

Utility of Frequency Domain Optical Coherence Tomographic Evaluation of Angiographically Optimized Stented Lesions
Abstract: Background. Given its high resolution, optical coherence tomography (OCT) may be a useful clinical tool to optimize stent deployment. Methods. We reviewed 100 patients with post-PCI OCT who had angiographically optimized coronary stent implantation to determine the frequency of further intervention based on OCT pathology. OCT pathology was classified as “significant” if an OCT finding prompted further intervention. Results. OCT pathology was found in 90% of patients and considered significant in 52%. Stent strut malapposition by OCT was the most common reason for prompting further treatment, with approximately one-half due to relative stent undersizing. Based on OCT findings, 42% underwent balloon dilation, 9% underwent another stent implantation, and 3% underwent treatment with a glycoprotein IIb/IIIa inhibitor. Minor plaque protrusion was present in 11%, which prompted no further intervention. Conclusion. Post-PCI OCT in angiographically optimized vessels was helpful in improving stent deployment in more than one-half of the cases. Our findings suggest that post-PCI OCT may be a clinically useful tool in angiographically optimized stenting. Prospective studies will provide further clarity on the place of OCT in this setting.
J INVASIVE CARDIOL 2016;28(3):94-97
Key words: optical coherence tomography, coronary stenting, angioplasty
______________________________________________
It is universally agreed that optimizing stent deployment strongly influences short-term and long-term outcomes. Seminal studies using intravascular ultrasound (IVUS) demonstrated that angiographically optimized stents were often not fully expanded or apposed to the vessel wall,1 which in turn was related to the early incidence of stent thrombosis. Since high-pressure inflation was begun as a result of these studies, the incidence of stent thrombosis has markedly declined. Current IVUS technology is limited by its axial resolution of 100 microns. Whether more subtle degrees of incomplete stent expansion or strut malapposition not visible with IVUS can adversely affect outcomes is less certain. With the advent of optical coherence technology (OCT), which has an axial resolution of 10 microns, less extensive deployment issues may be determined. The current study reviewed our experience with OCT in stents that were felt to be optimally deployed angiographically and were subsequently evaluated by OCT.
Methods
Patient population. The current analysis was part of a quality improvement project to determine the frequency of optimal stent deployment using OCT (as the reference standard) after angiographically adequate stenting results. We had previously shown in a small group of patients that angiographically optimized stenting frequently showed underexpansion and malapposition, and that deployment parameters could be improved by prolonged high pressure using a standardized protocol.2 The current study comprised consecutive patients from Oct 1, 2011 to Dec 31, 2014 who had technically adequate OCT after de novo stent implantation that was considered to be angiographically optimized by the operator. The method of stent implantation was performed at the discretion of the operator. The patients studied by OCT were decided by each operator. Patients with ST-segment elevation myocardial infarction (MI), in-stent restenosis, and vein graft stenting were excluded from this analysis. Technically unsatisfactory OCT imaging was defined as lack of the entire stent being imaged, absence of healthy proximal reference segment, or poor image quality with attenuation due to inadequate blood clearing with the dye. The OCT run was performed after obtaining satisfactory stenting results based on angiography. If the OCT was performed to evaluate an angiographically visible post-PCI in-stent angiographic finding, it was excluded from analysis.
OCT image acquisition and image evaluation. OCT was performed using a frequency-domain OCT system (C7-XR OCT Imaging System; LightLab Imaging, Inc, St. Jude Medical). OCT runs were performed at a frame rate of 30 frames/s and pullback speed of 0.5 mm/s. Offline data analysis was performed after calibrating the machine with the reference catheter diameter.
Study definitions. OCT pathology was defined as an OCT imaging finding that was angiographically invisible, including malapposition, stent strut underexpansion, stent undersizing, plaque prolapse, edge dissection, in-stent thrombus, and an angiographically unappreciated severe stenosis. OCT pathology was classified as “significant” if it prompted further action (defined below). Stent strut malapposition was defined as a bare-metal stent strut greater than 100 microns or 140 microns for drug-eluting stent from the intimal surface.
