

Comparison of Vascular Closure Devices vs Manual Compression After Femoral Artery Puncture in Patients on Oral Anticoagulation — Post Hoc Analysis of the ISAR-CLOSURE Trial
Abstract
Objectives. To compare vascular closure devices (VCD) with manual compression (MC) in patients on chronic oral anticoagulation (OAC) who undergo diagnostic coronary angiography in terms of vascular access-site complications. Methods. This is a subanalysis of 604 patients that had undergone transfemoral diagnostic coronary angiography and were randomly assigned to arteriotomy closure with either VCDs (intravascular FemoSeal VCD or extravascular EXOSEAL VCD) or MC within the large scale, randomized ISAR-CLOSURE trial. Primary endpoint was the composite of access-site-related vascular complications at 30 days. Secondary endpoints were time to hemostasis and repeat MC. Results. Vascular access-site complications were similar in patients assigned to VCDs compared to MC (8.2% vs 10.6%; P=.33). There was no interaction of treatment effect and OAC (P interaction = 0.59). Rates of pseudoaneurysms were lower with VCDs (0.8% vs 3.2%; P=.02). Time to hemostasis was significantly shortened with VCDs compared to MC (1 [IQR 0.5-2.0] min vs 12 [IQR 10-15] min; P<.001). There was no difference regarding repeat MC in both groups (VCD 1.5% vs MC 0.5%; P=.23). Time to hemostasis (0.5 [0.2-1.0] min, vs 2.0 [1.75-2.0] min; P<.001) and closure device failure (3.7% vs 17.2%; P<.001) were lower with the intravascular VCD, compared with the extravascular VCD. Conclusions. In patients on chronic OAC undergoing transfemoral diagnostic coronary angiography, the use of VCDs was comparable to MC regarding the primary combined endpoint of vascular access-site related complications. VCDs reduced the occurrence of pseudoaneurysms and time to hemostasis.
Key words: bleeding complications, pseudoaneurysms, vascular closure devices
Introduction
Bleeding complications during percutaneous coronary angiography and interventions (PCI) are associated with a mortality increase.1 A major criterion for high bleeding risk at the time of PCI is concomitant use of long-term oral anticoagulation (OAC).2 Vascular access complications, such as bleeding, considerably contribute to the morbidity of these patients. It is therefore recommended to use the radial artery to reduce bleeding complications during coronary angiography and PCI, 3 however, femoral access still is widely used. Traditionally, manual compression (MC) has been used to achieve hemostasis after femoral artery puncture. Then, with the aim of improving both efficacy and safety, vascular closure devices (VCD) were introduced into clinical practice about 20 years ago.
Contemporary VCDs have been shown to reduce access-site complications as compared to MC4,5 and may even be associated with a prognostic benefit.6 The reduction of bleeding with VCDs is pronounced in high-risk patients who receive anticoagulants in the setting of acute myocardial infarction.7
There is limited evidence from large-scale randomized trials on the performance of contemporary VCDs compared to MC in patients on chronic OAC. The Instrumental Sealing of ARterial Puncture Site—CLOSURE Device vs Manual Compression (ISAR-CLOSURE) trial proved that in patients undergoing transfemoral diagnostic coronary angiography VCDs were non-inferior to MC in terms of vascular access-site complications and reduced time to hemostasis.8 We therefore aimed to compare VCDs with MC in patients on OAC who were enrolled in the ISAR-CLOSURE trial in terms of vascular access-site complications.
Methods
Study design. A detailed description of the investigator-initiated, large-scale, multicenter, randomized, open-label ISAR-CLOSURE trial design and main results has previously been published.8,9 The trial was performed with the approval of the ethics committee at each participating center, and all patients provided written informed consent. The current analysis aims to assess the value of VCDs compared with MC in patients enrolled in the ISAR-CLOSURE trial who were on OAC.
