

Long-term Clinical Outcomes of Excimer Laser Coronary Atherectomy for the Management of Recurrent In-stent Restenosis
Abstract
BACKGROUND. Recurrent in-stent restenosis (ISR) remains a serious problem. Optimal modification of the underlying mechanism during index percutaneous coronary intervention (PCI) is key to prevent ISR. Excimer laser coronary atherectomy (ELCA) has its own indications and is among others used in recurrent ISR in case of stent underexpansion and/or diffuse neointimal hyperplasia. We aimed to assess the long-term clinical outcomes of ELCA for the management of recurrent ISR. METHODS. A multicenter, retrospective observational study was conducted. Patients with recurrent ISR who were additionally treated with ELCA were included. The primary outcome was major adverse cardiac events (MACE) defined as a composite of cardiovascular death, myocardial infarction, stroke, target lesion revascularization at 12 months, and longer term. RESULTS. Between 2014 and 2022, 51 patients underwent PCI with the additional use ELCA for recurrent ISR. Primary outcome occurred in 6 patients (11.8%) at 12 months and in 12 patients (23.5%) at a median follow-up of 4 (1-6) years. Technical and procedural success were achieved in 92% and 90% of cases, respectively. Coronary perforation occurred in 2 patients as a result of distal wire perforation, but was not ELCA-related. There were no in-hospital MACE. CONCLUSIONS. ELCA appears to be a safe method with acceptable long-term results for the management of recurrent ISR.
J INVASIVE CARDIOL 2023;35(7):E365-E374. doi: 10.25270/jic/22.00380. Epub 2023 June 18
Key words: laser, atherectomy, stent failure, in-stent restenosis, PCI
Target lesion revascularization (TLR) of ISR remains a serious problem after PCI.1 Prevention is key, and includes optimal stent expansion during index PCI with modification of calcified lesions using plaque modification techniques. These may include high-pressure balloons, scoring/cutting balloons, and/or atherectomy devices. This preparation should preferably be guided by intracoronary imaging, as coronary angiography is a poor discriminator of calcium distribution and thickness.2
A classification on disease process in ISR has been introduced ranging from type I to V, with type I accounting for a mechanical morphology (type IA stent underexpansion and type IB stent fracture), type II for a biologic morphology (type IIA neointimal hyperplasia, type IIB non-calcified neo-atherosclerosis, and type IIC calcified neo-atherosclerosis), a mixed pattern in type III, a CTO in type IV, and 2 or more layers of stent for a type V ISR.3 These different types of ISR result in different treatment options including high-pressure non-compliant (NC) balloon dilatation, intravascular lithotripsy, or ablative devices. However, their use can be limited by low technical success and/or increased complications.1,4 Despite adequate plaque modification and stent expansion, some patients present with recurrent diffuse in-stent hyperplasia, a difficult to treat entity.
ELCA has its own niche to achieve procedural success in recalcitrant ISR, stent underexpansion, and chronic total occlusions (CTO), but may not facilitate dense calcium modification as other dedicated atherectomy devices do.5-7 Moreover, there is limited data regarding the use of ELCA in ISR.
In this multi-center registry, we aimed to assess the clinical outcomes of ELCA for the management of recurrent ISR.
Methods
Study design. We undertook a multi-center, retrospective, observational study. The study was conducted in accordance with the Declaration of Helsinki and Good Clinical Practice guidelines. Baseline, procedural, and clinical outcome data were prospectively collected, validated, and entered into the databases, which were analyzed retrospectively.
