

Antiplatelet Therapy in Acute Myocardial Infarction and Cardiogenic Shock: Insights From the National Cardiogenic Shock Initiative
Abstract
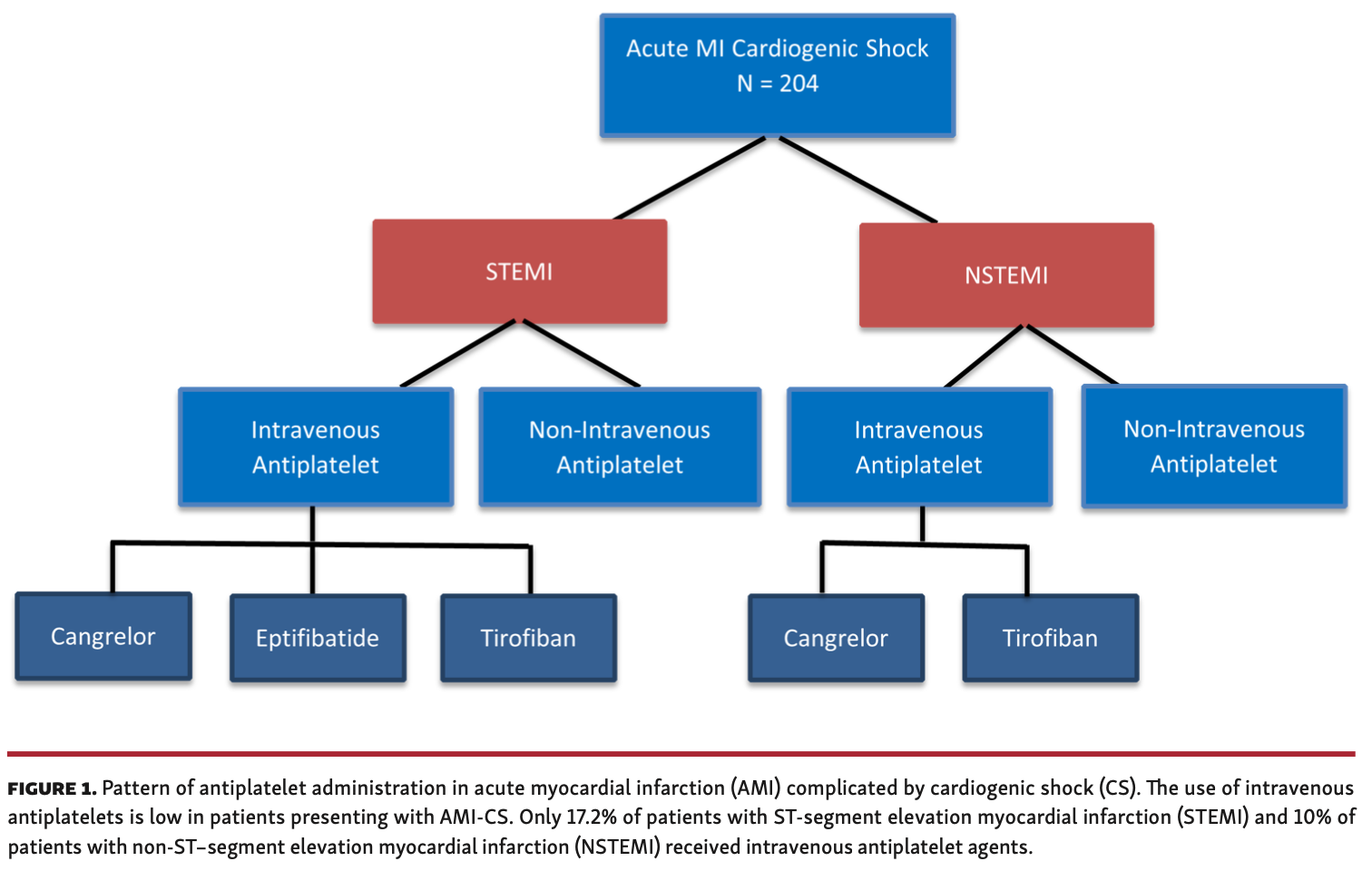
Background. Patients presenting with acute myocardial infarction complicated by cardiogenic shock (AMI-CS) are at high risk for impaired antiplatelet activity secondary to malabsorption, systemic hypoperfusion, hypothermia, need for mechanical ventilation, and high use of analgesics. The use of antiplatelet therapy in these high-risk patients is not well studied. Methods. Using the National Cardiogenic Shock Initiative database, we analyzed patients who presented with AMI-CS at 60 hospitals from March 2018 to December 2020. All patients were treated using a standard shock protocol. Herein, the patterns of antiplatelet use are described. Results. A total of 204 patients were included in the analysis, of which 174 (85.3%) presented with ST-segment elevation myocardial infarction (STEMI). The majority (84.3%) received antiplatelet therapy before percutaneous coronary intervention (PCI); of those who received antiplatelets, 77.9% received aspirin, 55.2% received an oral P2Y12 inhibitor, and 19.2% received intravenous (IV) antiplatelet therapy. Ticagrelor was the most common P2Y12 inhibitor administered (41.9%), followed by clopidogrel (12.2%) and prasugrel (1.2%). Only 18.6% of oral antiplatelet agents were crushed. Baseline characteristics of patients who received IV vs non-IV antiplatelet agents were similar. Thrombolysis in Myocardial Infarction (TIMI) 0 flow was present in 69.6% of patients before PCI and aspiration thrombectomy was performed in 24.5% of patients. The presence of STEMI, cardiac arrest, cardiopulmonary resuscitation, hypothermia, vasopressor use, elevated lactate levels, or number of vessels treated did not influence the use of IV antiplatelet agents. Conclusions. The use of crushed and IV antiplatelet agents in AMI-CS is low. Further studies are needed in this high-risk population to assess whether more potent antiplatelet inhibition will improve outcomes.
J INVASIVE CARDIOL 2022;34(3):E156-E163. Epub 2022 February 11.
