


Use of Plaque Modification Microcatheters During Percutaneous Coronary Interventions for Chronic Total Occlusion: Insights From the PROGRESS‐CTO Registry
© 2024 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
Abstract
Plaque modification microcatheters (PM) (Tornus [Asahi] and Turnpike Gold [Teleflex]) are devices that are mainly used to modify the cap or lesion and maintain good support in chronic total occlusion (CTO) percutaneous coronary intervention (PCI). We evaluated the frequency of use and outcomes of plaque modification microcatheters in an international multicenter registry. Plaque modification microcatheters were utilized in 242 cases (1.6%: Tornus in 51% and Turnpike Gold in 49%) with decreasing frequency over time (P-for-trend: 0.007 and 0.035, respectively). Technical and procedural success and the incidence of major cardiac adverse events were similar with Tornus and Turnpike Gold use. PMs are infrequently utilized in CTO-PCI and are associated with high success and acceptable complication rates.
Introduction
Plaque modification microcatheters (PM) (Tornus [Asahi] and Turnpike Gold [Teleflex]) are sometimes used in chronic total occlusion (CTO) percutaneous coronary intervention (PCI).1,2 Tornus is a braided-wire mesh over-the-wire (OTW) microcatheter that is advanced with counterclockwise rotation and removed with clockwise rotation.3 On the contrary, Turnpike Gold is a gold-coated threaded tip OTW microcatheter that is advanced with clockwise rotation and removed with counterclockwise rotation.2
Methods
We evaluated the frequency of use and outcomes of PMs in 15 070 lesions in 14 767 patients who underwent CTO-PCI at 43 centers between 2012 and 2023 as part of the Prospective Global Registry for the Study of CTO Intervention (PROGRESS-CTO; Clinicaltrials.gov identifier: NCT02061436). The study was approved by the institutional review board of each center. Technical success was defined as restoration of Thrombolysis in Myocardial Infarction (TIMI) 3 antegrade flow through the CTO with < 30% residual diameter stenosis. In-hospital