

Intra-Caval Balloon Pump
Keywords: balloon pump, intra-caval balloon pump
A 55-year-old female with a history of cardiac transplant-related coronary artery vasculopathy, disseminated fungal lung infection, and chronic respiratory failure presented with dyspnea and an increased oxygen requirement. Notable were a high sensitivity troponin I of 10,647 ng/L (reference range <52), and a left ventricular ejection fraction of 52% with a new wall-motion abnormality (previous ejection fraction and wall motion were normal).
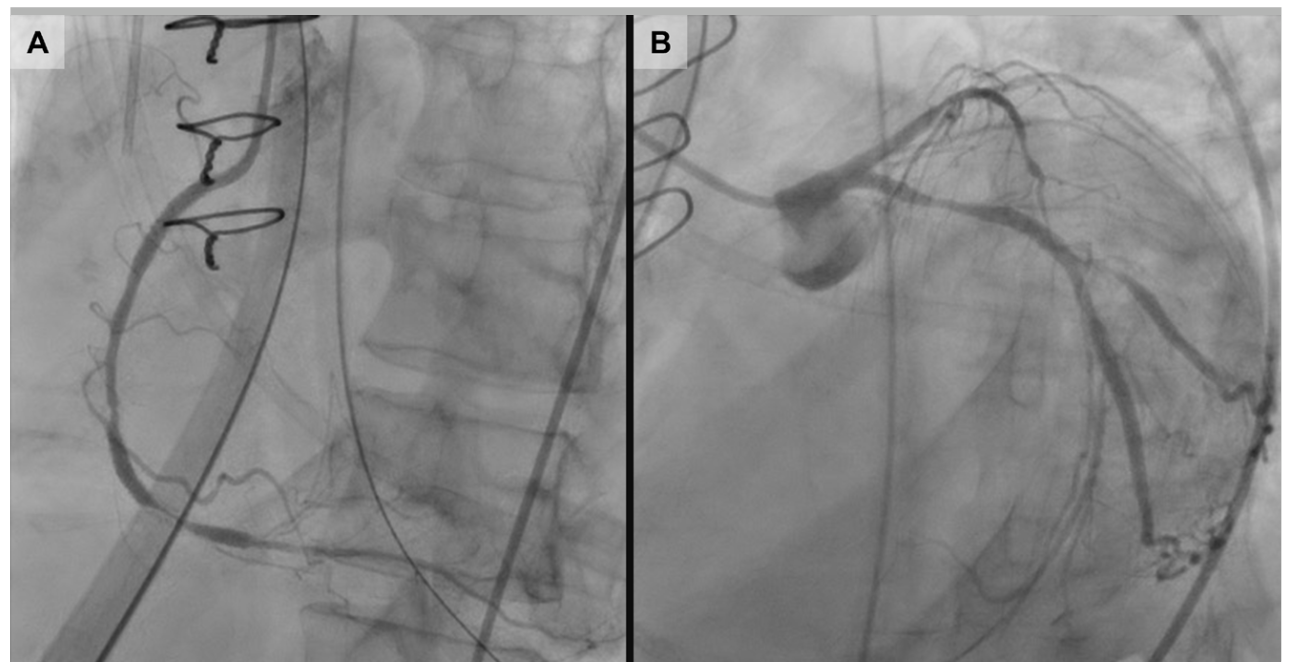
Coronary angiography performed after respiratory stabilization revealed a left-sided aortic arch and diffuse disease without a clear infarct-related artery (Figure 1). Percutaneous coronary intervention was deferred and medical therapy with dual-antiplatelet therapy and intravenous heparin was continued. Intravenous diuretic therapy was also started as the left ventricular end-diastolic pressure was 20 mm Hg.
