

King Ghidorah Technique for a Trifurcation Lesion in a Very High-Risk NSTEMI
© 2024 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
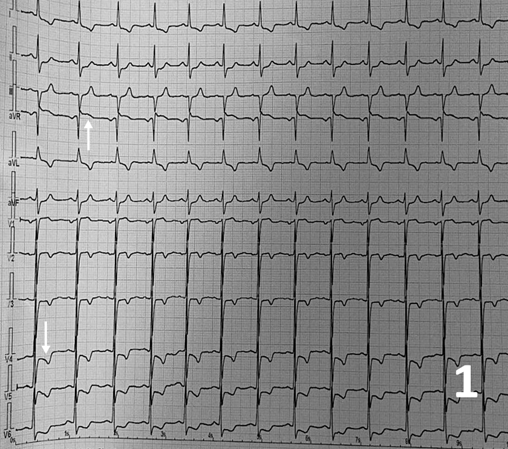
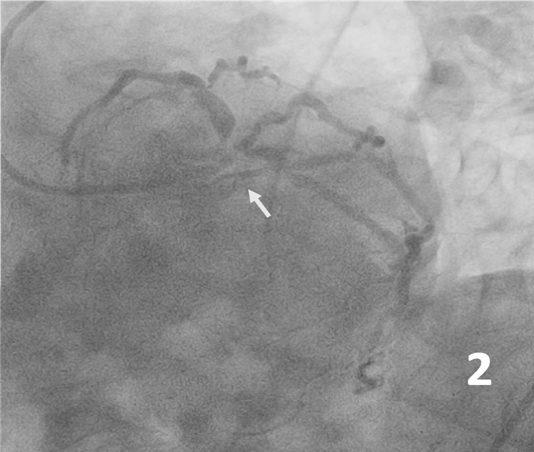
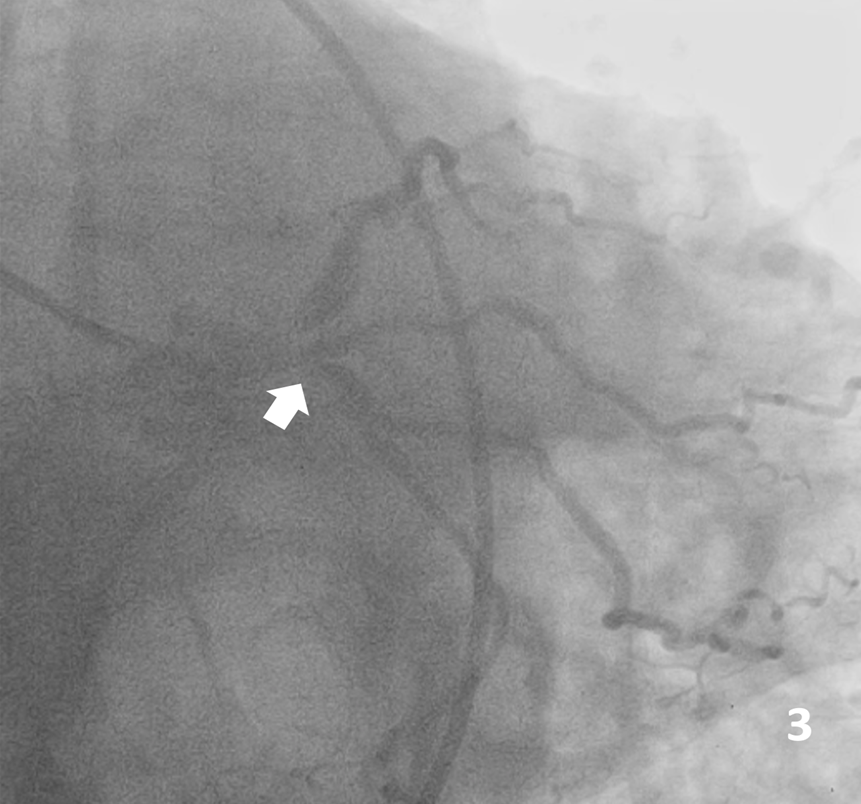
A 66-year-old male Jehovah’s Witness arrived at the emergency room having experienced typical persistent angina. Upon arrival, he was hemodynamically unstable. Electrocardiogram showed a high-risk pattern (Figure 1) and hs-cTn of 21 000 ng/L. Coronary angiography showed critical left distal main disease with trifurcation lesion to the left anterior descending artery (LAD), ramus intermedius, and left circumflex artery (LCx) (medina 1-1-1-1), and an 80% lesion in the middle segment of the LAD (Figure 2, 3). After medical consensus with surgeons, we decided to proceed with percutaneous coronary intervention.