Patient population. Patients were enrolled from April 2011 to May 2014 if they had given their written informed consent and underwent diagnostic coronary angiography with a 6 French sheath via the common femoral artery which had to have a diameter of >5 mm (proven by angiography). Main exclusion criteria were previous implantation of a VCD, symptomatic leg ischemia, prior thrombo-endarterectomy, patch plastic of the common femoral artery, planned invasive diagnostic/interventional procedure, heavily calcified vessel, active bleeding, bleeding diathesis, severe arterial hypertension, local infection, autoimmune disease, allergy to resorbable suture and pregnancy.9
According to clinical routine, vitamin K antagonist (VKA) therapy was paused in stable patients and coronary angiography was performed when the INR value was ≤ 1.8. Non-vitamin K oral anticoagulant (NOAC) therapy was paused 24h-48h before coronary angiography.
Study treatment. Eligible patients were randomized in a 1:1:1 fashion to arteriotomy closure with one of the following techniques: the intravascular FemoSeal VCD (St. Jude Medical Systems), the extravascular EXOSEAL VCD (Cordis Corp.) or manual compression. Allocation to treatment was performed with sealed opaque envelopes containing a computer-generated sequence. In patients randomized to VCD treatment, the VCDs were deployed according to the instructions for use under strictly sterile conditions. Investigators participating in the trial were instructed and certified from the manufacturer of the respective VCD. In patients assigned to manual compression, the sheath was removed by a physician and groin compression was performed until adequate hemostasis was achieved. Bed rest was recommended for all treatment groups. A pressure bandage was applied for 2 hours after VCD implantation and 6 hours after manual compression.
Follow-up. After removing the pressure bandage, the access-site was clinically inspected and mobilization allowed where considered appropriate. Before hospital discharge, all patients were scheduled to undergo color-coded duplex sonography of the access-site. Patients were contacted by letter, telephone or out-patient visit for clinical follow-up at 30 days after randomization. Those who reported complaints related to the access-site were invited for further clinical and duplex sonographic examination.
Endpoints and definitions. The primary endpoint is the incidence of vascular access-site complications, defined as the composite of hematoma ≥5 cm, arteriovenous fistula, pseudoaneurysm, access-site related major bleeding, acute ipsilateral leg ischemia, need for vascular surgical or interventional treatment or local infection at 30 days after randomization. Secondary endpoints are time to hemostasis and repeat manual compression. Definition of access-site related major bleeding is based on REPLACE-2 criteria10 and includes a reduction in hemoglobin of ≥3 g/dL with evident bleeding, a reduction in hemoglobin of ≥4 g/dL with or without evident bleeding or bleeding requiring blood transfusion.11
Statistical analysis. The present analysis aims to assess the safety and efficacy of VCDs compared with MC in patients on OAC undergoing transfemoral diagnostic coronary angiography in the randomized ISAR-CLOSURE trial. Categorical data are presented using frequencies and proportions and were analysed with the use of Chi-squared test or Fisher’s exact test, as appropriate. Continuous variables were summarized using median [25th, 75th percentiles] and compared using nonparametric Wilcoxon rank-sum test. We assessed the interaction between OAC and treatment effect with respect to the primary endpoint by logistic regression. All analyses were conducted in a blinded manner regarding the randomly-assigned treatment and were performed on an intention-to-treat principle. A P-value of <.05 was considered an indication of statistical significance. All analyses were performed using R (version 4.0.0.; R Foundation for Statistical Computing).
Results
Patients and procedures. In the ISAR-CLOSURE trial, 4524 patients were enrolled and 604 patients (13%) were on oral anticoagulation (OAC) on admission. 388 patients received VCDs and 216 patients underwent MC.