major adverse cardiac events (MACE) were defined as any of the following adverse events before discharge: death, myocardial infarction, repeat target vessel revascularization with PCI or coronary artery bypass surgery (CABG), coronary perforation, tamponade, pericardiocentesis, or stroke. Time-trend analysis was assessed using the Mann-Kendall test for monotonic trend. All statistical analyses were performed using R Statistical Software, version 4.2.2 (R Foundation for Statistical Computing).
Results
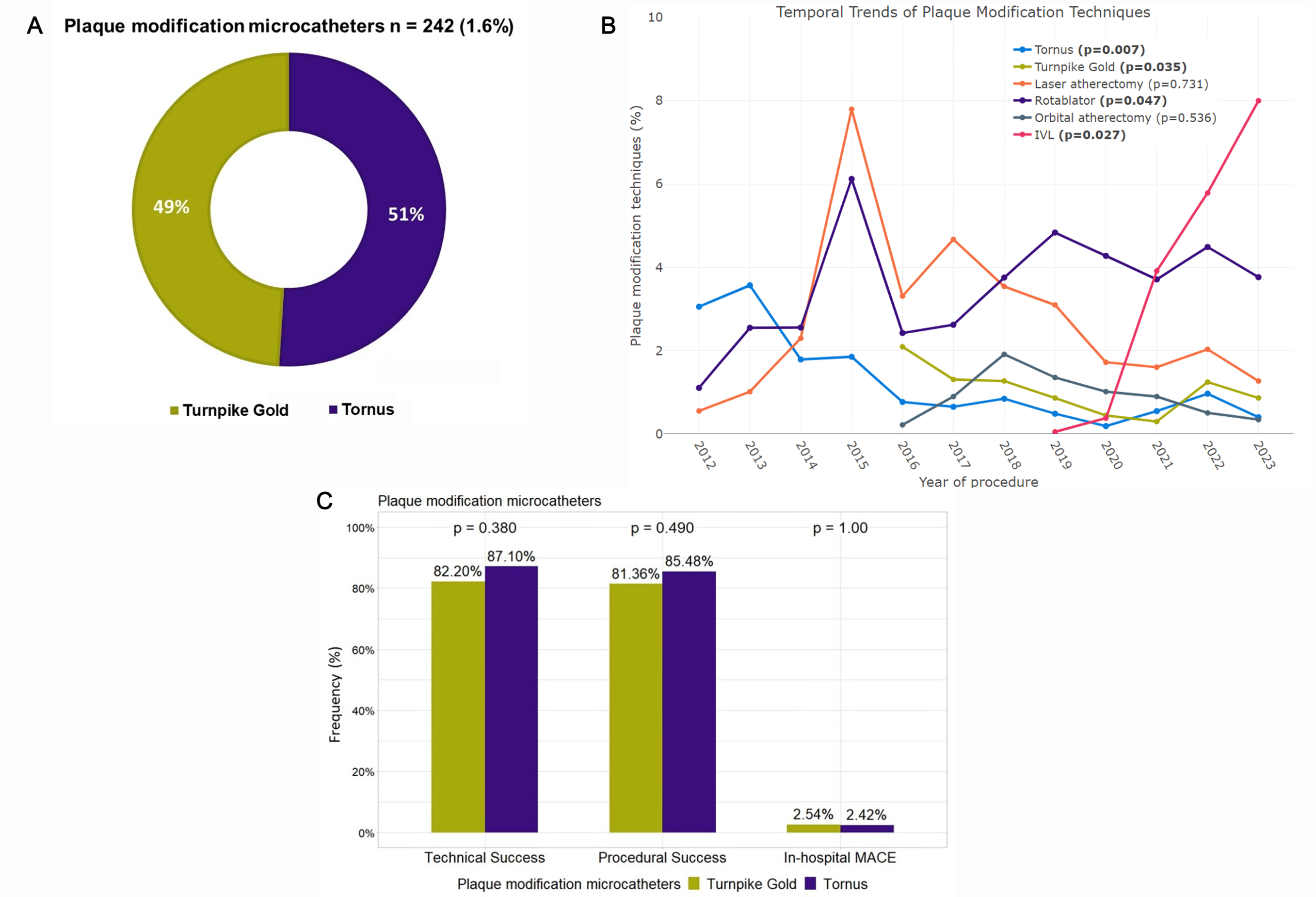
PMs were utilized in 242 (1.6%) cases (Tornus 51% and Turnpike Gold 49%) with decreasing frequency over time (Figure A and B). Mean patient age was 65 ± 9.6, 84% were men, and 32.5% had prior CABG. CTOs requiring use of PMs were more complex with a higher J-CTO (Multicenter CTO Registry in Japan) score (2.65 ± 1.14 vs. 2.38 ± 1.27, P = .001), and higher prevalence of moderate to severe calcification (77% vs. 45.5%, P < .001). They were more frequently located in the right coronary artery (60.1%) and the left circumflex artery (21.1%). The most common CTO-crossing technique was antegrade wiring (90.5%), followed by retrograde true-to-true wiring (6.2%). PMs were most commonly used to treat balloon-uncrossable (72.0%) and balloon-undilatable (26.0%) lesions.
Tornus (87.3%) was more frequently used than Turnpike Gold (58.0%) in balloon-uncrossable CTOs (P < .001). Technical (87.1% vs. 82.2%, P = .380) and procedural (85.5% vs. 81.3%, P = .490) success and the incidence of MACE (2.4% vs. 2.5%, P = 1.00) were similar with Tornus and Turnpike Gold (Figure C). Procedure time was also similar in both groups (134 [93-185] vs 119 [89-196] minutes, P = .538).
Over time, the overall use of plaque modification techniques such as rotational atherectomy (from 1.1% in 2012 to 3.8% in 2023, P for trend = 0.047) and intravascular lithotripsy (from 0.05% in 2019 to 8% in 2023, P for trend = 0.027) significantly increased, whereas the use of PMs decreased (from 3.1% in 2012 to 1.2% in 2023, P for trend = 0.047). (Figure B).