Key words: antiplatelets, cardiogenic shock, glycoprotein IIb/IIIa inhibitors, P2Y12 inhibitors
Introduction
The use of antiplatelet therapies and ability to achieve adequate platelet inhibition at the time of percutaneous coronary intervention (PCI) in acute myocardial infarction (AMI) complicated by cardiogenic shock (CS) is not well studied. Dual-antiplatelet therapy (DAPT) following early revascularization aims to prevent periprocedural thrombotic events and reduce major adverse cardiovascular events. The hemodynamic consequences of CS impact the activity of oral antiplatelet medications. Decreased organ perfusion, impaired absorption, hypothermia, administration of analgesics, and delayed metabolism all affect the ability to achieve adequate platelet inhibition using oral antiplatelet agents. The ideal combination of antiplatelet therapy continues to be debated. Current United States and European guidelines recommend that aspirin plus a P2Y12 inhibitor be given to patients with AMI undergoing PCI.1,2 The guidelines further provide a class IIA recommendation that ticagrelor be the preferred P2Y12 inhibitor and that the first dose be crushed or chewed for improved absorption. Due to continued concern over the bioavailability of oral agents, clinicians may use intravenous (IV) P2Y12 or glycoprotein (GP) IIb/IIIa inhibitors. The National Cardiogenic Shock Initiative (NCSI) collected data on the utilization of antiplatelet agents administered in patients presenting with AMI-CS using a shock protocol. Herein, we describe the current use of antiplatelet therapy in AMI-CS within the NCSI.
Methods
The NCSI (ClinicalTrials.gov: NCT03677180) was a single-arm, prospective study evaluating the use of a shock protocol emphasizing early treatment of AMI-CS using mechanical circulatory support (MCS) with Impella (Abiomed), PCI, and pulmonary artery catheter-guided therapy. Eligible patients were those with AMI-CS treated with early revascularization with PCI and supported by MCS. AMI was defined as electrocardiographic changes indicative of presumed new ischemia (ST-T changes), detection of elevated cardiac biomarkers, or angiographic findings of an infarct-related artery on coronary angiogram in the presence of ischemic symptoms. CS must have been present prior to PCI and was defined as the presence of at least 2 of the following: (1) prolonged hypotension (systolic blood pressure <90 mm Hg or use of vasopressors to maintain systolic blood pressure >90 mm Hg); (2) signs of end-organ hypoperfusion (cool extremities, oliguria or anuria, or elevated lactate levels); or (3) hemodynamic criteria represented by cardiac index <2.2 L/min/m2 or cardiac power output <0.6 watts. Operators were highly encouraged to follow the treatment algorithm and place MCS prior to PCI and use a pulmonary artery catheter to guide subsequent therapy. However, patients treated outside of these best practices were still included if they met all other inclusion and exclusion criteria listed below. The antiplatelet regimen used during the PCI was left to the discretion of the primary treatment team.
Between March 2018 and December 2020, a total of 60 sites participated and enrolled in the study, using a case report form that included antiplatelet data. Institutional review board approval was obtained at each of the participating sites. Consent was obtained from patients or patient surrogates if they survived. For patients who did not survive and would not require follow up, de-identified data were captured in accordance with local institutional review board requirements. Participating centers agreed to treat the majority of patients with AMI-CS using a mutually agreed-upon shock algorithm based on best practices. Exclusion criteria included the following: patients with evidence of anoxic brain injury on presentation; any unwitnessed out-of-hospital cardiac arrest; any cardiac arrest in which return of spontaneous circulation was not achieved within 30 minutes; intra-aortic balloon pump placed prior to Impella; septic, anaphylactic, hemorrhagic, and neurologic causes of shock; non-ischemic causes of shock/hypotension (including pulmonary embolism, pneumothorax, myocarditis, tamponade, etc); active bleeding for which MCS was contraindicated; recent major surgery for which MCS was contraindicated; mechanical complications of AMI (acute ventricular septal defect or acute papillary muscle rupture); known left ventricular thrombus for which MCS was contraindicated; mechanical aortic prosthetic valve; or contraindication to IV systemic anticoagulation. AMI-CS comprised a heterogeneous cohort of patients, and inclusion and exclusion criteria were included to limit those who presented in pre-shock and those with refractory shock associated with prolonged cardiac arrest. A total of 204 patients met all inclusion and no exclusion criteria to be included in this study. All patients had antiplatelet information available for review.
Statistical analysis. Continuous variables were described using mean ± standard deviation, while categorical variables were described with frequency and percentage. Student’s t-test was used for continuous variables and Chi‐square test or Fisher’s exact tests were used for categorical variables, as appropriate. A P-value <.05 was considered significant for all statistical tests.