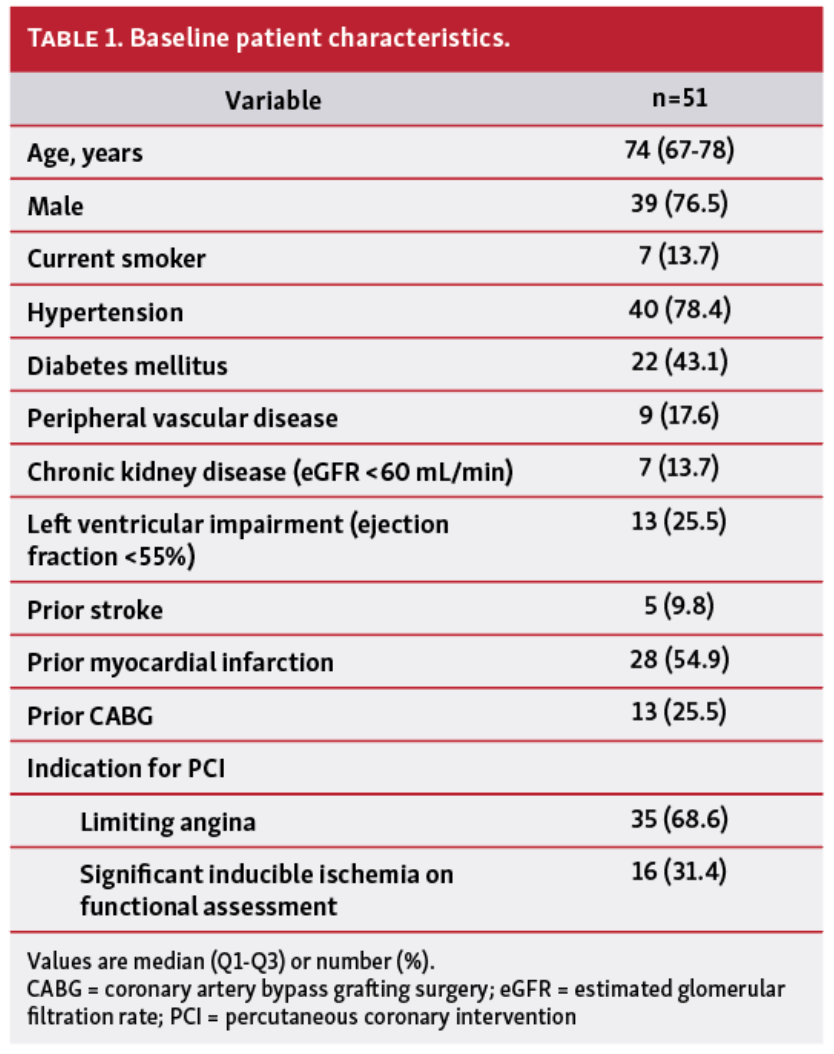
Study population. Patients with recurrent ISR, an indication for revascularization, and the use of additional ELCA were included (Table 1). ISR has been defined as a reduction of 50% of the luminal diameter within the previously stented segment or within 5 mm from the stent edges as assessed by coronary angiography.8
The mechanism of ISR was reported (type I to V). The number of stent layers and the use of a prior drug-coated balloon (DCB) are described. The mechanism of ISR was based on the use of intracoronary imaging, angiography, or stent enhancement techniques. Stent underexpansion was defined as ≥30% stenosis at discretion of the operator.
PCI and ELCA procedures. All patients treated with ELCA (Spectranetics) with either a .9 mm or 1.4 mm diameter catheter were included. A .9 mm diameter catheter was used when a crossing problem was expected. A 1.4 mm diameter catheter was used for debulking and/or treatment of an under-expanded stent. Excimer energy was delivered at a pulse frequency of 25 to 80 Hz and a fluency from 30 to 80 mJ/mm². ELCA with saline media was mainly used. Contrast media was used when saline or blood media did not achieve adequate crossing or stent expansion. Final stent optimization using (high pressure) non-compliant balloon dilatation was performed to ensure stent expansion, with or without additional stent placement or DCB.
Study outcomes and definitions. The primary study outcome was MACE, defined as a composite of cardiovascular death, myocardial infarction, stroke, target lesion revascularization at 12 months, and at long-term follow-up. The individual components of MACE were defined according to the academic research consortium-2 consensus document.9 Secondary outcomes included technical success, procedural success, procedural complications, and non-cardiovascular death at 12 months and long-term follow-up. Technical success was defined as achievement of TIMI grade 3 antegrade flow in the distal vessel with <30% residual stenosis of the treated segment at the end of the procedure. Procedural success was defined as technical success plus the absence of in-hospital MACE.
Statistical analysis. Data are presented as median and Q1-Q3 or number (%). Analyses were performed with Stata V.15.1 (StataCorp).
Results
Between 2014 and 2022, 51 patients underwent PCI with additional ELCA for recurrent ISR in 4 cardiac centers in Belgium and The United Kingdom (Table 2). All patients were treated for ISR in the target lesion more than 2 times. Baseline patient characteristics are shown in Table 1.