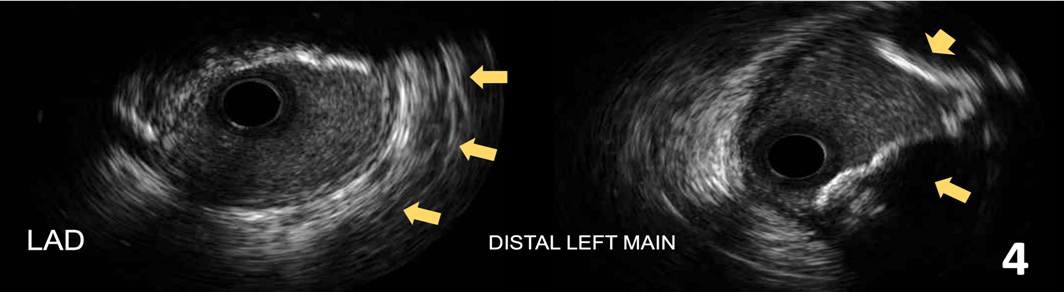
An 8-French VODA (Boston Scientific) catheter was used through femoral route and 3 Runthrough NS Hypercoat 0.014-inch guidewires (Terumo) were advanced to the LAD, ramus, and the LCx. Intravascular ultrasound (IVUS) OptiCross (Boston Scientific) was performed from the mid-segment LAD to the left main artery; the LAD had severe calcification in the mid-to-proximal segment with a minimum luminal area (MLA) of 3.4 mm2, and the left main artery had severe calcification and an MLA of 3 mm2. (Figure 4).
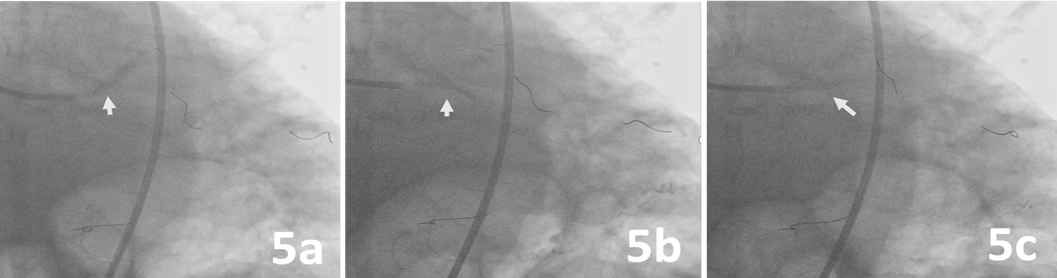
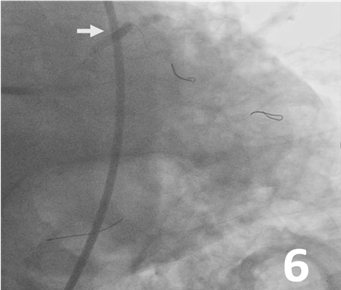
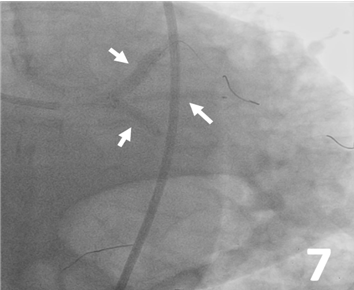
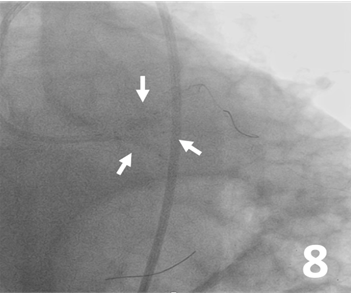
Predilatation was made from the LAD, ramus, and LCx to the left main artery with 3 Ryurei balloons (Terumo) at 8 atm (3.5 x 20 mm, 2.5 x 20 mm, and 2.5 x 15 mm, respectively) (Figure 5). A 3.0 x 32-mm synergy stent was deployed from the middle to the proximal segment of the LAD (Figure 6). Then, 3 stents were advanced and deployed simultaneously from the LAD, ramus, and LCx (Synergy 5.0 x 24 mm [Boston Scientific], Xience Sierra 3.0 x 33 mm [Abbott], and Synergy 3.5 x 16 mm, respectively) (Figure 7). Simultaneous triple-balloon (kissing) inflation at 12 atm was performed with three 2.0 x 15-mm Ryurei balloons (Figure 8); the 3 balloons were simultaneously inflated 3 times.