Results
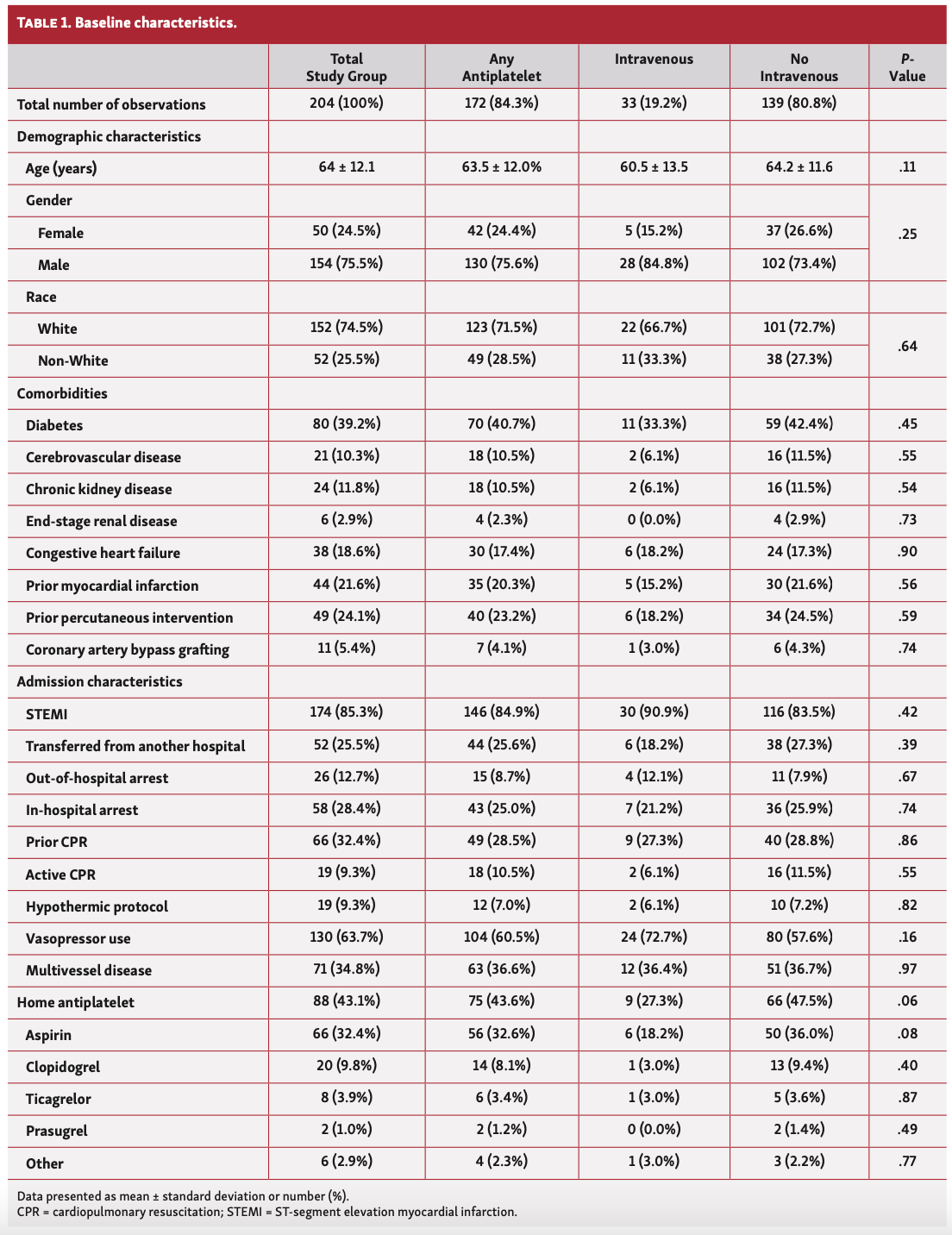
There were 204 patients included in this analysis. The mean age was 64 ± 12.1 years, 75.5% were men, and 85.3% presented with ST-segment elevation myocardial infarction (STEMI). Out of the 204 patients, 12.7% had out-of-hospital arrest, 28.4% had in-hospital arrest, and 9.3% underwent therapeutic hypothermia. The majority of patients (86.3%) required ≥1 vasopressors, 64.2% of patients had single-vessel PCI and 34.8% had multivessel PCI. Baseline demographics are outlined in Table 1.
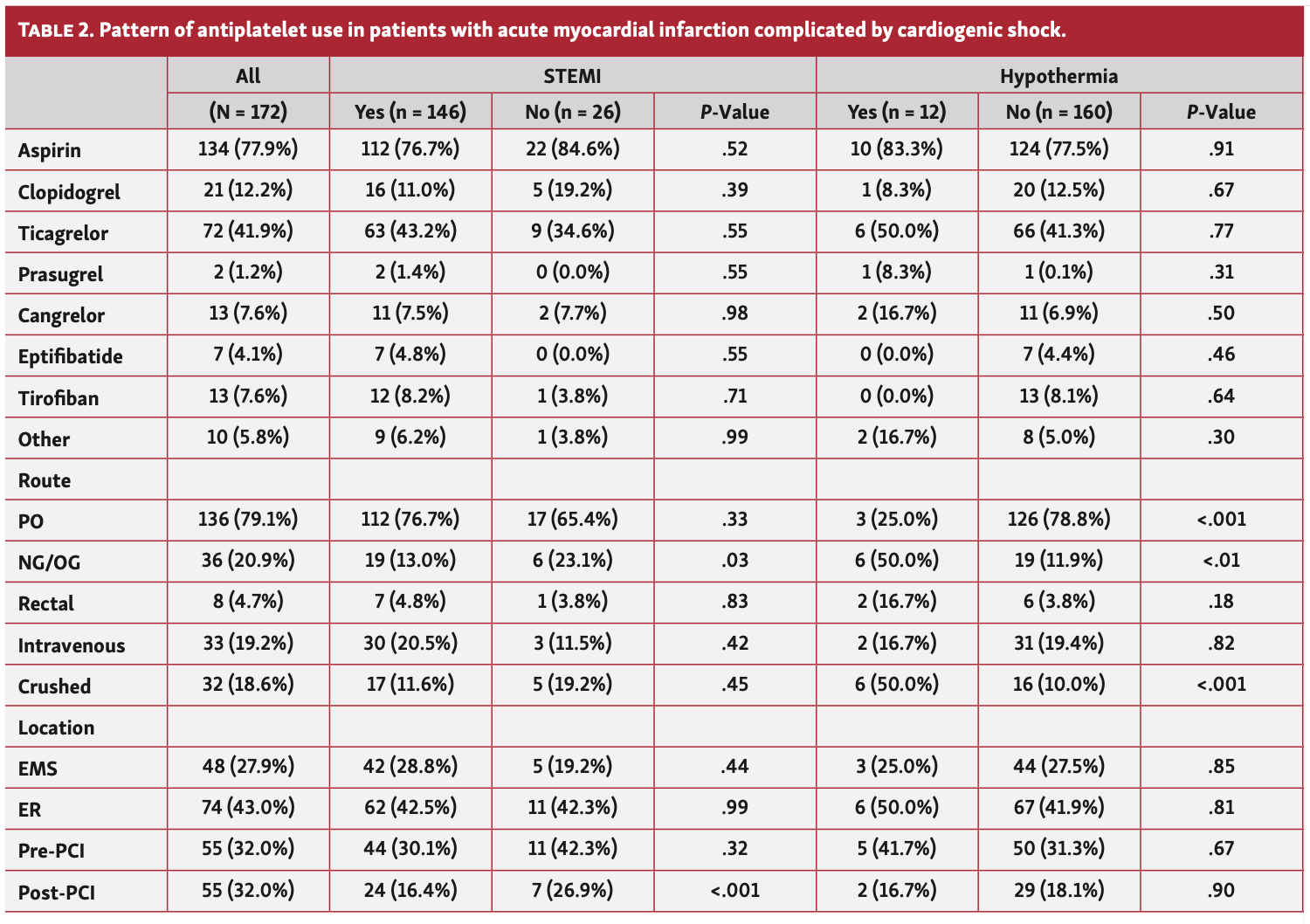
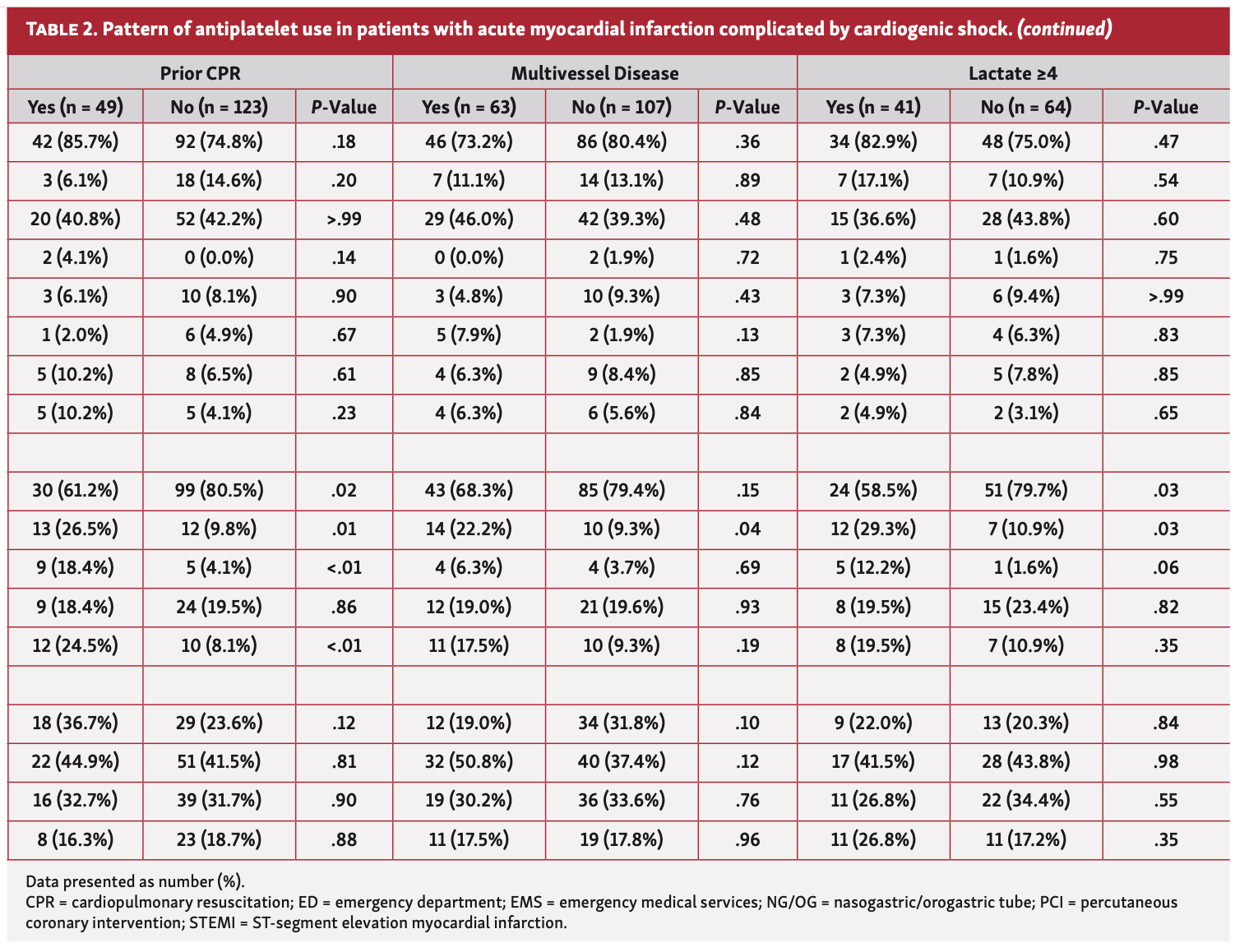
Most patients (84.3%) received at least 1 antiplatelet agent prior to intervention. A total of 146/174 patients (83.9%) who presented with STEMI received an antiplatelet agent prior to PCI, and 86.7% of those with non-STEMI received an antiplatelet agent prior to PCI. In patients who received antiplatelet therapy, 134/172 (77.9%) received aspirin, 95/172 (55.2%) received an oral P2Y12 inhibitor, and 33/172 (19.2%) received an IV antiplatelet agent. Ticagrelor was the most common P2Y12 administered (72/172; 41.9%), followed by clopidogrel (21/172; 12.2%), and prasugrel (2/172; 1.2%). IV antiplatelet agents used included cangrelor (13/172; 7.6%), tirofiban (13/172; 7.6%), and eptifibatide (7/172; 4.1%) (Figure 1). The most common route of administration was oral (136/172 (79.1%), nasogastric/orogastric tube (36/172; 20.9%), IV (33/172; 19.2%), and rectal (8/172; 4.7%). Oral antiplatelet agents were crushed in 18.6% of patients. Patients who underwent therapeutic hypothermia and cardiopulmonary resuscitation were more likely to receive antiplatelet agents via rectal or nasogastric/orogastric tube routes and have them crushed. Those who had lactate >4 mmol/L or had multivessel intervention were more likely to receive antiplatelet therapy via nasogastric/orogastric tube (Table 2, Part 1 and Table 2, Part 2).
