS treatment in modifying calcified lesions of varying morphology in above the knee, popliteal, and below the knee locations. After modification of lesion compliance with orbital atherectomy, the majority of lesions (82.5%) were treated with adjunctive PTA. Vessel patency was restored with a final mean residual restenosis after adjunctive PTA of 11%. This investigation shows that patency can be significantly improved when orbital atherectomy is included in the treatment paradigm. Reported 12-month outcomes for femoropopliteal revascularization with traditional PTA and stenting show suboptimal patency rates of 61% and 67%, respectively.10 In comparison, the durability of the treatment during the 12-month follow-up period was favorable, with only 10.9% of the lesions requiring additional intervention while 89.1% did not receive additional treatment.
When PTA is the primary treatment, typical stent implantation rates range from 10%-43%.11 However, when orbital atherectomy is the primary treatment, stent implantation rates are only 0%-6%.11 No bail-out stents were required in this investigation. In contrast, a study comparing the SilverHawk directional atherectomy device and adjunctive PTA to primary PTA reported bail-out stenting in 62.1% of patients in the primary PTA arm versus 27.6% of patients in the atherectomy/adjunctive PTA arm.11
The use of orbital atherectomy as a primary intervention resulted in adjunctive PTA being performed at lower balloon inflation pressures. When PTA is used alone, higher balloon inflation pressures (8-16 atm) are generally required, which may result in damage to the vessel wall and related complications such as dissection, perforation, embolism, and thrombotic occlusion. In this investigation, orbital atherectomy allowed for lower balloon inflation pressures (mean, 5 atm) and a reduction in procedural complications was noted.
The incidence of complications noted in our study was found to be lower than incidence rates published in the literature. In this investigation, only 5 patients (10.9%) had restenosis at 12-month follow-up and required re-treatment, while typical 12-month PTA restenosis rates are approximately 40%.12,13 Fractures of femoropopliteal stents have been reported in 37.2% of patients with significantly lower primary patency at 12 months for patients with stent fractures (41.1%) compared to those patients without stent fractures (84.3%).14 Ultrasound has detected significant localized calcium deposits in up to 74% of lesions and significant dissection or plaque fracture immediately after balloon dilation in up to 76% of patients.9 Secondary bail-out stenting has occurred in more than 40% because of inadequate PTA results, either a flow-limiting dissection or a residual stenosis, after multiple balloon inflations.15 In contrast, only 1 dissection (1.8%) was observed in our study, which was promptly and successfully resolved with balloon inflation. Distal embolization has been estimated to range between 4% and 5% with peripheral percutaneous interventions.16 Furthermore, significant distal embolization has been reported with primary SilverHawk atherectomy (64.7%) compared to primary PTA (none).11 However, in our investigation, orbital atherectomy did not result in any embolization events and the use of a filter or distal protection was not needed.
It appears that the difference in the adverse event profile between the different interventions stems from the fundamentally different design of the orbital atherectomy device. Specifically, the design of the OAS and the eccentrically mounted crown allows the compliant vessel tissue to flex away from the crown and for fibrocalcific plaque, which provides resistance, to be differentially sanded off. Consequently, each pass of the crown modifies the calcified lesion. As the vessel wall becomes more compliant, the orbiting radius increases and the force applied to the vessel wall decreases. Only one part of the vessel wall is in contact with the sanding crown at any given time.7 This mechanism prevents heat generation, a potential cause of restenosis, and produces a smooth vessel lumen, improving the blood flow and lesion compliance.
The orbital atherectomy system design also results in particulate matter that is small in size and is removed from the body by the reticuloendothelial system. The particulate matter generated by the sanding action of the crown is approximately three times smaller than the diameter of a typical capillary.7 In orbital atherectomy, the particles created are continuously flushed with saline into the blood stream. Therefore, due to constant particle removal by the orbital atherectomy system, the likelihood of complications such as slow flow, embolism, and thrombus formation are decreased.
There is a growing body of evidence that points to the clinical and economic relevance of orbital technology to treat challenging lesions. Furthermore, use of the orbital atherectomy system in interventional procedures may prevent peripheral artery bypass surgery, enabling treatment with traditional, minimally invasive techniques.
One of the major limitations of this study is that it was a single-center study.
Conclusion
In this investigation, orbital atherectomy treatment with the Diamondback OAS, followed by low-pressure balloon angioplasty, produced desirable outcomes in modifying lesion compliance in difficult to treat resistant calcified and fibrotic plaques. Postorbital adjunctive balloon inflation pressures were low and of short duration. Bail-out stenting was eliminated in this challenging patient population. Long-term results were durable as evidenced by a low re-intervention rate at 12-month follow-up. Ultimately, orbital atherectomy is an effective and durable treatment modality that preserves limbs and does not preclude future treatment options.