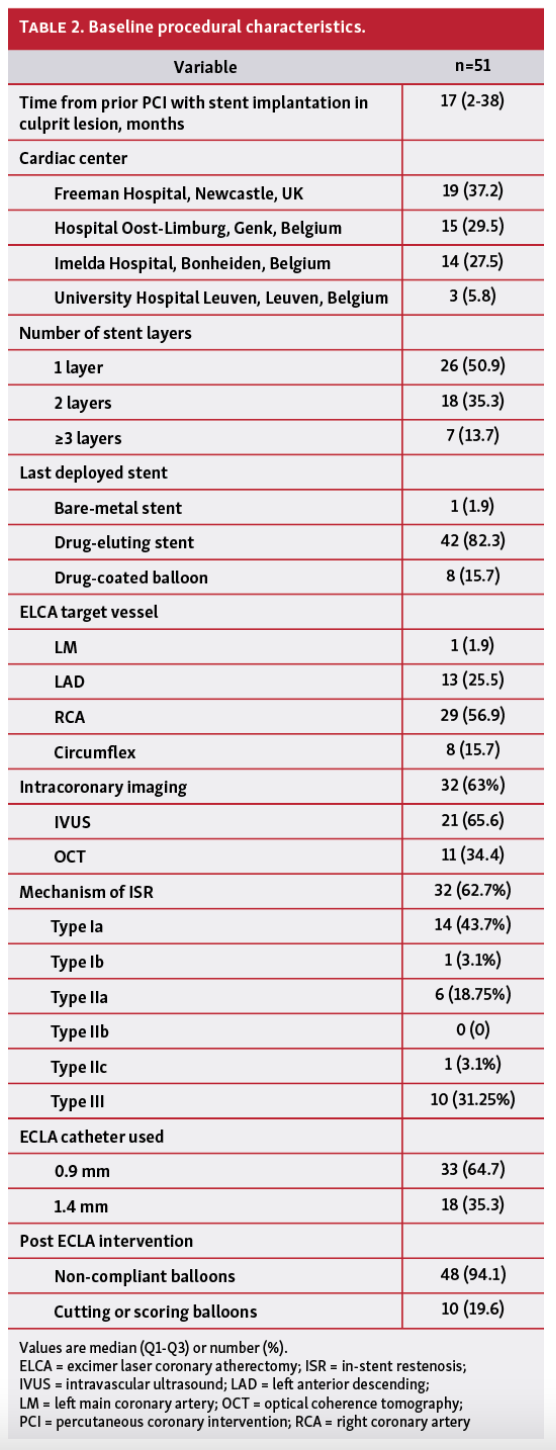
ISR occurred at a median of 17 months (2-38) after the most recent PCI. In 82% of the cases, the last deployed stent was a drug-eluting stent (DES), and in 16%, a DCB. A total of 25 patients fulfilled the criteria for a type V ISR (>2 stent layers).
Intracoronary imaging was used in 51% of the cases (OCT 35%; IVUS 65%) to determine optimal strategy. Most lesions comprised a Type IA (N=14) ISR, followed by a type III (N=10). Neointimal hyperplasia alone (type IIA) was present in 6 cases.
The right coronary artery was the most common target vessel (N=29), followed by the left anterior descending artery (N=13), circumflex artery (N=8), and left main coronary artery (N=1).