Stent underexpansion was defined as a stent with strut-strut distance less than the diameter of the stent at nominal inflation pressure as provided by the manufacturer despite fully apposed struts. If the stent strut was malapposed in addition to being underexpanded, it was counted under malapposition and not stent underexpansion.
Stent undersizing as a cause of strut malapposition was defined as present if the nominal diameter of the stent was less than the proximal mean reference diameter (within 5 mm proximal of stent) and the entire proximal edge of the stent was malapposed.
Definitions of plaque prolapse, edge dissection, and in-stent thrombus were used as recommended by an international working group on consensus standards.2 A lesion unrecognized on angiography was defined as either a severely (>70%) stenotic segment proximal or distal to the deployed stent length or identification of an ulcerated lesion/crater as per the international working group definition.3
Action based on OCT pathology was defined as a stent optimization procedure or any subsequent intervention based on OCT findings. If a subsequent intervention was performed for clinical or angiographic reasons other than OCT finding, it was not counted as a subsequent action. Actions included stent postdilation, another stent implantation, treatment with addition of glycoprotein IIb IIIa inhibitors, and/or aspiration thrombectomy. If the patient had multiple pathologies identified on OCT imaging, then the pathology for which the action was being performed was counted in the analysis and that pathology was considered significant. For example, if a patient had strut malapposition and in-stent thrombus as the OCT pathology and the patient was subsequently treated with glycoprotein IIb/IIIa inhibitors alone, then only thrombus was considered significant and was counted as the reason for action based on OCT pathology.
Postdilation was defined as stent dilation performed after OCT imaging with high-pressure inflation of semicompliant stent balloon or a non-compliant balloon or the use of a larger non-compliant balloon (compared with stent diameter at nominal inflation pressure).
Statistical analyses. Demographics, baseline angiographic characteristics, frequency, and extent of malapposition were described by mean and standard deviation. Student’s t-test was used to compare means of independent continuous variables. All analyses were done using Microsoft Excel (Microsoft).
Results
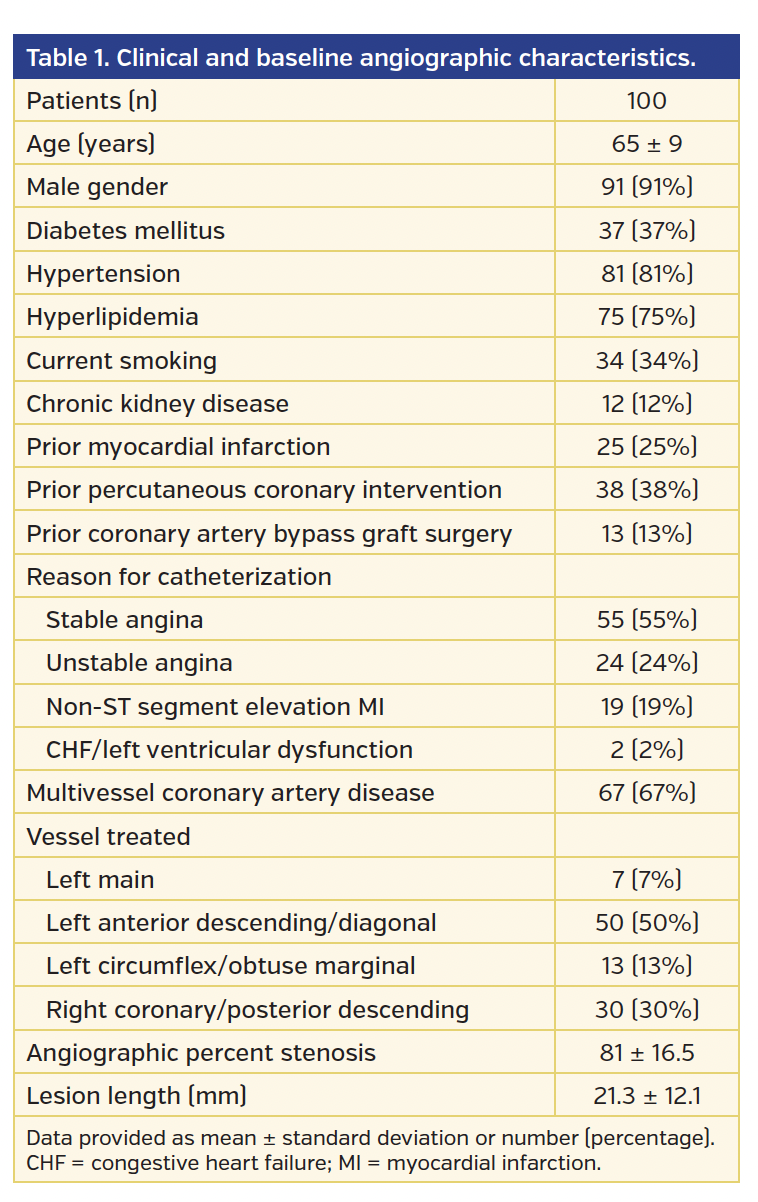
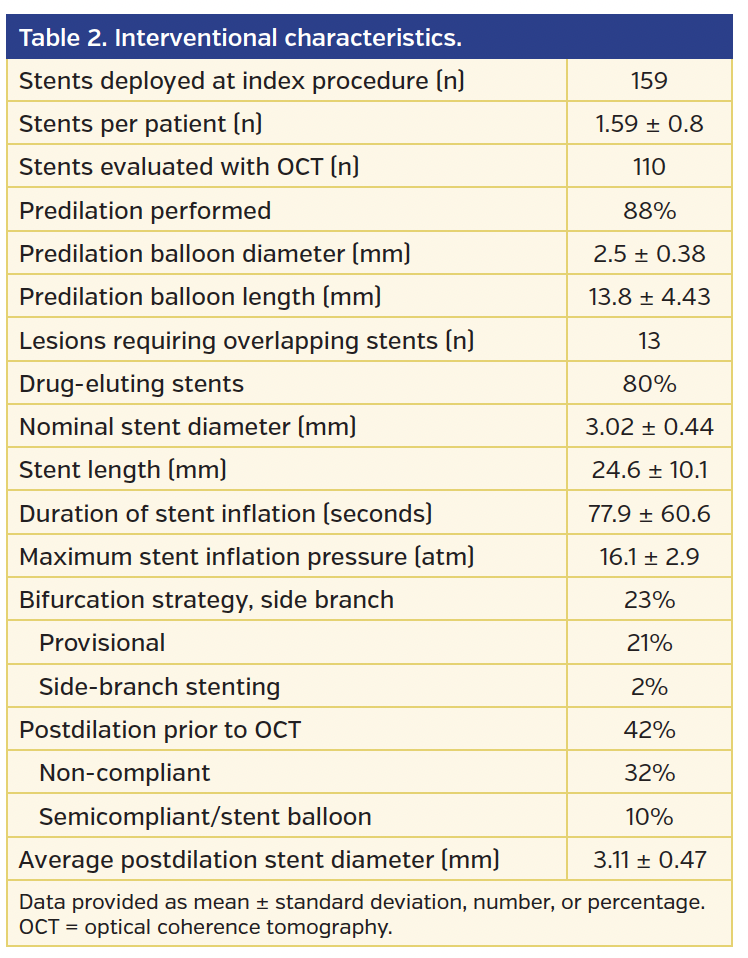
One hundred patients post stent deployment and angiographic optimization were evaluated by OCT. The 100 patients had 159 stents implanted, 110 of which were evaluated by OCT. The cohort was typical of patients with advanced coronary disease, as shown in Table 1. All stents were implanted successfully (Table 2) with essentially no residual angiographic stenosis prior to OCT evaluation. There was a high incidence of abnormal findings (90% of patients) (Table 3), with the most common being stent strut malapposition (Figure 1).