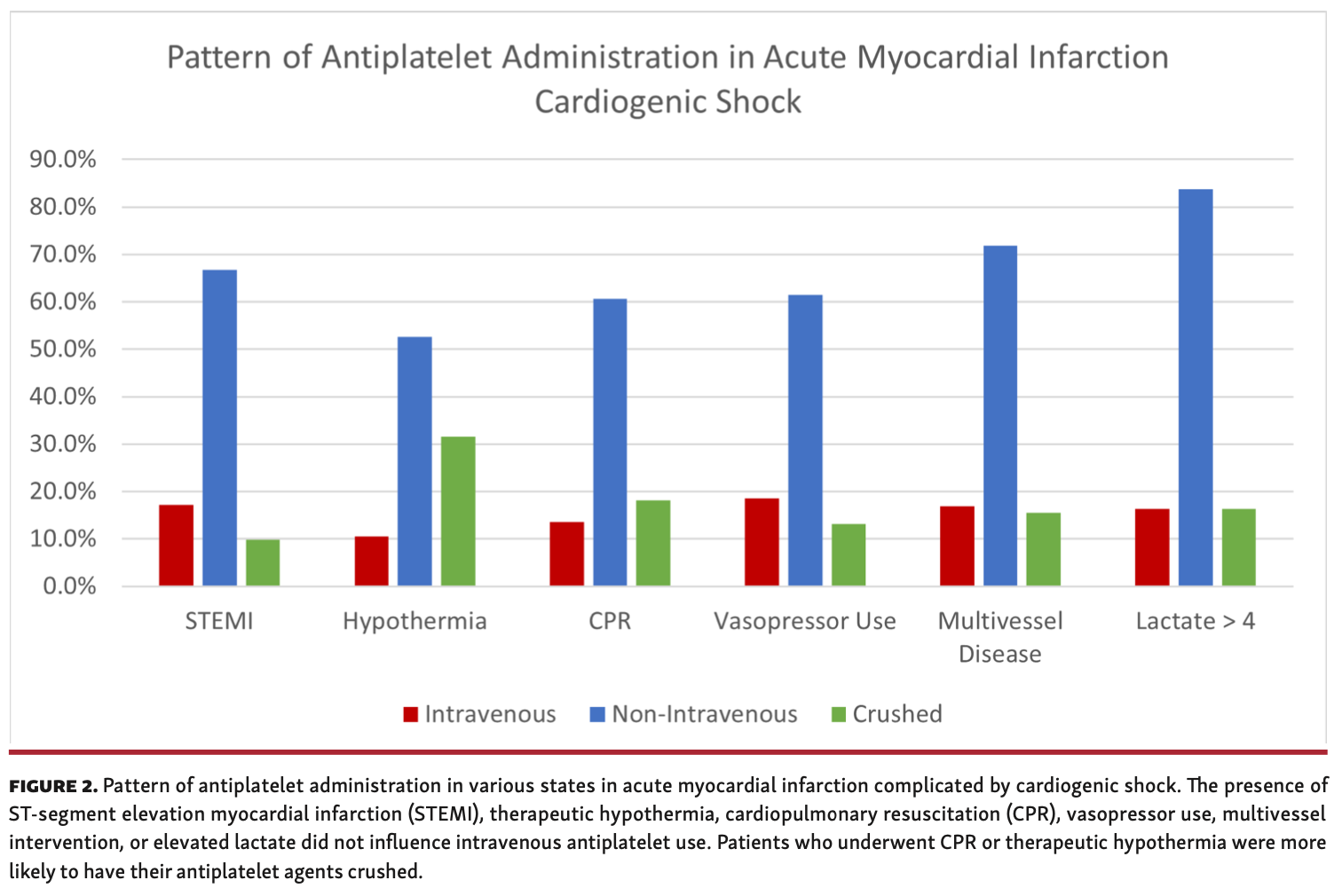
The presence of STEMI, cardiac arrest, cardiopulmonary resuscitation, therapeutic hypothermia, use of vasopressors, and elevated lactate did not influence IV antiplatelet use. Furthermore, single vs multivessel intervention was not associated with a difference in the form or route of antiplatelet administration (Figure 2). There was Thrombolysis in Myocardial Infarction (TIMI) 0 flow in 152/204 patients (74.5%) before PCI and aspiration thrombectomy was performed in 50/204 patients (24.5%). TIMI 0 flow and aspiration thrombectomy were present in higher rates in patients who received IV antiplatelet therapy, but the difference was not statistically significant.
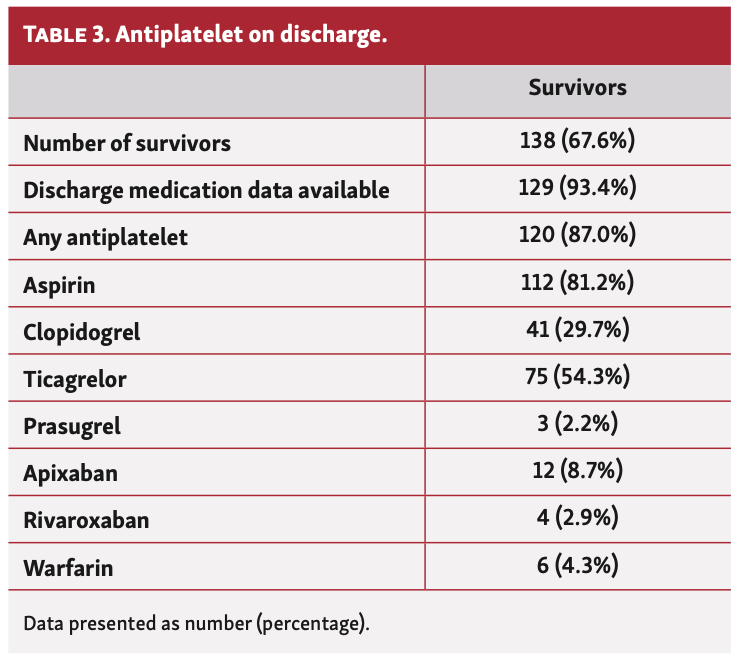
Overall, 67.6% of patients survived to discharge. Discharge medications were available for 129 patients (Table 3). Those who were not placed on DAPT were treated using an antiplatelet agent along with an anticoagulant.