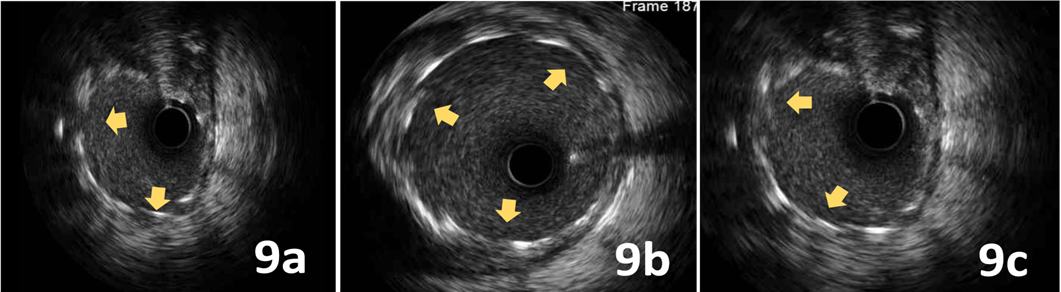
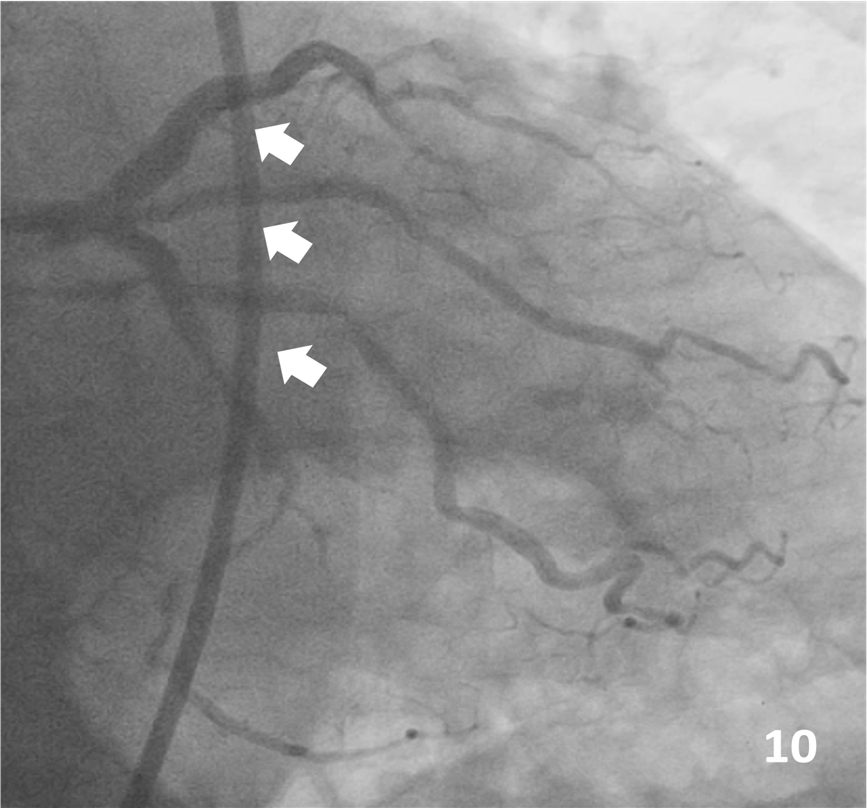
Final IVUS showed adequate expansion and no edge dissections (Figure 9). The final angiographic result is shown in Figure 10. There were no complications at all during the procedure, and the patient was discharged 3 days later.
Affiliations and Disclosures
From the Department of Interventional Cardiology, Centro Médico Nacional 20 de Noviembre, ISSSTE, Ciudad de México, México.
Disclosures: The authors report no financial relationships or conflicts of interest regarding the content herein.
Address for correspondence: Kevin Hernández-Flores, MD, Department of Interventional Cardiology, Av. Félix Cuevas #540, Col. Del Valle Del. Benito Juárez, C.P. 03100, México. Email: kevinrene9191@gmail.com