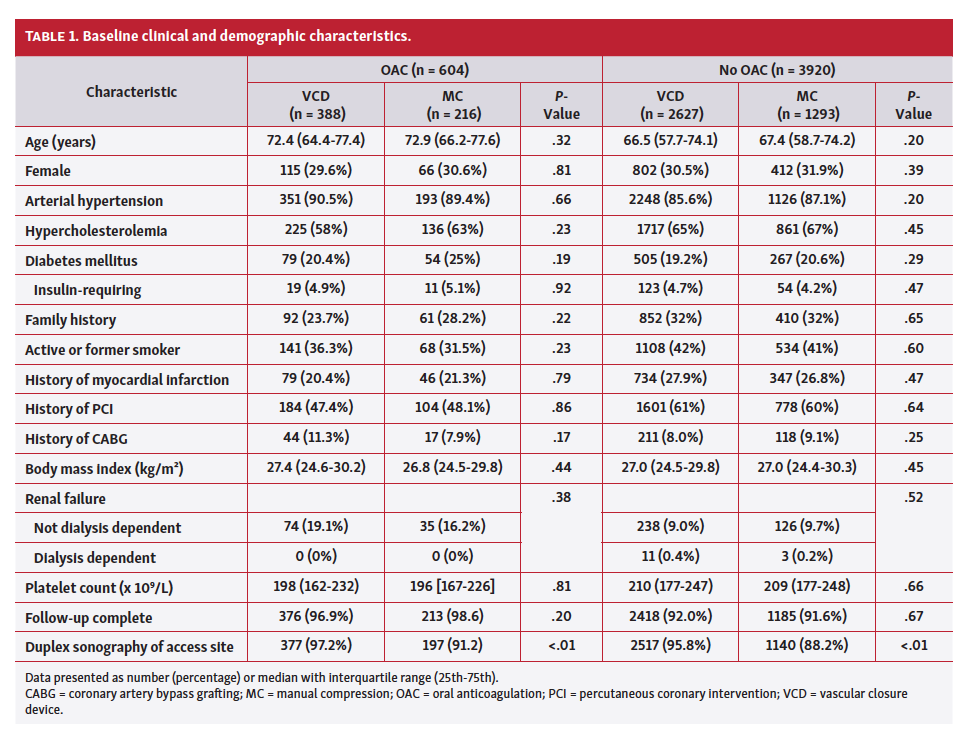
Patients with OAC on admission were older, more often had renal failure and less often a history of myocardial infarction (MI) or percutaneous coronary intervention (PCI) than patients without OAC therapy (Table 1).
In total, 95% of patients on OAC underwent duplex sonography of the access site before hospital discharge. Clinical follow-up at 30 days was available for 97% of patients. Only 1 patient (0.2%) underwent neither duplex sonographic examination of the access site nor clinical follow-up at 30 days.
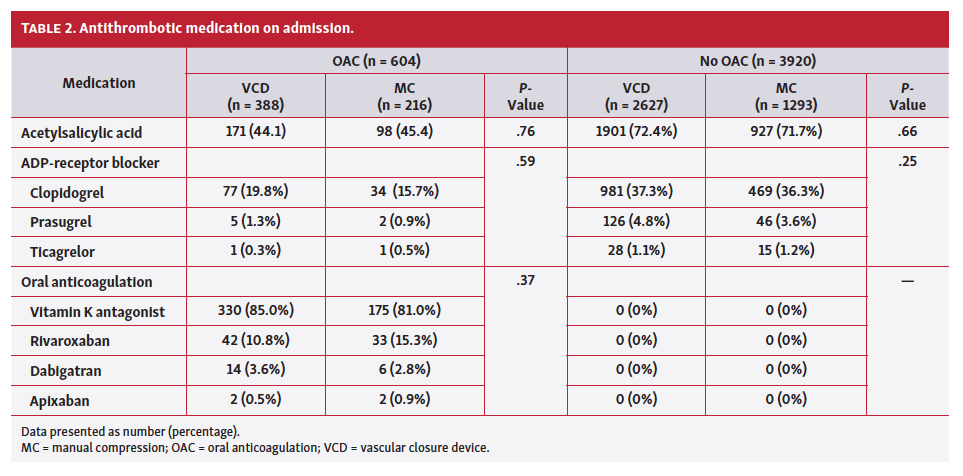
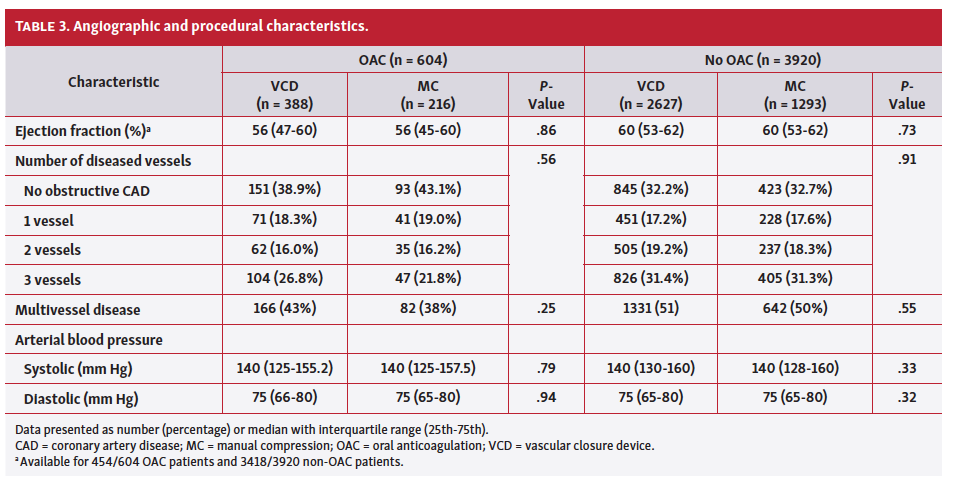
Baseline clinical and demographic characteristics according to treatment allocation to VCD or MC are shown in Table 1, and the antithrombotic medication on admission is summarized in Table 2. A total of 44% of patients received