Discussion
Fang et al reported successful use of Tornus in highly calcified CTOs with a short proximal stump.4 Overall technical success was 71.4% in 56 balloon- or microcatheter-uncrossable CTOs.4 In a study by Mohandes et al, Tornus successfully crossed 78.6% in 14 balloon-uncrossable CTOs.5 Martin-Yuste et al reported a technical success of 88% in 17 patients with balloon-undilatable CTOs.6 Jackson et al reported a technical success rate of 67% for Turnpike Gold in 21 balloon- and microcatheter-uncrossable lesions (5 were CTOs).7 We did not find any difference in success and complications between the Tornus and Turnpike Gold groups. However, as the Tornus lacks an inner lining, it is not feasible to inject contrast through it, whereas injection of contrast or other liquids is feasible through the Turnpike Gold.
The use of plaque modification microcatheters declined between 2012 and 2023. This decline can be attributed to advancements in contemporary plaque modification techniques, including the adoption of low-profile balloons, rotational/orbital or laser atherectomy, intravascular lithotripsy, and development of innovative plaque modification techniques, such as move-the-cap techniques (balloon-assisted subintimal entry, scratch-and-go) and the Carlino technique.1,8
Limitations. PROGRESS-CTO is an observational registry without core laboratory assessment of angiograms and event adjudication of the complications. All procedures were performed by experienced and dedicated CTO-PCI operators, and the decision to use PMs was at the operator's discretion.
Conclusions
In summary, PMs are infrequently utilized in CTO-PCI and are associated with high success and acceptable complication rates.
Affiliations and Disclosures
From the 1Minneapolis Heart Institute and Minneapolis Heart Institute Foundation, Abbott Northwestern Hospital, Minneapolis, Minnesota, USA; 2Massachusetts General Hospital, Boston, MA, USA; 3Henry Ford Cardiovascular Division, Detroit, MI, USA; 4Cleveland Clinic, Cleveland, OH, USA; 5Meshalkin National Research Institute, Novosibirsk, Russian Federation; 6Biruni University Medical School, Istanbul, Turkey; 7Memorial Bahcelievler Hospital, Istanbul, Turkey; 8Texas Health Presbyterian Dallas Hospital and Baylor Scott & White Heart and Vascular Hospital, Dallas, TX, USA; 9Oklahoma Heart Institute, Tulsa, OK, USA; 10The Heart Hospital Baylor Plano, Plano, TX, USA; 11University Hospitals, Case Western Reserve University, Cleveland, OH, USA; 12Central Arkansas Veterans Health System, and University of Arkansas for Medical Sciences, Little Rock, AR, USA; 13Piedmont Heart Institute, Atlanta, GA, USA; 14Goztepe Medical Park Hospital, Istanbul, Turkey; 15University of Washington, Seattle, WA, USA.
Acknowledgments: The authors are grateful for the philanthropic support of our generous anonymous donors (2), and the philanthropic support of Drs. Mary Ann and Donald A Sens; Mr. Raymond Ames and Ms. Barbara Thorndike; Frank J and Eleanor A. Maslowski Charitable Trust; Joseph F and Mary M Fleischhacker Family Foundation; Mrs. Diane and Dr. Cline Hickok; Mrs. Marilyn and Mr. William Ryerse; Mr. Greg and Mrs. Rhoda Olsen; Mrs. Wilma and Mr. Dale Johnson; Mrs. Charlotte and Mr. Jerry Golinvaux Family Fund; the Roehl Family Foundation; the Joseph Durda Foundation. The generous gifts of these donors to the Minneapolis Heart Institute Foundation’s Science Center for Coronary Artery Disease (CCAD) helped support this research project.