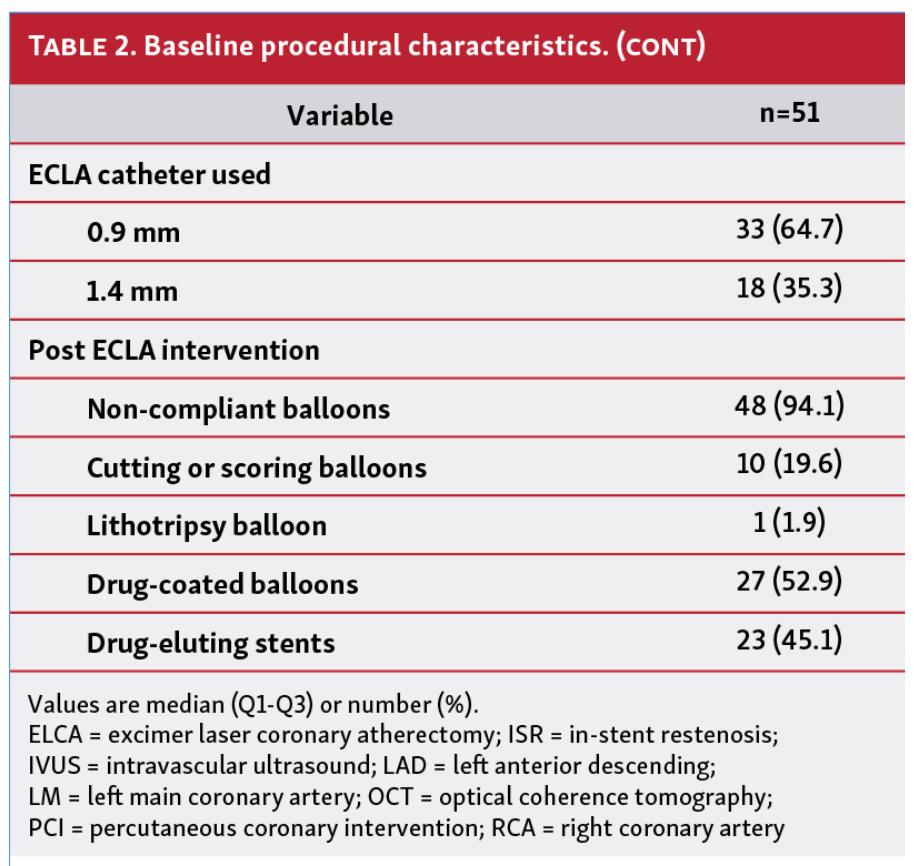
The .9 mm diameter ELCA catheter was used in 33 patients (65%) and the 1.4 mm diameter catheter in 18 patients (35%). In 48 cases (94%), the lesion was additionally treated with a non-compliant balloon. In 10 cases (20%), a cutting and/or scoring balloon was used; in 1 case (2%), a lithotripsy balloon; in 27 cases (53%), a DCB; and in 23 cases (45%), a DES was implanted. In 45 patients (88%), >2 of these treatment options were used during the procedure.
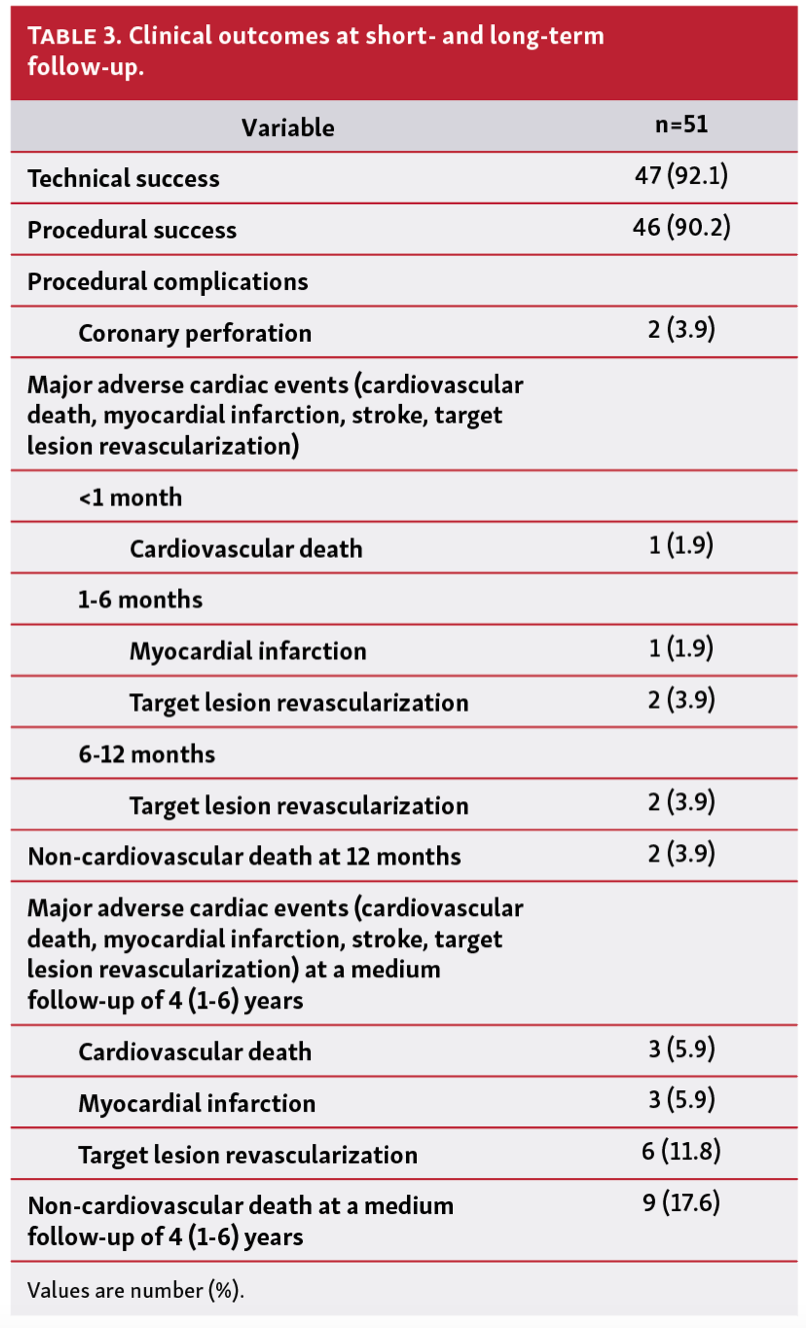
MACE occurred in 6 patients (11.8%) at 12 months and in 12 patients (23.5%) at a median follow-up of 4 (1-6) years (Table 3). Technical and procedural success were achieved in 92% and 90% of cases, respectively. Procedural complications occurred in 2 patients. These included both distal wire perforation with cardiac tamponade requiring emergency pericardiocentesis and coil embolization, respectively. There were no ELCA-related complications and no in-hospital MACE. One patient died of sudden cardiac failure secondary to ischemic cardiomyopathy 3 weeks after the procedure. Two patients died from non-cardiovascular causes (sepsis and cancer) at 12 months and a total of 9 patients (17.6) at a median follow-up of 4 (1-6) years.
Discussion
This multicenter study is the largest to date to examine the long-term clinical outcomes of ELCA for the management of recurrent ISR. The results demonstrate a high technical and procedural success of ELCA in recurrent ISR of around 90%, importantly, with a safe profile. These results match other studies in which ELCA was used for ISR and other indications.10,11 Other previous small registries showed that ELCA may be a reasonable adjunctive therapy for stent underexpansion.12-14 Our study supports the fact that ELCA may be a good adjunctive therapy for not only stent underexpansion, but also the presence of diffuse neointimal hyperplasia.