aspirin and about 20% received an adenosine-diphosphate (ADP) receptor blocker. All patients were on an oral anticoagulant and the majority of patients received VKAs (84%). Angiographic and procedural characteristics are presented in Table 3.
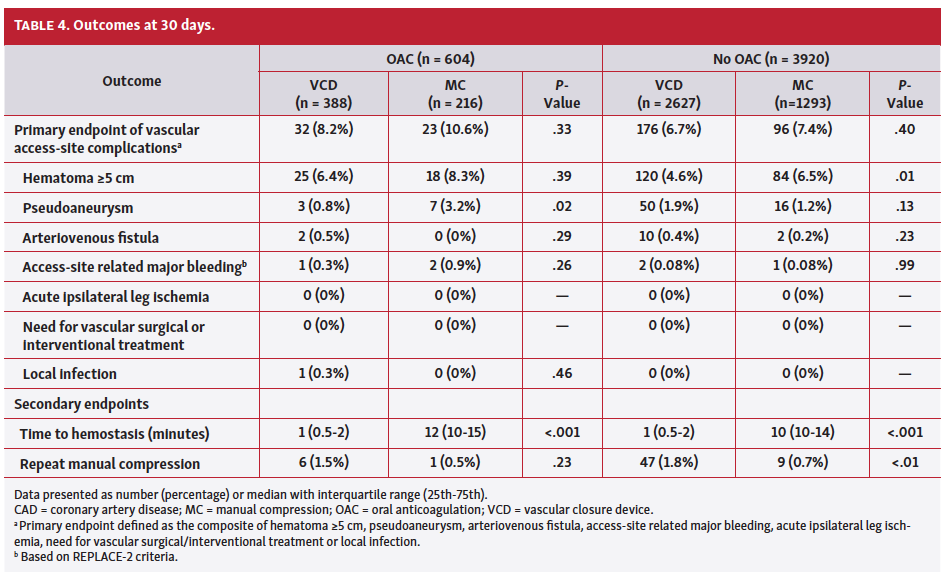
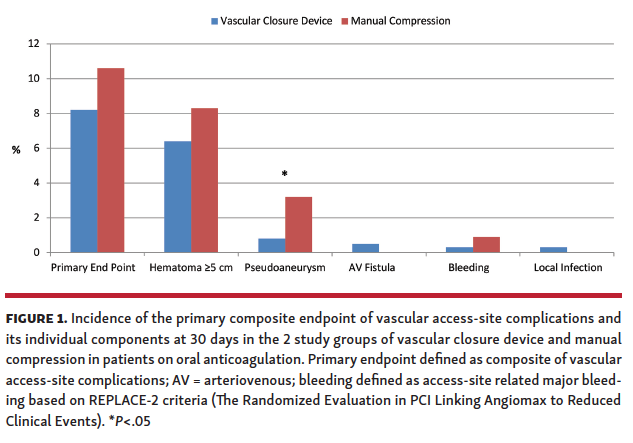
Primary comparison between VCD and manual compression. In patients on OAC, the primary composite endpoint was not significantly different in patients assigned to VCD compared with MC (32 VCD patients [8.2%] vs 23 MC patients [10.6%]; P=.33) (Figure 1, Table 4). There was no interaction of treatment effect with VCD or MC and OAC with regard to the primary endpoint (P interaction=.59). There was no difference in the incidence of hematomas in OAC patients assigned to VCD (25 VCD patients [6.4%] vs 18 MC patients [8.3%]; P=.39).