References
- Rooke TW, Hirsch AT, Misra S, et al. American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines; Society for Cardiovascular Angiography and Interventions; Society of Interventional Radiology; Society for Vascular Medicine; Society for Vascular Surgery. 2011 ACCF/AHA focused update of the guideline for the management of patients with peripheral artery disease (updating the 2005 guideline): a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines: developed in collaboration with the Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society for Vascular Medicine, and Society for Vascular Surgery. J Vasc Surg. 2011;54(5):e32-e58. (Epub 2011 Sep 29).
- Rosamond W, Flegal K, Friday G, et al. Heart disease and stroke statistics — 2007 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2007;115(5):e69-e171. (Epub 2006 Dec 28).
- Hirsch AT, Hartman L, Town RJ, Virnig BA. National health care costs of peripheral arterial disease in the Medicare population. Vasc Med. 2008;13(3):209-215.
- Allaqaband S, Kirvaitis R, Jan F, Bajwa T. Endovascular treatment of peripheral vascular disease. Curr Probl Cardiol. 2009;34(9):359-476.
- Davies MG, Vykoukal D. Changing Paradigms in the Management of Peripheral Vascular Disease: The Need for Integration of Knowledge, Imaging, and Therapeutics. Computational Surgery and Dual Training. New York, New York: Springer Science+Business Media, LLC: 2010.
- Li F, McDermott MM, Li D, et al. The association of lesion eccentricity with plaque morphology and components in the superficial femoral artery: a high-spatial-resolution, multi-contrast weighted CMR study. J Cardiovasc Magn Reson. 2010;12:37. doi: 10.1186/1532-429X-12-37.
- Adams GL, Khanna PK, Staniloae CS, et al. Optimal techniques with the Diamondback 360° System achieve effective results for the treatment of peripheral arterial disease. J Cardiovasc Transl Res. 2011;4(2):220-229. (Epub 2011 Feb 11).
- Naidoo NG, Benningfield S. Claudication of the lower limb: an approach to investigation and management. Peripheral arterial disease is a relatively common cause of morbidity among men over 55 who have other risk factors for vascular disease. CME. 2009;27(7):301-305.
- Fitzgerald PJ, Ports TA, Yock PG. Contribution of localized calcium deposits to dissection after angioplasty. An observational study using intravascular ultrasound. Circulation. 1992;86(1):64-70.
- Dormandy JA, Rutherford RB. Management of peripheral arterial disease (PAD). TASC Working Group. TransAtlantic Inter-Society Consensus (TASC). (B4 Treatment of Intermittent Claudication S105 Table 21, S109 Table-24). J Vasc Surg. 2000;31(1 Pt 2):S1-S296.
- Shammas NW, Coiner D, Shammas GA, et al. Percutaneous lower-extremity arterial interventions with primary balloon angioplasty versus Silverhawk atherectomy and adjunctive balloon angioplasty: randomized trial. J Vasc Interv Radiol. 2011;22(9):1223-1228. (Epub 2011 Jul 14).
- Schillinger M, Mlekusch W, Haumer M, et al. Angioplasty and elective stenting of de novo versus recurrent femoropopliteal lesions: 1-year follow-up. J Endovasc Ther. 2003;10(2):288-297.
- Schillinger M, Haumer M, Schlerka G, et al. Restenosis after percutaneous transluminal angioplasty in the femoropopliteal segment: the role of inflammation. J Endovasc Ther. 2001;8(5):477-483.
- Scheinert D, Scheinert S, Sax J, et al. Prevalence and clinical impact of stent fractures after femoropopliteal stenting. J Am Coll Cardiol. 2005;45(2):312-315.
- Laird JR, Katzen BT, Scheinert D, et al; RESILIENT Investigators. Nitinol stent implantation versus balloon angioplasty for lesions in the superficial femoral artery and proximal popliteal artery: twelve-month results from the RESILIENT randomized trial. Circ Cardiovasc Interv. 2010;3(3):267-276. (Epub 2010 May 18).
- Lam RC, Shah S, Faries PL, et al. Incidence and clinical significance of distal embolization during percutaneous interventions involving the superficial femoral artery. J Vasc Surg. 2007;46(6):1155-1159.
________________________________________
From Community Healthcare System, Munster, Indiana.
Disclosure: The author has completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. Dr Makam is a shareholder of Cardiovascular Systems, Inc. He has no other conflicts of interest.
Manuscript submitted July 3, 2012, provisional acceptance given August 8, 2012, final version accepted October 1, 2012.
Address for correspondence: Prakash Makam, MD, FACC, FSCAI, Community Health Care System, Cardiovascular Research, Community Hospital, 901 MacArthur Blvd, Munster, IN 46321. Email: prakashmakam@comcast.net