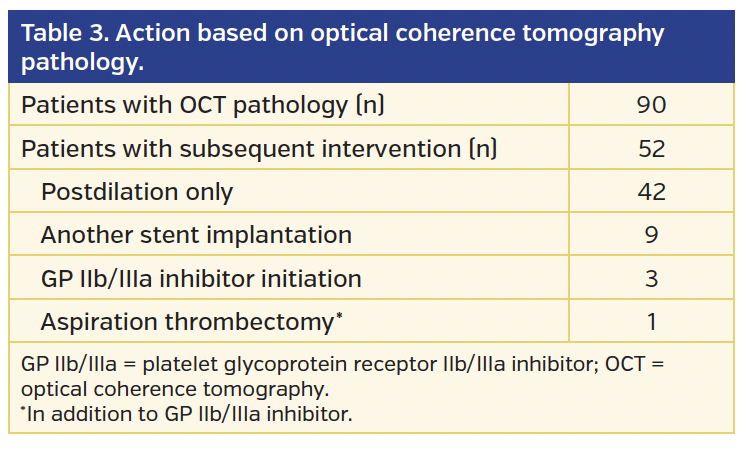
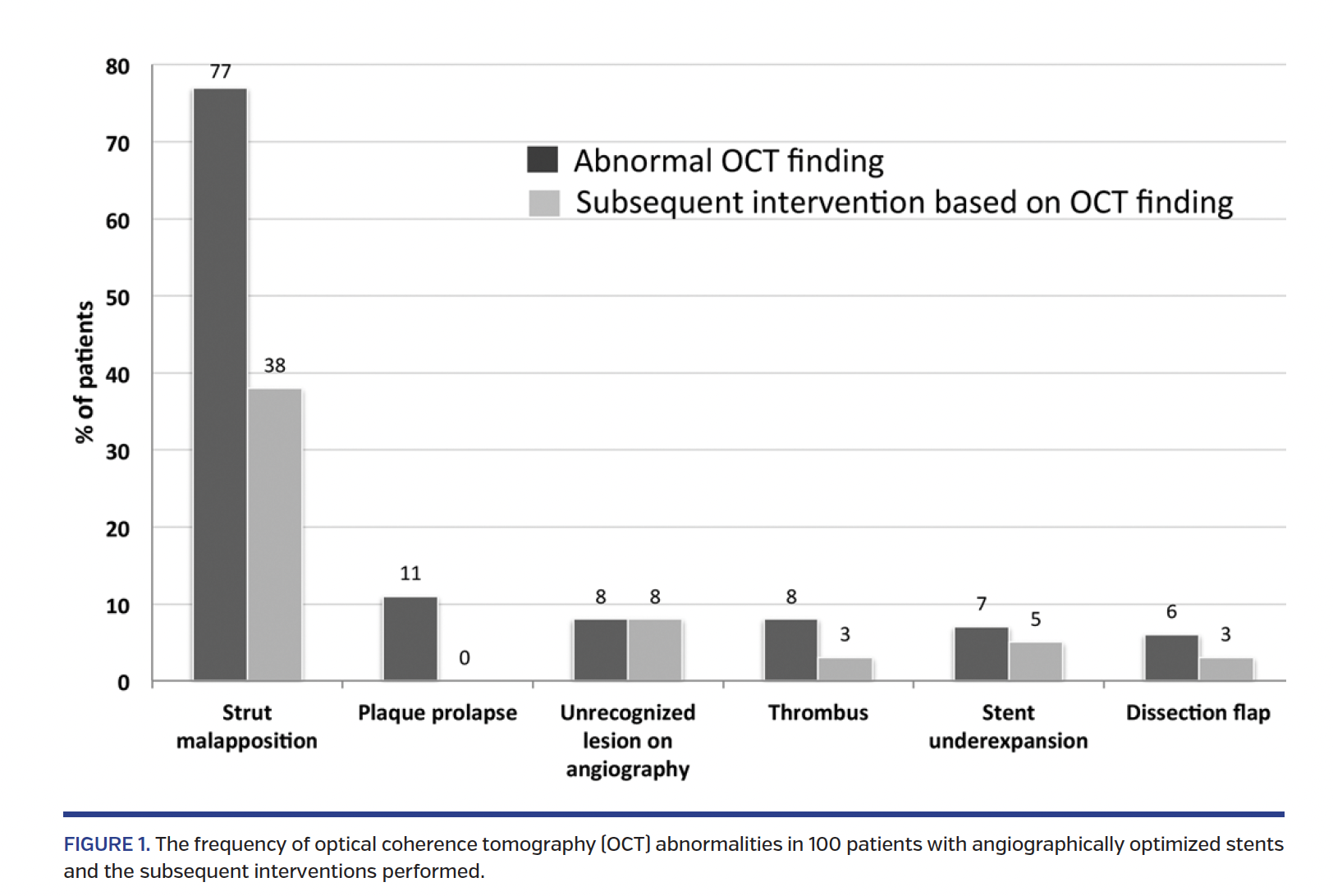
About one-half of patients (52%) undergoing OCT evaluation of stents with excellent angiographic appearance required further intervention or stent optimization (Table 3). Interventions are shown graphically in Figure 1. Stent undersizing was the cause of stent strut malapposition in 38 of 77 patients (49.3%). Twenty-one of 38 patients (55%) with stent undersizing had significant stent strut malapposition requiring postdilation with proximal stent segment optimization.
None of the 11 patients with plaque prolapse had substantial luminal narrowing prompting the operator to perform any further intervention. There were 8 severe unrecognized lesions on angiography observed by OCT in the adjacent proximal or distal vessel to the deployed stents. Seven of the 8 lesions were stented and 1 lesion was an in-stent restenosis in a previously implanted stent that underwent balloon dilatation. Five patients required postdilation of an underexpanded although adequately apposed stents. Two of 6 edge dissection flaps observed were treated with new stent deployment and 1 was treated with glycoprotein IIb/IIIa inhibitor infusion. In-stent thrombus was treated with glycoprotein IIb/IIIa inhibitor infusion (3 of 8 with observed thrombus) in addition to aspiration thrombectomy in 1 patient (Figure 1).
Discussion
The primary finding of the current analysis was that a large percentage of angiographically optimized stents demonstrated OCT abnormalities (90% of patients), requiring further intervention in approximately one-half of patients (52%). The most common reasons for further treatment after OCT were stent strut malapposition (77%), angiographically inapparent severe lesion (8%), in-stent thrombus (8%), and stent underexpansion (7%).