There were statistically fewer patients with pseudoaneurysm occurrence with VCDs (3 VCD patients [0.8%] vs 7 MC patients [3.2%]; P=.02).
Time to hemostasis was significantly shortened with the use of VCD compared to MC (1 min [IQR, 0.5 -2.0 min] vs 12 min [IQR, 10-15 min], respectively; P<.001). There was no difference regarding repeat MC after initial hemostasis in both groups (6 VCD patients [1.5%] vs 1 MC patient [0.5%]; P=.23).
No patient required interventional treatment or vascular surgery and no patient suffered from acute ipsilateral leg ischemia. There was 1 case of an access-site infection within 30 days in the VCD group. One patient assigned to MC died.
Secondary comparison between intravascular vs extravascular VCDs. Supplemental Table S1 summarizes the baseline clinical and demographic characteristics according to treatment allocation to receive an intravascular VCD (n = 190, FemoSeal) or extravascular VCD (n = 198, Exoseal). Antithrombotic medication on admission is depicted in Supplemental Table S2. Angiographic and procedural characteristics are shown in Supplemental Table S3.
Clinical outcomes according to treatment allocation to the intravascular VCD or extravascular VCD are reported in Supplemental Table S4. The primary composite endpoint was not statistically different in patients assigned to intravascular VCD compared with extravascular VCD (13 patients [6.8%] vs 19 patients [9.6%]; P=.32). In patients on OAC, time to hemostasis (0.5 min [IQR, 0.2-1.0 min] vs 2.0 min [IQR, 1.75-2.0 min]; P<.001) and closure device failure (7 patients [3.7%] vs 34 patients [17.2%]; P<.001) were lower with the intravascular VCD compared with the extravascular VCD.
Intravascular or extravascular VCD vs manual compression. The primary composite endpoint was also not statistically different in patients assigned to an intravascular VCD or extravascular VCD compared to MC respectively (13 patients [6.8%]) with the intravascular VCD vs 23 patients [10.6%] with MC; P=.18) and (19 patients [9.6%] with the extravascular VCD vs 23 patients [10.6%] with MC; P=.72).
Impact of anticoagulation. The primary composite endpoint of access-site related vascular complications occurred more often in patients on OAC vs patients without OAC (Table 4: 55 patients on OAC [9.1%] vs 272 patients without OAC [6.9%]; P=.05). Hematomas were more often observed in patients on OAC vs those with no OAC (43 patients on OAC [7.1%] vs 204 patients with no OAC [5.2%]; P=.05).
Patients with NOACs as compared with VKA had similar outcomes regarding the primary endpoint, the occurrence of hematomas, or pseudoaneurysms.
Discussion
This post hoc analysis reports the largest randomized comparison of VCDs with MC in patients on chronic OAC. The main findings are the following: (1) There was no difference regarding the composite primary endpoint of the occurrence of vascular access site complications between both study groups. (2) There were significantly fewer pseudoaneurysms in the VCD group and (3) time to hemostasis was significantly reduced with VCDs as compared to MC.
The large scale randomized ISAR-CLOSURE trial showed that VCDs were noninferior to MC in terms of vascular access-site complications.8 One limitation of that trial was, that patients who were at higher risk for access-site complications (eg, PCI patients) were not studied.