Excimer laser modifies underlying resistant atheroma without disrupting the stent architecture and changes plaque burden under the stent struts via its photothermal (localized thermal energy), photochemical (breaking molecular bonds), and photomechanical (microbubble formation) properties.7,15,16 Therefore, it enables enlargement of the vessel lumen and further expansion of the existing stent(s) with a NC balloon. ELCA can also be very useful to modify balloon-uncrossable or balloon-undilatable lesions.7 ELCA is typically performed under continuous saline infusion to displace blood or contrast media, which reduces the mechanical trauma to the vessel wall (saline has lower photomechanical effect than blood, and blood has lower photomechanical effect than contrast). However, activation of ELCA in blood or contrast media stimulates the formation of larger bubbles to potentiate its photomechanical action, making it an additional tool to achieve adequate stent expansion in refractory cases.13 Within a stented vessel, ELCA using contrast media appears to be safe, facilitating optimal stent expansion. This technique was initially evaluated in 28 patients in the ELLEMENT registry,12 with procedural success achieved in 27 out of 28 cases (96%), and a low complication rate. This was also demonstrated in 2 other small registries.13,14
In our cohort, 49% of the patients had a type V ISR, of which 14% even had ≥3 stent layers. It is unclear how to treat ISR in the case of multiple stent layers and it remains a technical challenge. It is known that primary stent underexpansion has been associated with an increased risk of secondary stent underexpansion. This has been associated with an increased risk of MACE and ISR recurrence.17,18 Post-procedural stent underexpansion has also been shown to predict recurrence for ISR treated with DCBs.19 Suboptimal treatment of ISR can result in a vicious cycle, especially when patients are treated with an additional DES leading to multiple stent layers (“sandwich strategy”).20 In this cohort, the 2 patients who needed TLR within 6 months both had a type IA ISR and were treated with a scoring/cutting balloon and DCB, respectively. In the 2 patients who needed TLR within 1 year, both had 2 previous stent layers, of which one showed type IA and the other type IIA. They were treated with a DCB and DES, respectively. These data contribute to the fact that underexpansion of stents remains an important problem in the occurrence of ISR.
