

Rare Case of Myocardial “Milking” in a Diagonal Branch Artery
© 2024 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
Myocardial bridging is a very common anomaly that can be found in more than 30% of the population based on autopsy studies.1 Systolic compression during coronary filling can result in hemodynamic changes that may be associated with angina, myocardial ischemia, acute coronary syndrome, left ventricular (LV) dysfunction, arrhythmias, and sudden cardiac death.2 One study found that the relative frequency of myocardial bridging exclusively involving the left anterior descending artery (LAD) was 70%, involving the left circumflex artery was 40%, and involving the right coronary artery was 36%.3 However, there are little data on myocardial bridging in branch vessels.
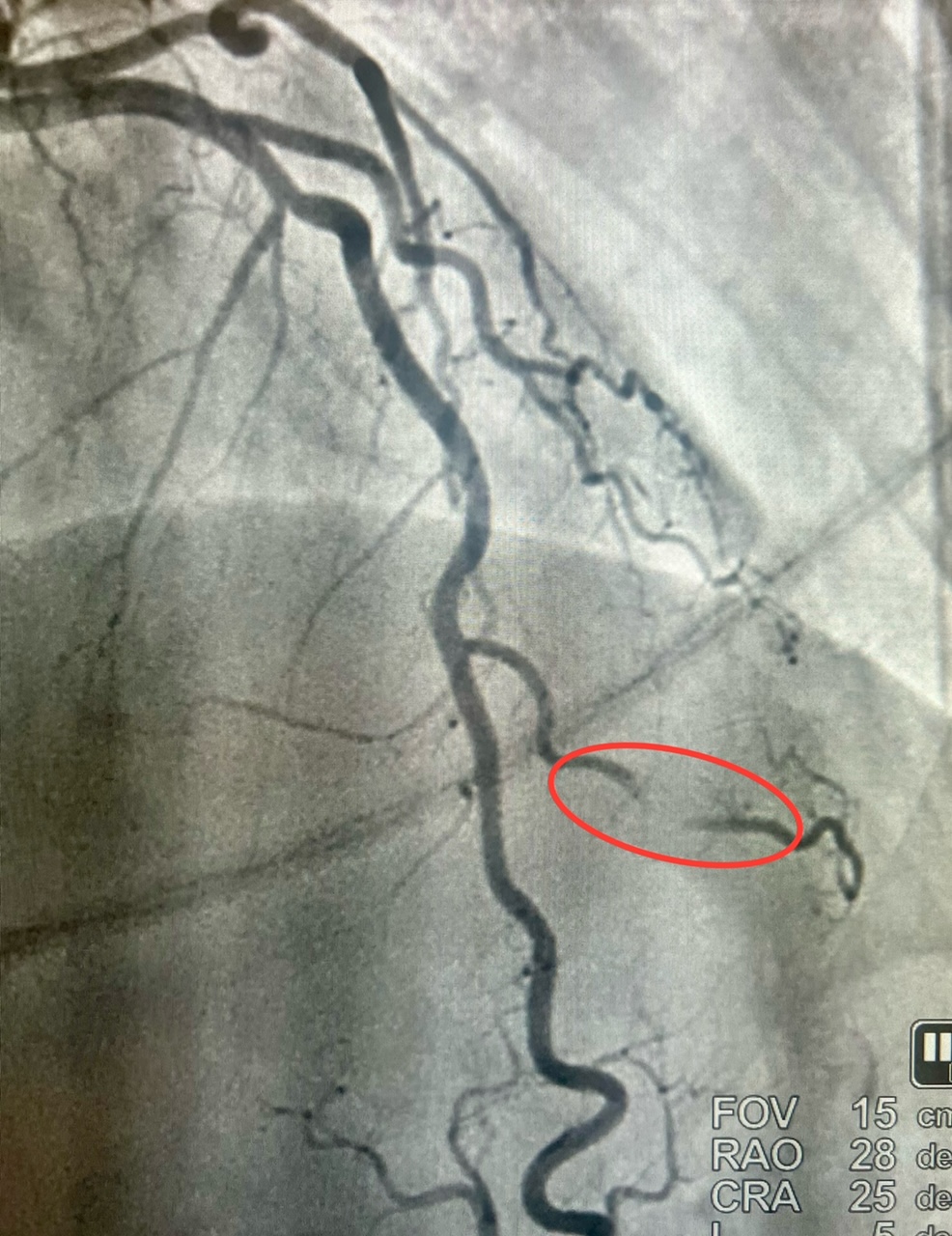
We present a 54-year-old woman with a medical history of opioid addiction, anxiety disorder, and current cigarette smoker who presented to the hospital via Emergency Medical Service after an episode of syncope at home. (Figures 1 and 2). The patient continued to have recurrent episodes of ventricular tachycardia along with elevated troponins, with an echocardiogram that showed reduced LV ejection fraction with slightly more pronounced hypokinesis of the septal and apical walls; thus, the decision was made to rule out ischemia as a possible cause. She subsequently underwent coronary angiography via the right radial approach, which revealed a right-dominant system, and normal coronary arteries, with the exception of the second diagonal branch of the LAD, which had severe systolic compression, resulting in obliteration of the artery with each cardiac cycle. Angiographically, when a vessel completely obliterates during cardiac catheterization, it is referred to as a “milking” phenomenon (Video).
The patient was referred for implantable cardioverter defibrillator placement for cardiomyopathy. Medical therapy was recommended for the myocardial bridging, the initial treatment of which primarily includes beta blockers, which are thought to relieve hemodynamic disturbances by decreasing peak heart rate, increasing diastolic filling time, and decreasing contractility and compression of the artery.4 The patient will routinely follow up with their cardiologist for observation.

Affiliations and Disclosures
Richard Casazza, MAS; David J. Epstein, MD; Nicole DeLeon, MD; Enrico Montagna, RT (CI); Isa Sarro; Arsalan Hashmi, MD
From the Maimonides Medical Center, Brooklyn, New York, USA.
Disclosures: The authors report no relevant financial relationships or conflicts of interest regarding the content herein.
Consent statement: Informed consent from the patient was received.
Address for correspondence: Richard Casazza, MAS, RT (R) (CI), Department of Cardiology, Maimonides Medical Center, 4802 10th Avenue, Brooklyn, NY 11219, USA. Email: rcasazza@maimonidesmed.org; X: @tesslagra
References
- Hostiuc S, Negoi I, Rusu MC, Hostiuc M. Myocardial bridging: a meta-analysis of prevalence. J Forensic Sci. 2018;63(4):1176-1185. doi:10.1111/1556-4029.13665
- Lee MS, Chen CH. Myocardial bridging: an up-to-date review. J Invasive Cardiol. 2015;27(11):521-528.
- Polacek P, Kralove H. Relation of myocardial bridges and loops on the coronary arteries to coronary occulsions. Am Heart J. 1961;61:44-52. doi:10.1016/0002-8703(61)90515-4
- Schwarz ER, Klues HG, vom Dahl J, Klein I, Krebs W, Hanrath P. Functional, angiographic and intracoronary Doppler flow characteristics in symptomatic patients with myocardial bridging: effect of short-term intravenous beta-blocker medication. J Am Coll Cardiol. 1996; 27(7):1637-1645. doi:10.1016/0735-1097(96)00062-9