In this post hoc analysis of the ISAR-CLOSURE trial we therefore focused on other well-known high-risk patients such as those who were on chronic OAC.2 We could show that vascular access-site complications, including bleeding complications, occurred significantly more often in these patients as compared to those without OAC. Reduction of bleeding complications is of utmost importance in patients on OAC who undergo transarterial cardiac procedures. Although it is recommended to use the radial access route in patients with high bleeding risk,3 one third of patients with concomitant OAC still undergo catheterization via the femoral route for various reasons.12
The results of this subgroup analysis in patients with OAC are in line with the results of the main trial and showed similar rates for the primary endpoint of combined vascular access-site complications for VCD and MC. There was no interaction of OAC with treatment effect on the primary endpoint of vascular access-site complications. Therefore, current data reassure that the use of VCD is also safe in patients with OAC. In addition, the rate of femoral pseudoaneurysms was significantly reduced in anticoagulated patients who received VCDs as compared to MC. This is of clinical importance because pseudoaneurysms can lead, if untreated, to life threatening complications such as major bleeding, distal embolization, infections and the compression of surrounding arteries, veins or nerves. Treatment of pseudoaneurysms prolongs hospital stay. In current practice, it is standard treatment to perform ultrasound-guided compression therapy and/or percutaneous thrombin injection.13
In the main ISAR-CLOSURE trial, the hematoma rate was significantly reduced with VCDs vs MC. In this subgroup analysis, the incidence of hematoma was only numerically lower but not statistically significant, which may be attributed to the smaller patient population.
Other trials studied patients with acute myocardial infarction (AMI) and could show a significant reduction of vascular events14 or major bleeding with VCDs.7 There are several differences in our population, however. Firstly, coronary angiography was performed only when VKAs were paused and the INR was ≤1,8 or when NOACs were paused for at least 24 hours. In contrast, AMI patients in the other trials received periprocedural anticoagulants such as unfractionated heparin plus a glycoprotein IIb/IIIa inhibitor or bivalirudin. Secondly, we studied only patients who did not undergo PCI, and therefore 60% of patients were not on additional antithrombotic therapy, as compared to the AMI patients who were on dual antiplatelet therapy.7
It may be assumed, that the reduction in bleeding with the use of VCDs vs MC would be more pronounced in unstable patients who need urgent coronary angiography, and therefore OAC therapy cannot be paused before undergoing PCI.
An advantage of VCDs as compared to MC is the shorter time to hemostasis which was reduced from 12 minutes to 1 minute in this trial. Time to hemostasis was further reduced with the intravascular VCD as compared to the extravascular VCD. In addition, the extravascular VCD had a high rate of closure device failure as compared to the intravascular VCD. In a previous post hoc analysis of the ISAR-CLOSURE trial, the use of the intravascular FemoSeal VCD was associated with a reduction in vascular access-site complications driven by fewer hematomas when compared to MC.5
Patients on chronic OAC who undergo transarterial cardiac procedures are challenging for the treating physician. Peri- and post-procedural antithrombotic therapies need to be adjusted accordingly to reduce the bleeding risk without increasing the risk for ischemic events.15 Furthermore, the radial access route is recommended. When the femoral route is chosen, the results of this analysis suggest that it is superior to use VCDs to reduce the rate of pseudoaneurysms and time to hemostasis.
Study limitations. This subgroup analysis suffers from the same limitations as previously described for the ISAR-CLOSURE trial, ie, its open-label nature and the exclusion of patients undergoing PCI. In this analysis, we included 13% of patients of the main trial, and, therefore, its power is limited, and the results of this analysis are hypothesis generating. We did not adjust for multiple testing and hidden confounders cannot be excluded. However, this is the largest trial with patients on chronic OAC who were studied to receive either VCD or MC. The majority of patients received VKAs and further studies are needed in patients with VCDs and NOAC therapy.
Conclusion
In patients on chronic OAC undergoing transfemoral diagnostic coronary angiography, the use of VCDs was comparable to MC regarding the primary combined endpoint of vascular access-site-related complications. VCDs reduced the occurrence of pseudoaneurysms and time to hemostasis. Additional studies are needed to assess the value of VCDs in patients on OAC who receive NOACs and who undergo PCI.
Affiliations and Disclosures
From the 1Klinik fuer Herz- und Kreislauferkrankungen, Deutsches Herzzentrum Muenchen, Germany; 2Klinik fuer Innere Medizin II, Krankenhaus Barmherzige Brueder Muenchen, Germany; 3Kardiologie und Pneumologie; Klinikum Landkreis Erding, Germany; and 4Klinik und Poliklinik für Innere Medizin I, Klinikum rechts der Isar, Technische Universitaet Muenchen, Germany.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest.
