

Non-ST Elevation Myocardial Infarction With Occluded Culprit Artery: A Continuum of Mortality Risk Across the Spectrum of Acute Myocardial Infarction
Abstract
Background. Non-ST segment elevation myocardial infarction (NSTEMI) patients presenting with occluded culprit artery (OCA) may be at higher risk for worse outcomes. We sought to compare in-hospital (IH) mortality between patients presenting with NSTEMI with and without OCA, and ST-segment elevation myocardial infarction (STEMI). Methods. This retrospective analysis studied 14,037 patients enrolled in the Portuguese National Registry of Acute Coronary Syndromes. Three groups were defined: (A) STEMI (n = 8616); (B) OCA-NSTEMI (n = 1309); and (C) non-OCA NSTEMI (n = 4112). Baseline characteristics, therapeutic strategies, and outcomes were compared. Multivariate analysis was performed to assess the risk of IH all-cause mortality across the prespecified groups. Results. Twenty-four percent of NSTEMI patients presented with OCA. The left circumflex artery was more frequently the culprit artery in group B (12.4% A vs 34.5% B vs 26.0% C; P<.001) and this group was also less likely to receive percutaneous revascularization (95.2% A vs 69.7% B vs 83.2% C; P<.001). The incidence of left ventricular systolic dysfunction was higher in group A and lower in group C (19.9% A vs 12.2% B vs 8.1% C; P<.001). The adjusted risk of IH mortality was significantly higher in group A when compared with group B (3.9% A vs 1.8% B; odds ratio, 2.34; 95% confidence interval, 1.34-4.07; P<.01) and in group B when compared with group C (1.8% B vs 0.9% C; odds ratio, 2.25; 95% confidence interval, 1.17-4.35; P=.02). Conclusion. OCA-NSTEMI patients had worse IH outcomes than non-OCA NSTEMI patients and better IH outcomes than STEMI patients, suggesting the existence of a continuum of increased risk of IH mortality across these groups.
J INVASIVE CARDIOL 2021;33(12):E931-E938. Epub 2021 November 3.
Key words: myocardial infarction, occluded culprit artery, prognosis
Introduction
Patients with non-ST segment elevation myocardial infarction (NSTEMI) represent a heterogeneous group regarding clinical characteristics, coronary anatomy, and in-hospital (IH) management.1 According to different series, up to 44.4% may present with occluded culprit artery (OCA)2,3 and there is some evidence that this subgroup may develop worse prognosis than non-OCA (nOCA) NSTEMI patients,4,5 highlighting the potential benefits of the early recognition of OCA in NSTEMI patients.
Although STEMI and NSTEMI patients share the same risk factors, pathogenesis, complications, and prognosis,6 the relative insensitivity of surface 12-lead electrocardiogram (ECG) to identify acute left circumflex coronary artery (LCX) occlusion may be one possible factor to elucidate why some patients admitted with the diagnosis of NSTEMI, instead of STEMI, may present with OCA.7,8
Considering the evidence suggesting worse outcomes in NSTEMI patients presenting with OCA vs nOCA and the lack of studies comparing OCA-NSTEMI and STEMI outcomes, we sought to ascertain how much the presence of OCA in NSTEMI patients influences IH mortality in relation to nOCA-NSTEMI and STEMI patients.
Methods
Study population and design. The Portuguese National Registry of Acute Coronary Syndromes (ProACS, current version of study NCT01642329 on www.ClinicalTrials.gov), conducted by the Portuguese Society of Cardiology, is an ongoing observational and nationwide registry involving 49 hospital centers enrolling patients admitted due to acute coronary syndromes (ACS).9 This prospective registry includes consecutive patients and collects important data during hospitalization, including demographic, clinical and patient management-related characteristics.