Discussion
Our study demonstrates that in patients who present with AMI-CS undergoing PCI and MCS, the type of antiplatelet used and method of administration is variable. The use of crushed and IV antiplatelet therapy is low despite a significant portion of patients having multivessel coronary disease and a high thrombus burden. The degree of thrombus burden is evidenced by the large number of patients presenting with STEMI (85.3%), high frequency of TIMI 0 flow (74.5%), and an increased need for aspiration thrombectomy (24.5%). Despite this complexity, only 19.2% of patients in AMI-CS received IV antiplatelet agents and only 18.6% had their oral antiplatelet agents crushed.
Patients undergoing PCI for AMI require early, rapid, and potent platelet inhibition to prevent peri-PCI thrombotic events.1 Patients in AMI-CS frequently present with STEMI, cardiac arrest, and multiorgan failure. CS complicates traditional antiplatelet management following PCI due to hemodynamic changes that reduce organ perfusion, impair oral absorption, and cause inflammation, resulting in reduced platelet inhibition.3,4 Pharmacokinetically, several studies have verified the limited and delayed antiplatelet effects in such patients. A prospective study by Adamski et al assessed antiplatelet activity in AMI patients using liquid chromatography and demonstrated that plasma concentrations of P2Y12 inhibitors were one-third lower in STEMI patients as compared with non-STEMI patients.5 Cardiopulmonary resuscitation, frequently performed in AMI-CS patients, results in inflammation that encourages platelet aggregation and lactic acidosis, which reduces platelet inhibition. Therapeutic hypothermia has also been shown to weaken platelet inhibition and independently increases the risk of acute stent thrombosis due to reduced aspirin-mediated platelet inhibition,6 reduced P2Y12-mediated platelet inhibition,7 and reduced drug metabolism.8 To complicate things further, a significant number of patients in AMI-CS develop liver failure and renal injury. Compromised liver function from hepatic congestion impairs cytochrome P-450 activity—the main mediator of drug metabolism4—and renal failure resulting in need for dialysis increases the risk of platelet loss and bleeding events.9 In our analysis of antiplatelet administration patterns, those who required cardiopulmonary resuscitation, underwent hypothermic protocol, or had multiorgan failure were not more likely to receive IV antiplatelets, despite the increased risk of peri-PCI thrombotic events.
The simultaneous use of other medications (opiates, proton-pump inhibitors, and unfractionated heparin) in CS patients also impacts the response to antiplatelet therapies. The use of morphine has been shown to impair platelet inhibition, partly due to prolonged gastric transit.10,11 This resulted in the European Society of Cardiology changing their recommendation for analgesia with morphine from class I to IIa in AMI.2 In addition, the United States Food and Drug Administration required manufacturers of oral P2Y12 inhibitors to state in product labels that administration of opioids with oral P2Y12 inhibitors can result in delayed and reduced concentrations of these agents. Proton-pump inhibitors, routinely used for stress ulcer prophylaxis in the intensive care unit, have been shown to reduce platelet inhibition, increase stent thrombosis, and increase reinfarction rates in patients who undergo PCI on proton-pump inhibitors.12-15 Unfractionated heparin, which is used for MCS, can also reduce platelet number and function. These potential drug interactions further complicate antiplatelet management in this patient population.
The decreased bioavailability and activity of oral antiplatelets is therefore a major concern in patients with AMI-CS due to the factors outlined above. When using oral antiplatelet agents, the best first step is to crush the medications. It is simple, quick, and has been shown to accelerate and increase platelet inhibition in multiple studies using clopidogrel, ticagrelor, and prasugrel.16-18 IV antiplatelet agents are even more effective than crushed oral antiplatelets, and their addition should be strongly considered in this high-risk population, while keeping in mind the risk of bleeding. In patients undergoing primary PCI for STEMI, the CANTIC study prospectively demonstrated that combining cangrelor with crushed ticagrelor significantly improved platelet inhibition without increasing bleeding risk when compared with crushed ticagrelor alone.19 The CHAMPION-PHOENIX study similarly demonstrated that regardless of the form of AMI, patients who underwent PCI and received cangrelor had a significantly reduced risk of ischemic events (all-cause mortality, MI, ischemia-driven revascularization, or stent thrombosis) as compared with clopidogrel, also without increased bleeding.20 In the AMI-CS population, Droppa et al used multiple electrode aggregometry to assess the effect of cangrelor and found that cangrelor overcame problems with reduced absorption and improved platelet inhibition in patients with CS.21 The investigators went on to subsequently perform a matched pair analysis of patients in the IABP-Shock II trial treated with cangrelor vs no cangrelor and found that those treated with cangrelor more frequently experienced >1 TIMI flow grade improvement during PCI (92.9% vs 81.2%; P=.02).22 Vaduganathan et al performed a single-center study evaluating the use of cangrelor and found that 25% of cangrelor use was in CS patients and that those treated with cangrelor had a low rate of severe bleeding events.23
The use of GP IIb/IIIa inhibitors in AMI patients has also been shown to reduce ischemic events and angiographic complications of primary PCI, especially in those with delayed onset of oral antiplatelet action due to hemodynamic compromise.24 Hasdai et al demonstrated that the use of GP IIb/IIIa inhibitors in AMI patients was associated with significantly lower 30-day mortality among those who developed CS.25 In patients with CS who require dialysis, the use of reversible GP IIb/IIIa inhibitors has been shown to preserve platelet number and function. GP IIb/IIIa inhibitors combined with unfractionated heparin during dialysis inhibit platelet activation and platelet-monocyte interactions, resulting in platelet protection, antithrombotic, and anti-inflammatory effects.9
Patients in our study had a high thrombus burden and increased need for aspiration thrombectomy. Aspiration thrombectomy was used in 24.5% of patients, significantly higher than the 10.8% utilization seen nationally.26 Rates of aspiration thrombectomy were similarly high in the CULPRIT-SHOCK trial at 14.5%.27 The CULPRIT-SHOCK trial also demonstrated low rates of IV antiplatelet use, with only 2% of patients receiving cangrelor and 22% receiving GP IIb/IIIa inhibitors.27 It is unclear whether these highly thrombotic lesions led to CS or whether the metabolic changes seen in CS led to poor platelet inhibition and increased thrombotic complications. Either way, the ability to safely achieve TIMI 3 flow is paramount in reducing mortality in AMI-CS patients.28
CS complicates antiplatelet management in acute coronary syndrome. In our study, no single factor that is known to affect platelet inhibition was associated with higher rates of crushed or IV antiplatelet use, including STEMI, cardiopulmonary resuscitation, hypothermia, lactate elevation, and liver dysfunction. The reasons for the decisions are unclear, but factors such as availability, cost, and familiarity with the drugs may play a role.