Manuscript accepted March 17, 2021.
Address for correspondence: PD Dr med Nikolaus Sarafoff, Klinik fuer Herz- und Kreislauferkrankungen, Deutsches Herzzentrum Muenchen, Lazarettstr. 36, 80363 Muenchen, Germany. Email: n.sarafoff@gmail.com
References
1. Research Consortium definition of bleeding in patients with coronary artery disease undergoing percutaneous coronary intervention. Circulation. 2012;125:1424-1431. ePub 2012 Feb 17.
2. Urban P, Mehran R, Colleran R, et al. Defining high bleeding risk in patients undergoing percutaneous coronary intervention. Circulation. 2019;140:240-261.
3. Knuuti J, Wijns W, Saraste A, et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur Heart J. 2020;41:407-477.
4. Jiang J, Zou J, Ma H, et al. Network meta-analysis of randomized trials on the safety of vascular closure devices for femoral arterial puncture site haemostasis. Sci Rep. 2015;5:13761.
5. Mankerious N, Mayer K, Gewalt SM, et al. Comparison of the FemoSeal vascular closure device with manual compression after femoral artery puncture — post hoc analysis of a large-scale, randomized clinical trial. J Invasive Cardiol. 2018;30:235-239.
6. Farooq V, Goedhart D, Ludman P, de Belder MA, Harcombe A, El-Omar M. Relationship between femoral vascular closure devices and short-term mortality from 271 845 percutaneous coronary intervention procedures performed in the United Kingdom between 2006 and 2011: a propensity score-corrected analysis from the British Cardiovascular Intervention Society. Circ Cardiovasc Interv. 2016;9(6). e003560.
7. Sanborn TA, Tomey MI, Mehran R, et al. Femoral vascular closure device use, bivalirudin anticoagulation, and bleeding after primary angioplasty for STEMI: results from the HORIZONS-AMI trial. Catheter Cardiovasc Interv. 2015;85:371-379.
8. Schulz-Schupke S, Helde S, Gewalt S, et al. Comparison of vascular closure devices vs manual compression after femoral artery puncture: the ISAR-CLOSURE randomized clinical trial. JAMA. 2014;312:1981-1987.
9. Xhepa E, Byrne RA, Schulz S, et al. Rationale and design of a randomised clinical trial comparing vascular closure device and manual compression to achieve haemostasis after diagnostic coronary angiography: the Instrumental Sealing of ARterial puncture site — CLOSURE device versus manual compression (ISAR-CLOSURE) trial. EuroIntervention. 2014;10:198-203.
10. Lincoff AM, Kleiman NS, Kereiakes DJ, et al. Long-term efficacy of bivalirudin and provisional glycoprotein IIb/IIIa blockade vs heparin and planned glycoprotein IIb/IIIa blockade during percutaneous coronary revascularization: REPLACE-2 randomized trial. JAMA. 2004;292:696-703.
11. Lincoff AM, Bittl JA, Harrington RA, et al. Bivalirudin and provisional glycoprotein IIb/IIIa blockade compared with heparin and planned glycoprotein IIb/IIIa blockade during percutaneous coronary intervention: REPLACE-2 randomized trial. JAMA. 2003;289:853-863.
12. Cannon CP, Bhatt DL, Oldgren J, et al. Dual antithrombotic therapy with dabigatran after PCI in atrial fibrillation. N Engl J Med. 2017;377:1513-1524.
13. Stolt M, Braun-Dullaeus R, Herold J. Do not underestimate the femoral pseudoaneurysm. Vasa. 2018;47:177-185.
14. Applegate RJ, Grabarczyk MA, Little WC, et al. Vascular closure devices in patients treated with anticoagulation and IIb/IIIa receptor inhibitors during percutaneous revascularization. J Am Coll Cardiol. 2002;40:78-83.
15. Collet JP, Thiele H, Barbato E, et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur Heart J. 2021;42:1289-1367.