It is uncertain if further interventions based on OCT abnormalities found after angiographic optimization are useful in improving outcomes. One major study showed that minimizing strut malapposition, the most common OCT finding in this evaluation, improved long-term outcomes and decreased stent thrombosis,4 whereas some studies suggest it is not helpful.5 Identification of severe angiographic inapparent lesions post stenting, found in 8% of patients, either due to missed proximal or distal length of lesion, plaque shift, or ulcerated lesions may have clinical relevance but lack of prospective studies in this regard limits conclusions. In addition, more than one-half of patients (55%) with stent undersizing as the cause of stent strut malapposition required postdilation with proximal stent segment optimization. This finding was angiographically invisible. Stent undersizing has been shown by angiography to be a strong and independent predictor of stent thrombosis in registry data,6 although no prospective data in this regard are available. It also remains uncertain whether small edge dissections inapparent angiographically but seen on OCT heal spontaneously; thus, the value of covering them with an additional stent is uncertain.7,8 Therefore, the use of OCT to guide clinical decision making requires further study, particularly in a prospective and randomized fashion.
In our series, operators preferred to optimize stents with postdilation for stent strut malapposition. At this stage, the results reflect an individual operator’s practice patterns at a single institution, but do highlight the increasing recognition of stent strut malapposition after angiographically optimized stenting.