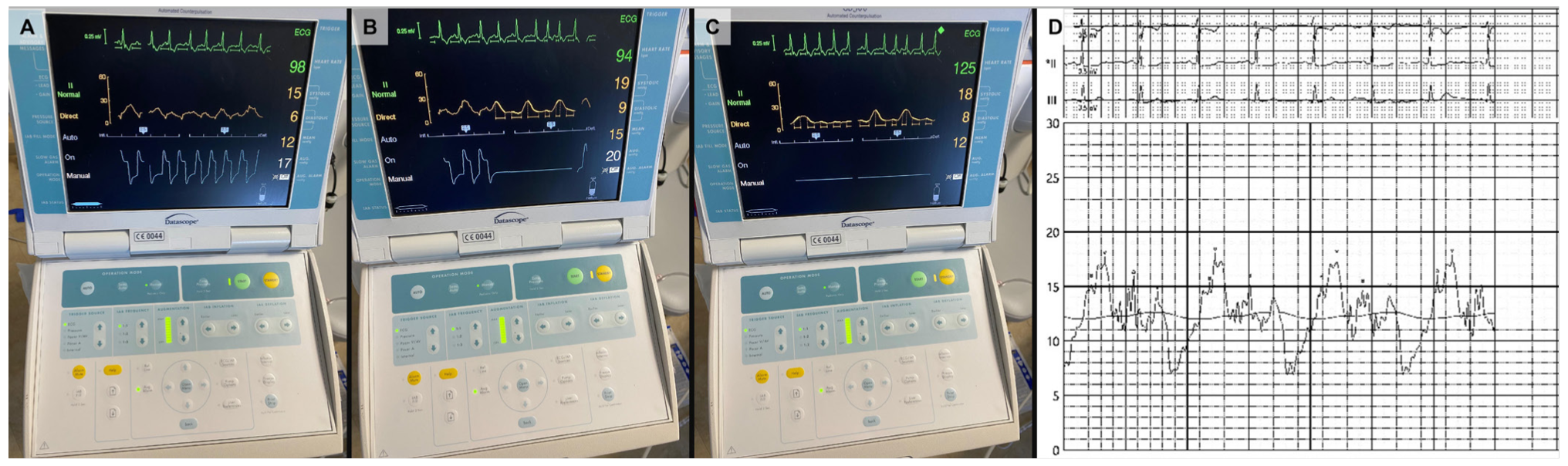
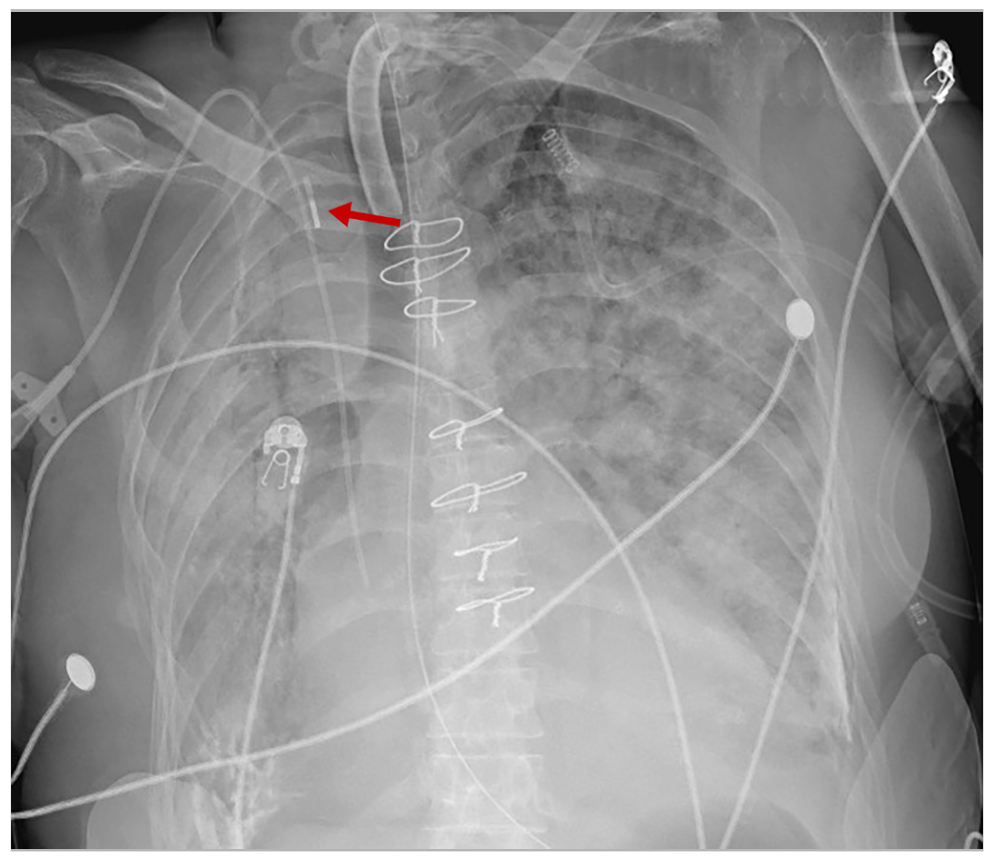
Cardiac arrest occurred 48 hours later, and a Lund University Cardiopulmonary Assist System was used to provide mechanical chest compressions, while emergent right femoral intra-aortic balloon pump (IABP) was placed at the bedside after confirmation of pulsatile blood return. Inflations at 1:1 were initiated and resuscitation efforts continued. The balloon pump waveform appeared abnormal with low mean and augmentation pressures (Figure 2), but this was attributed to ongoing hypotension or a technical problem related to the pump rather than position, because pulsatile blood return was noted at the time of right femoral access. It was not until a chest x-ray was performed that intra-caval placement of the balloon pump was identified and subsequently replaced in the femoral artery.
The hemodynamic benefits of IABP during experimental cardiac arrest include shorter circulation time, increases in end-tidal CO2, and coronary perfusion pressure. However, the hemodynamic effect of venous diastolic augmentation during experimental cardiogenic shock varies from detrimental in cases of low preload, to possibly beneficial in a high preload state.