Study limitations. This is a descriptive analysis collected from the NCSI. The vast majority of case report forms were complete, but a few did not report route or timing of antiplatelet administration. The case report forms are retrospectively filled out by investigators largely using chart review; therefore, details such as timing of antiplatelet administration and whether they were crushed may be difficult to delineate.
Conclusion
The use of crushed and IV antiplatelet agents in AMI-CS patients is low, despite the high burden of multivessel coronary artery disease and high thrombotic burden. Further studies are needed in this high-risk population to assess whether more potent antiplatelet inhibition will improve outcomes.
Affiliations and Disclosures
From the 1Division of Cardiovascular Medicine, Henry Ford Hospital, Detroit, Michigan; 2Orange County Heart Institute and Research Center, Orange California; 3Division of Cardiovascular Medicine, Ascension St. John Hospital and Medical Center, Detroit, Michigan; 4Division of Cardiovascular Medicine, UT Southwestern Medical Center, Dallas, Texas; 5Washington Regional Heart Institute, Fayetteville, Arkansas; 6Parkwest Regional Medical Center, Knoxville, Tennessee; 7Vassar Brothers Hospital, Poughkeepsie, New York; 8Kettering Health Network, Dayton, Ohio; 9Orange Park Medical Center, Orange Park, Florida; 10Division of Cardiovascular Medicine, Texas A&M University, Temple, Texas; 11Spartanburg Medical Center, Spartanburg, South Carolina; and 12Peacehealth, Springfield, Oregon.
Funding: The NCSI is funded by unrestricted research grants from Abiomed and Chiesi USA, Inc. Neither company had direct involvement in the study design or the present analysis.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. Dr Basir is a consultant for Abbott Vascular, Abiomed, Cardiovascular Systems, Inc, Chiesi, Procyrion, and Zoll. Dr O'Neill is a consultant for Abbott Vascular, Abiomed, Boston Scientific, and Edwards Lifesciences. The remaining authors report no conflicts of interest regarding the content herein.
Manuscript accepted May 20, 2021.
Address for correspondence: Sarah Gorgis, MD, Henry Ford Hospital, Cardiovascular Department, 2799 W Grand Blvd, Detroit, MI 48202. Email: sgorgis1@hfhs.org
Related Articles
- A Comparison of In-Hospital Outcomes Between the Use of Impella and IABP in Acute Myocardial Infarction Cardiogenic Shock Undergoing Percutaneous Coronary Intervention
- Mortality in STEMI Patients With Cardiogenic Shock: Results From a Nationwide PCI Registry and Focus on Left Main PCI
- Predictors of Clinical Outcome After Early Veno-Arterial Extracorporeal Membrane Oxygenation in Cardiogenic Shock Complicating ST-Elevation Myocardial Infarction
- VA-ECMO With IABP is Associated With Better Outcome Than VA-ECMO Alone in the Treatment of Cardiogenic Shock in ST-Elevation Myocardial Infarction
- Predictors of Hemodynamic Response to Intra-Aortic Balloon Pump Therapy in Patients With Acute Decompensated Heart Failure and Cardiogenic Shock
- Initiation of Extracorporeal Membrane Oxygenation in the Cardiac Catheterization Laboratory: The Mayo Clinic Experience
- Percutaneous Mitral Valve Repair With MitraClip in Inoperable Patients With Severe Mitral Regurgitation Complicated by Cardiogenic Shock
- Safety of Intravenous Cangrelor Administration for Antiplatelet Bridging in Hospitalized Patients: A Retrospective Study
- Evaluation of a Real-World In-hospital Antiplatelet-Switching Strategy Following Coronary Interventions: The SWITCH Study
References
1. Levine GN, Bates ER, Bittl JA, et al. 2016 ACC/AHA guideline focused update on duration of dual antiplatelet therapy in patients with coronary artery disease: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol. 2016;68(10):1082-1115.
2. Valgimigli M, Bueno H, Byrne RA, et al. 2017 ESC focused update on dual antiplatelet therapy in coronary artery disease developed in collaboration with EACTS: the task force for dual antiplatelet therapy in coronary artery disease of the European Society of Cardiology (ESC) and of the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J. 2018;39(3):213-260.
3. Orban M, Byrne RA, Hausleiter J, Laugwitz KL, Sibbing D. Massive thrombus burden with recurrence of intracoronary thrombosis early after stenting and delayed onset of prasugrel action in a patient with ST-elevation myocardial infarction and cardiac shock. Thromb Haemostas. 2011;106(3):555-558.
4. Weeks PA, Sieg A, Paruthi C, Rajapreyar I. Antiplatelet therapy considerations in ischemic cardiogenic shock: implications of metabolic bioactivation. J Cardiovasc Pharmacol Ther. 2015;20(4):370-377.
5. Adamski P, Sikora J, Laskowska E, et al. Comparison of bioavailability and antiplatelet action of ticagrelor in patients with ST-elevation myocardial infarction and non-ST-elevation myocardial infarction: a prospective, observational, single-centre study. PloS One. 2017;12(10):e0186013.