This study was undertaken as part of a quality improvement project to determine the adequacy of stent deployment in a single cardiac catheterization laboratory environment. Thus, the results of this analysis may not be generalizable. Furthermore, the analysis is limited by its retrospective nature and the uncertainty as to the reason for OCT evaluation in each case despite optimized stent angiographic appearance. Thus, the frequency of OCT abnormalities may be higher in this study than in day-to-day practice as operators chose to image the stented area despite an excellent angiographic appearance, suggesting a clinical suspicion by the operators.
During the study period, OCT evaluation of optimally deployed stents was undertaken in <10% of deployed stents, emphasizing the highly selected nature of the cohort. However, the data are clear that many OCT abnormalities are invisible angiographically and OCT may be a useful technique when there are concerns about the satisfactoriness of stent deployment. At this point, there are insufficient long-term data to recommend OCT more widely, but our data do suggest the possibility that OCT surveillance post stenting may improve results from stenting. Clearly, long-term studies are required to understand the place of OCT in optimizing stenting technique and long-term results.
Conclusion
In patients with optimized stent deployment by angiography, there was a relatively high frequency of abnormalities by OCT prompting further intervention. Stent strut malapposition was the most common reason for further intervention. OCT may be a useful technique in optimizing stent deployment and possibly improve outcomes.
References
1. Colombo A, Hall P, Nakamura S, et al. Intracoronary stenting without anticoagulation accomplished with intravascular ultrasound guidance. Circulation. 1995;91:1676-1688.
2. Cook JR, Mhatre AJ, Wang FW, Uretsky BF. Prolonged high-pressure is required for optimal stent deployment as assessed by optical coherence tomography. Catheter Cardiovasc Interv. 2014;83:521-527.
3. Tearney GJ, Regar E, Akasaka T, et al. Consensus standards for acquisition, measurement, and reporting of intravascular optical coherence tomography studies: a report from the International Working Group for Intravascular Optical Coherence Tomography Standardization and Validation. J Am Coll Cardiol. 2012;59:1058-1072.
4. Prati F, Di Vito L, Biondi-Zoccai G, et al. Angiography alone versus angiography plus optical coherence tomography to guide decision-making during percutaneous coronary intervention: the Centro per la Lotta contro l’Infarto-Optimisation of Percutaneous Coronary Intervention (CLI-OPCI) study. EuroIntervention. 2012;8:823-829.
5. Im E, Kim BK, Ko YG, et al. Incidences, predictors, and clinical outcomes of acute and late stent malapposition detected by optical coherence tomography after drug-eluting stent implantation. Circ Cardiovasc Interv. 2014;7:88-96.
6. van Werkum JW, Heestermans AA, Zomer AC, et al. Predictors of coronary stent thrombosis: the Dutch Stent Thrombosis Registry. J Am Coll Cardiol. 2009;53:1399-1409.
7. Radu MD, Räber L, Heo J, et al. Natural history of optical coherence tomography-detected non-flow-limiting edge dissections following drug-eluting stent implantation. EuroIntervention. 2014;9:1085-1094.
8. Bouki KP, Sakkali E, Toutouzas K, et al. Impact of coronary artery stent edge dissections on long-term clinical outcome in patients with acute coronary syndrome: an optical coherence tomography study. Catheter Cardiovasc Interv. 2015;86:237-246. Epub 2015 Feb 17.
_________________________________________________
From the Division of Cardiology, Central Arkansas Veterans Administration System, Little Rock, Arkansas.
Funding: This study was funded by a grant from St. Jude Medical.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. Dr Ahmed reports speaker’s bureau fees from Astra Zeneca. The remaining authors report no conflicts of interest regarding the content herein.
Manuscript submitted June 29, 2015, provisional acceptance given August 21, 2015, final version accepted November 6, 2015.
Address for correspondence: Barry F. Uretsky, MD, Central Arkansas Veterans Administration System, Division of Cardiology, 4300 West 7th Street, Little Rock, AR 72205. Email Address: buretsky@gmail.com