Intracoronary imaging is critical to identify the mechanism of ISR and tailor therapy accordingly to improve clinical outcomes. An algorithmic approach guided by intracoronary imaging for the treatment of DES-ISR is recommended based on the specific cause of restenosis.3 In our cohort, in 1 patient where intracoronary imaging was used, MACE occurred. The other primary outcome events occurred in patients in whom intracoronary imaging was not used. This might support the importance of guiding PCI with optical coherence tomography/intravascular ultrasound.
Similar to other aggressive atherectomy devices, the use of ELCA during complex PCI may be associated with increased rates of procedural complications, especially coronary perforation, however this does not appear to increase the likelihood of in-hospital mortality or MACE.21 The risk of distal wire perforation in our cases concerned the need for a guidewire with higher tip load for better crossing of the lesion and a more distal wire position for more support to deliver a stent. With improved operator experience and patient selection, ELCA-associated complications can be significantly reduced. In our study, coronary perforation occurred because of distal wire perforation and was not ELCA-associated.
Limitations
This was a retrospective study, and therefore, has inherent limitations of the retrospective design. Additionally, quantitative coronary angiography by an independent core laboratory was not done, which might have introduced performance bias. Moreover, the multicenter design with small sample sizes and operator variance should be taken into consideration when interpreting the results.
Conclusion
ELCA appears to be a safe method with acceptable long-term results for the management of recurrent ISR with a high procedural and technical success and low complication rate.
Affiliations and Disclosures
*Joint first authors.
From 1Cardiothoracic Department, Freeman Hospital, Newcastle upon Tyne, United Kingdom; 2Department of Clinical, Pharmaceutical, and Biological Science, University of Hertfordshire, Hertfordshire, United Kingdom; 3Cardiology Department, Ziekenhuis Oost-Limburg, Genk, Belgium; 4Cardiology Department, Imelda Hospital, Bonheiden, Belgium; 5Cardiology Department, UZ Leuven, Leuven, Belgium; 6Newcastle University Translational and Clinical Research Institute, Newcastle upon Tyne, United Kingdom; 7School of Medicine, University of Sunderland, United Kingdom.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. One or more of the authors have disclosed potential conflicts of interest regarding the content herein (Professor M Egred is a proctor for laser and has received honoraria, proctorship, and speaker’s fee from Phillips).
Manuscript accepted May 11, 2023.
Address for correspondence: Professor Mohaned Egred BSc (Hons) MB ChB MD FRCP FESC, Cardiothoracic Department, Freeman Hospital, Newcastle-Upon-Tyne, Tyne and Wear, NE7 7DN, United Kingdom. Email: m.egred@nhs.net
References
1. Stefanini GG, Alfonso F, Barbato E, et al. Management of myocardial revascularisation failure: an expert consensus document of the EAPCI. EuroIntervention. 2020;16(11):e875-e890. doi: 10.4244/EIJ-D-20-00487
2. Bourantas CV, Zhang YJ, Garg S, et al. Prognostic implications of coronary calcification in patients with obstructive coronary artery disease treated by percutaneous coronary intervention: a patient-level pooled analysis of 7 contemporary stent trials. Heart. 2014;100(15):1158-1164. doi: 10.1136/heartjnl-2013-305180
3. Shlofmitz E, Iantorno M, Waksman R. Restenosis of drug-eluting stents: a new classification system based on disease mechanism to guide treatment and state-of-the-art review. Circ Cardiovasc Interv. 2019;12(8):e007023. doi: 10.1161/CIRCINTERVENTIONS.118.007023
4. Rawlins J, Din JN, Talwar S, et al. Coronary intervention with the excimer laser: review of the technology and outcome data. Interv Cardiol. 2016;11(1):27-32. doi: 10.15420/icr.2016:2:2
5. McQuillan C, Farag M, Egred M. Excimer laser coronary angioplasty: clinical applications and procedural outcome, in a large-volume tertiary center. Cardiology. 2021;146(2):137-143. doi: 10.1159/000513142
6. Egred M, Brilakis ES. Excimer laser coronary angioplasty (ELCA): fundamentals, mechanism of action, and clinical applications. J Invasive Cardiol. 2020;32(2):E27-E35.