6. Prüller F, Milke OL, Bis L, et al. Impaired aspirin-mediated platelet function inhibition in resuscitated patients with acute myocardial infarction treated with therapeutic hypothermia: a prospective, observational, non-randomized single-centre study. Ann Intensive Care. 2018;8(1):28.
7. Kaufmann J, Wellnhofer E, Stockmann H, et al. Clopidogrel pharmacokinetics and pharmacodynAMI-CS in out-of-hospital cardiac arrest patients with acute coronary syndrome undergoing target temperature management. Resuscitation. 2016;102:63-69.
8. Tortorici MA, Kochanek PM, Poloyac SM. Effects of hypothermia on drug disposition, metabolism, and response: A focus of hypothermia-mediated alterations on the cytochrome P450 enzyme system. Critical Care Med. 2007;35(9):2196-2204.
9. Link A, Girndt M, Selejan S, Rbah R, Böhm M. Tirofiban preserves platelet loss during continuous renal replacement therapy in a randomised prospective open-blinded pilot study. Crit Care. 2008;12(4):R111.
10. Farag M, Srinivasan M, Gorog D. Morphine use impairs thrombotic status in patients with ST-elevation myocardial infarction undergoing primary percutaneous coronary intervention [abstract]. J Am Coll Cardiol. 2016;67(13 Suppl):40.
11. Adamski P, Buszko K, Sikora J, et al. Determinants of high platelet reactivity in patients with acute coronary syndromes treated with ticagrelor. Scientific Reports. 2019;9(1):3924.
12. Juurlink DN, Gomes T, Ko DT, et al. A population-based study of the drug interaction between proton pump inhibitors and clopidogrel. CMAJ. 2009;180(7):713-718.
13. Bundhun PK, Teeluck AR, Bhurtu A, Huang WQ. Is the concomitant use of clopidogrel and proton pump inhibitors still associated with increased adverse cardiovascular outcomes following coronary angioplasty?: a systematic review and meta-analysis of recently published studies (2012-2016). BMC Cardiovasc Disord. 2017;17(1):3.
14. Hu W, Tong J, Kuang X, Chen W, Liu Z. Influence of proton pump inhibitors on clinical outcomes in coronary heart disease patients receiving aspirin and clopidogrel: a meta-analysis. Medicine. 2018;97(3):e9638.
15. Pang J, Wu Q, Zhang Z, et al. Efficacy and safety of clopidogrel only vs. clopidogrel added proton pump inhibitors in the treatment of patients with coronary heart disease after percutaneous coronary intervention: a systematic review and meta-analysis. Int J Cardiol Heart Vasc. 2019;23:100317.
16. Zafar MU, Farkouh ME, Fuster V, Chesebro JH. Crushed clopidogrel administered via nasogastric tube has faster and greater absorption than oral whole tablets. J Int Cardiol. 2009;22(4):385-389.
17. Rollini F, Franchi F, Hu J, et al. Crushed prasugrel tablets in patients with STEMI undergoing primary percutaneous coronary intervention: the CRUSH study. J Am Coll Cardiol. 2016;67(17):1994-2004.
18. Ratcovich H, Sadjadieh G, Andersson HB, et al. The effect of ticagrelor administered through a nasogastric tube to comatose patients undergoing acute percutaneous coronary intervention: the TICOMA study. EuroIntervention. 2017;12(14):1782-1788.
19. Franchi F, Rollini F, Rivas A, et al. Platelet inhibition with cangrelor and crushed ticagrelor in patients with ST-segment-elevation myocardial infarction undergoing primary percutaneous coronary intervention. Circulation. 2019;139(14):1661-1670.
20. Bhatt DL, Stone GW, Mahaffey KW, et al. Effect of platelet inhibition with cangrelor during PCI on ischemic events. N Engl J Med. 2013;368(14):1303-1313.
21. Droppa M, Borst O, Rath D, et al. Impact of intravenous P2Y12-receptor inhibition with cangrelor in patients presenting with acute coronary syndrome and cardiogenic shock - a case series. Cell Physiol Biochem. 2017;42(4):1336-1341.
22. Droppa M, Vaduganathan M, Venkateswaran RV, et al. Cangrelor in cardiogenic shock and after cardiopulmonary resuscitation: a global, multicenter, matched pair analysis with oral P2Y12 inhibition from the IABP-SHOCK II trial. Resuscitation. 2019;137:205-212. Epub 2019 Feb 18.
23. Vaduganathan M, Qamar A, Badreldin HA, et al. Cangrelor use in cardiogenic shock. JACC Cardiovasc Interv. 2017;10(16):1712-1714.
24. Dziewierz A, Rakowski T, Dudek D. Abciximab in the management of acute myocardial infarction with ST-segment elevation: evidence-based treatment, current clinical use, and future perspectives. Ther Clin Risk Manag. 2014;10:567-576.
25. Hasdai D, Harrington RA, Hochman JS, et al. Platelet glycoprotein IIb/IIIa blockade and outcome of cardiogenic shock complicating acute coronary syndromes without persistent ST-segment elevation. J Am Coll Cardiol. 2000;36(3):685-692.
26. Secemsky EA, Ferro EG, Rao SV, et al. Association of physician variation in use of manual aspiration thrombectomy with outcomes following primary percutaneous coronary intervention for ST-elevation myocardial infarction: the National Cardiovascular Data Registry CathPCI Registry. JAMA Cardiol. 2019;4(2):110-118.
27. Thiele H, Akin I, Sandri M, et al. PCI strategies in patients with acute myocardial infarction and cardiogenic shock. N Engl J Med. 2017;377(25):2419-2432.
28. Overtchouk P, Barthelemy O, Hauguel-Moreau M, et al. Angiographic predictors of outcome in myocardial infarction patients presenting with cardiogenic shock: a CULPRIT-SHOCK angiographic substudy. EuroIntervention. 2021;16(15):e1237-e1244.











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}