Disclosures: Dr. Jaffer receives consulting/speaker honoraria from Canon, Biotronik, Teleflex, Boston Scientific, Heartflow, Siemens, and Mercator; and is a shareholder in Fastwave, DurVena, and Intravascular Imaging Inc. Dr. Alaswad receives consulting/speaker honoraria from Boston Scientific, Abbott Vascular, Teleflex, and CSI. Dr. Khatri receives personal honoraria for proctoring and speaking from Abbott Vascular, Medtronic, Terumo, Shockwave, and Boston Scientific. Dr. Basir receives consulting/speaker honoraria from Abiomed, Boston Scientific, Chiesi, Saranas, and Zoll. Dr. Choi serves on the advisory board member of Medtronic. Dr. Potluri receives consulting/speaker honoraria from Edwards Lifesciences, Boston Scientific, Philips, and Shockwave. Dr. Poommipanit receives consulting/speaker honoraria from Abbott Diagnostics and Asahi. Dr. Kandzari receives consulting/speaker honoraria from Biotronik, Boston Scientific, Medtronic, and Cardinal Health. Dr. Azzalini receives consulting/speaker honoraria from Abbott, Teleflex, GE Healthcare, Reflow Medical, Cardiovascular Systems Inc, and Abiomed; and serves on the advisory board for Abiomed and GE Healthcare. Dr. Sandoval receives consulting/speaker honoraria from Abbott Diagnostics, Roche Diagnostics, Zoll, and Philips; is an associate editor of JACC Advances; and holds patent 20210401347. Dr. Burke receives consulting honoraria, and has received speaker honoraria, from Abbott Vascular and Boston Scientific. Dr Brilakis receives consulting/speaker honoraria from Abbott Vascular, the American Heart Association (associate editor, Circulation), Amgen, Asahi Intecc, Biotronik, Boston Scientific, Cardiovascular Innovations Foundation (Board of Directors), CSI, Elsevier, GE Healthcare, IMDS, Medicure, Medtronic, Siemens, and Teleflex; receives research support from Boston Scientific and GE Healthcare; is the owner Hippocrates LLC; and is a shareholder in MHI Ventures, Cleerly Health, and Stallion Medical.
Address for correspondence: Emmanouil S. Brilakis, MD, PhD, Minneapolis Heart Institute, 920 E 28th Street #300, Minneapolis, MN 55407, USA. Email: esbrilakis@gmail.com. ; X: @dnzmtlu, @RempakosT, @m1chaella_alex, @AhmedAlOgaili, @LAzzaliniMD, @yadersandoval, @esbrilakis
References
1. Mashayekhi AK, Pyxaras AS, Werner SG, et al. Contemporary issues of percutaneous coronary intervention in heavily calcified chronic total occlusions: an expert review from the European CTO Club. EuroIntervention. 2023;19(2):e113-e122. doi: 10.4244/EIJ-D-22-01096
2. Vemmou E, Nikolakopoulos I, Xenogiannis I, et al. Recent advances in microcatheter technology for the treatment of chronic total occlusions. Expert Rev Med Devices. 2019;16(4):267-273. doi: 10.1080/17434440.2019.1602039
3. Brilakis ES, Grantham JA, Rinfret S, et al. A percutaneous treatment algorithm for crossing coronary chronic total occlusions. JACC Cardiovasc Interv. 2012;5(4):367-379. doi: 10.1016/j.jcin.2012.02.006
4. Fang HY, Lee CH, Fang CY, et al. Application of penetration device (Tornus) for percutaneous coronary intervention in balloon uncrossable chronic total occlusion-procedure outcomes, complications, and predictors of device success. Catheter Cardiovasc Interv. 2011;78(3):356-362. doi: 10.1002/ccd.22862
5. Mohandes M, Rojas S, Guarinos J, et al. Efficacy and safety of Tornus catheter in percutaneous coronary intervention of hard or balloon-uncrossable chronic total occlusion. ARYA Atheroscler. 2016;12(4):206-211.
6. Martin-Yuste V, Alvarez-Contreras L, Cola C, et al. [Usefulness of the Tornus(R) catheter in nondilatable coronary chronic total occlusion]. Rev Esp Cardiol. 2011;64(10):935-938. doi: 10.1016/j.recesp.2011.01.011
7. Jackson M, Egred M. Usefulness of the Turnpike Gold Catheter in Balloon Uncrossable Coronary Lesions. J Clinical Cardiology and Cardiovascular Interventions. 2020;3(5):1-7.
8. McQuillan C, Jackson MWP, Brilakis ES, Egred M. Uncrossable and undilatable lesions-A practical approach to optimizing outcomes in PCI. Catheter Cardiovasc Interv. 2021;97(1):121-126. doi: 10.31579/2641-0419/064