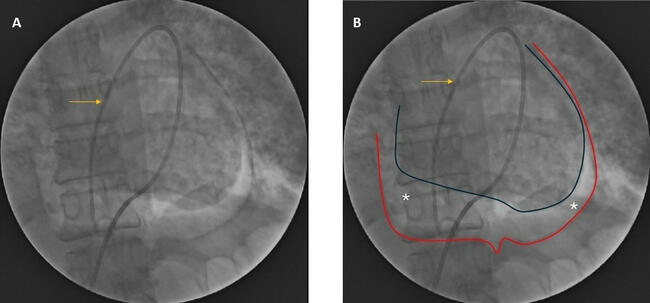
When performed emergently at the bedside, inadvertent intra-caval placement of a balloon pump can occur due to elevated venous pressures such as during cardiopulmonary resuscitation, in the presence of severe tricuspid regurgitation, or through an arteriovenous fistula. A similar radiographic appearance can also be seen in the presence of a right–sided aortic arch (Figure 3). Clues to improper position include an abnormal pressure waveform and the absence of hemodynamic changes or blood pressure augmentation.
Affiliations and Disclosures
From the 1Division of Cardiology, 2Department of Internal Medicine, University of Texas Southwestern Medical Center, Dallas, Texas.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
The authors report that patient consent was provided for publication of the images used herein.
Manuscript accepted May 9, 2022.
Address for correspondence: Faris G. Araj, MD, Associate Professor of Medicine, University of Texas Southwestern Medical Center, Professional Office Bldg 2, Suite 600, 5939 Harry Hines Blvd, Dallas, TX 75390-9252. Email: faris.araj@utsouthwestern.edu













{kind=link}
{kind=link}
{kind=link}