7. Tsutsui RS, Sammour Y, Kalra A, et al. Excimer laser atherectomy in percutaneous coronary intervention: a contemporary review. Cardiovasc Revasc Med. 2020;25:75-85. doi: 10.1016/j.carrev.2020.10.016
8. Kuntz RE, Baim DS. Defining coronary restenosis. Newer clinical and angiographic paradigms. Circulation. 1993;88(3):1310-1323. doi: 10.1161/01.cir.88.3.1310
9. Garcia-Garcia HM, McFadden EP, Farb A, et al. Standardized end point definitions for coronary intervention trials: the Academic Research Consortium-2 consensus document. Circulation. 2018;137(24):2635-2650. doi: 10.1161/CIRCULATIONAHA.117.029289
10. Karacsonyi J, Armstrong EJ, Truong HTD, et al. Contemporary use of laser during percutaneous coronary interventions: insights from the Laser Veterans Affairs (LAVA) multicenter registry. J Invasive Cardiol. 2018;30(6):195-201.
11. Mehran R, Mintz GS, Satler LF, et al. Treatment of in-stent restenosis with excimer laser coronary angioplasty: mechanisms and results compared with PTCA alone. Circulation. 1997;96(7):2183-2189. doi: 10.1161/01.cir.96.7.2183
12. Latib A, Takagi K, Chizzola G, et al. Excimer laser lesion modification to expand non-dilatable stents: the ELLEMENT registry. Cardiovasc Revasc Med. 2014;15(1):8-12. doi: 10.1016/j.carrev.2013.10.005
13. Veerasamy M, Gamal AS, Jabbar A, et al. Excimer laser with and without contrast for the management of under-expanded stents. J Invasive Cardiol. 2017;29(11):364-369.
14. Nan J, Joseph TA, Bell MR, et al. Outcomes of excimer laser-contrast angioplasty for stent underexpansion. EuroIntervention. 2021;17(1):78-80. doi: 10.4244/EIJ-D-19-01074
15. Burris N, Lippincott RA, Elfe A, et al. Effects of 308 nanometer excimer laser energy on 316 L stainless-steel stents: implications for laser atherectomy of in-stent restenosis. J Invasive Cardiol. 2000;12(11):555-559.
16. Sunew J, Chandwaney RH, Stein DW, et al. Excimer laser facilitated percutaneous coronary intervention of a nondilatable coronary stent. Catheter Cardiovasc Interv. 2001;53(4):513-517. doi: 10.1002/ccd.1212
17. Fujii K, Mintz GS, Kobayashi Y, et al. Contribution of stent underexpansion to recurrence after sirolimus-eluting stent implantation for in-stent restenosis. Circulation. 2004;109(9):1085-1088. doi: 10.1161/01.CIR.0000121327.67756.19
18. Yin D, Mintz GS, Song L, et al. Collaborators. In-stent restenosis characteristics and repeat stenting underexpansion: insights from optical coherence tomography. EuroIntervention. 2020;16(4):e335-e343. doi: 10.4244/EIJ-D-18-01191
19. Miura K, Tada T, Habara S, et al. Optical coherence tomography predictors for recurrent restenosis after paclitaxel-coated balloon angioplasty for drug-eluting stent restenosis. Circ J. 2018;82(11):2820-2828. doi: 10.1253/circj.CJ-18-0464
20. Alfonso F, Coughlan JJ, Giacoppo D, et al. Management of in-stent restenosis. EuroIntervention. 2022;18(2):e103-e123. doi: 10.4244/EIJ-D-21-01034
21. Protty MB, Hussain HI, Gallagher S, et al. Excimer laser coronary atherectomy during complex PCI: An analysis of 1,471 laser cases from the British Cardiovascular Intervention Society database. Catheter Cardiovasc Interv. 2021;97(5):E653-E660. doi: 10.1002/ccd.29251
Related Reading
Excimer Laser Coronary Angioplasty (ELCA): Fundamentals, Mechanism of Action, and Clinical Applications
Histopathologic Characterization of Chronic Total Occlusions by Directional Atherectomy: The HIPACT Study
Coronary Perforation After Excimer Laser Coronary Angioplasty at a Calcium Nodule
Clinical Performance of a Paclitaxel Drug-Coated Balloon in Real-World Percutaneous Coronary Intervention Practice: The PEARL Registry
Unstable Angina Induced by Fracture of a Recently Implanted Drug-Eluting Stent
Paclitaxel Drug-Coated Balloon for the Treatment of De Novo Small-Vessel and Restenotic Coronary Artery Lesions: 12-Month Results of the Prospective, Multicenter, Single-Arm PREVAIL Study