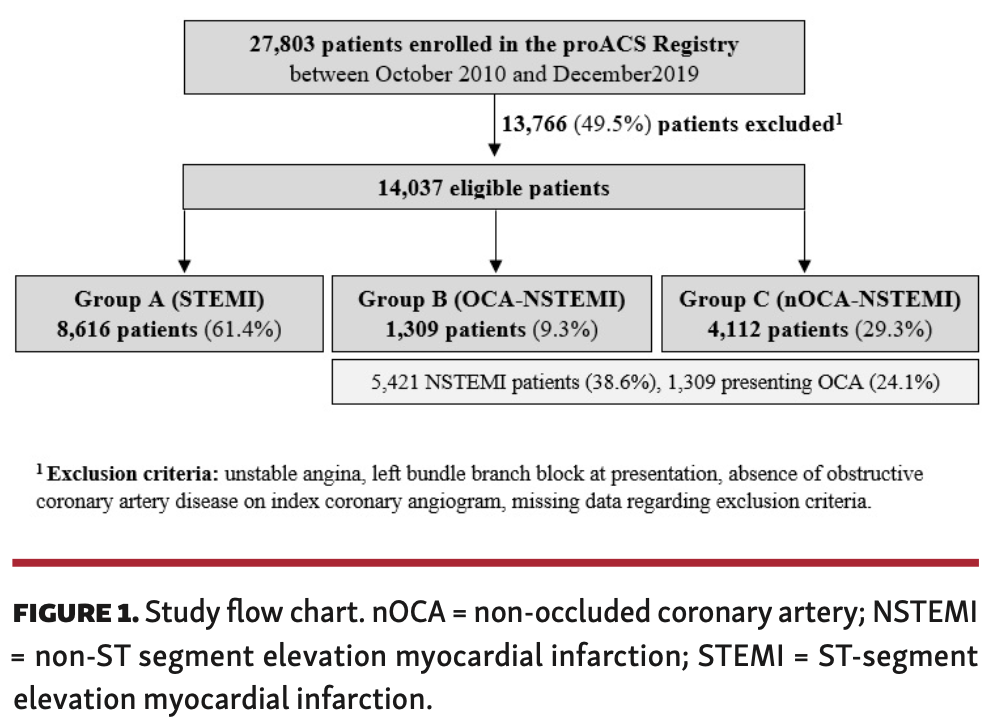
For the current study, we included a cohort of 27,803 patients enrolled in between October 2010 and December 2019. The major criteria for inclusion were: patients aged >18 years old and unequivocal diagnosis of acute myocardial infarction (MI), according to the contemporary guidelines,1,10 who underwent coronary angiography during index hospitalization. Patients with unstable angina, showing left bundle-branch block (LBBB), not presenting obstructive coronary artery disease (CAD) on coronary angiogram, and those with missing data regarding these variables were excluded. Following the application of these criteria, 14,037 patients were eligible for the final analysis. Three groups were considered according to baseline diagnosis and coronary angiography findings: group A, STEMI (n = 8616; 61.4%); group B, OCA-NSTEMI (n = 1309; 9.3%); and group C, nOCA-NSTEMI (n = 4112; 29.3%) (Figure 1).
Obstructive CAD was defined according to the presence of at least 1 major coronary artery with a ≥50% stenosis on the index coronary angiogram; multivessel CAD was considered whenever ≥2 major coronary arteries were involved. Baseline Thrombolysis in Myocardial Infarction (TIMI) flow grade 0/1 in the culprit artery defined the presence of OCA. The culprit vessel of patients with NSTEMI was identified based on the findings of coronary angiography, 12-lead electrocardiogram (ECG), and 2-dimensional echocardiogram. Percutaneous coronary intervention (PCI) was performed, when appropriate, given angiographic, ECG, and clinical data. Left ventricular systolic dysfunction (LVSD) required the documentation of left ventricular ejection fraction (LVEF) <40%, a definition in accordance with the most recent European recommendations.11 LVEF was determined by 2-dimensional echocardiography (biplane Simpson’s method) before discharge. We defined the primary endpoint as IH all-cause mortality. The study complied with the Declaration of Helsinki.
Statistical analysis. Baseline demographic and clinical characteristics, angiographic findings, therapeutic strategies, LVEF, and outcomes were analyzed. Variables are expressed as mean ± standard deviation, median and interquartile range (IQR), or counts and percentages (%), as appropriate. Normality of continuous variables was assessed by histogram observation and the Shapiro-Wilk test. For continuous variables, paired Student’s t-test or non-parametric Mann-Whitney tests were used for comparisons between 2 groups (A vs B and B vs C), as appropriate, and the non-parametric Kruskal Wallis test was used to compare the 3 groups; the Chi-squared test (or Fisher’s exact test, as appropriate) was used for categorical variables. The level of significance was adjusted at P<.025 (.05/2) using the Bonferroni correction method for paired comparisons; significance was set at P<.05 for the remaining analysis.
The risk of IH mortality was compared between paired groups using logistic regression analysis to produce odds ratios (ORs) and corresponding 95% confidence intervals (CIs) adjusted for predefined characteristics. All variables with P-values <.05 were entered into the model (age, gender, cardiovascular risk factors, history of MI, PCI, coronary artery bypass grafting [CABG], peripheral artery disease, stroke as well as Killip-Kimball class, cardiac arrest as presentation, right bundle-branch block [RBBB], GRACE score, heart rate, blood pressure, PCI during index hospitalization, and LVEF). The software used for statistical analyses was IBM SPSS Statistics, version 19.0 (IBM Corporation).
Results
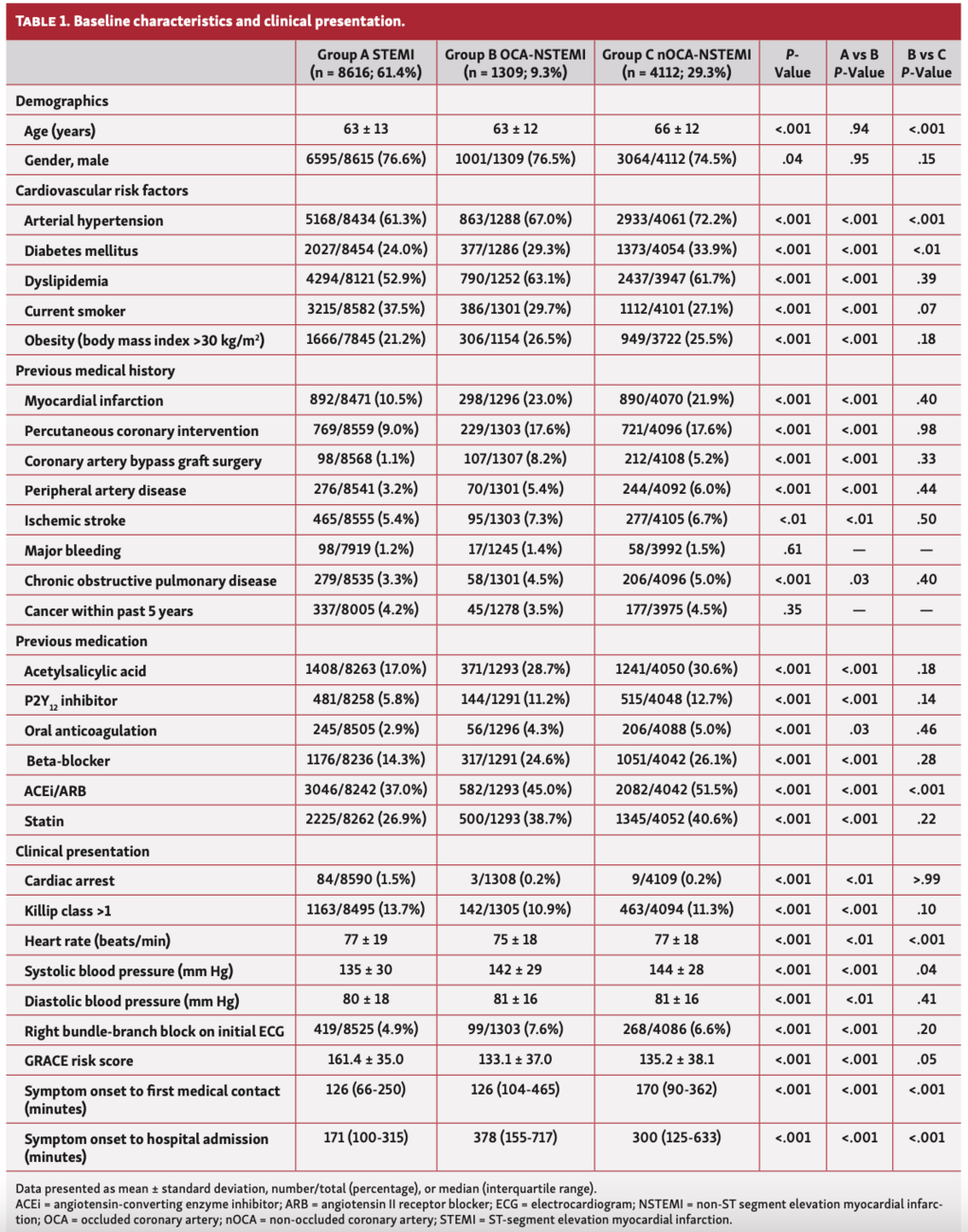
Baseline characteristics and clinical presentation (Table 1). Mean age was 64 ± 13 years, with no differences between groups A and B, while group B patients were younger than group C patients. Overall, 76.6% of patients were male, with no differences regarding paired comparisons. Group A had lower cardiovascular risk factor (CVRF) burden (arterial hypertension, diabetes, dyslipidemia, obesity) than group B, despite including more smokers. Group C had higher rates of arterial hypertension and diabetes mellitus than group B, with no differences regarding the remaining CVRF. In comparison with group A, group B had more frequent previous MI, PCI, CABG, ischemic stroke, and peripheral artery disease diagnoses. On the contrary, no differences were registered between groups B and C regarding these variables. Accordingly, antiplatelet drugs (acetylsalicylic acid and P2Y12 inhibitors), beta-blockers, angiotensin-converting enzyme inhibitors/angiotensin-II receptor blockers, and statins were more frequently prescribed to group B than group A. No major differences were found among groups B and C regarding previous medication.
Group A presented more frequently at admission with cardiac arrest, Killip-Kimball class >1, and higher CRUSADE score when compared with group B, with no differences between groups B and C. RBBB on 12-lead ECG was more common in group B than in group A, with no differences between groups B and C (P=.20). Time from symptom onset to first medical contact (FMC) and to hospital admission was significantly lower in group A compared with group B.
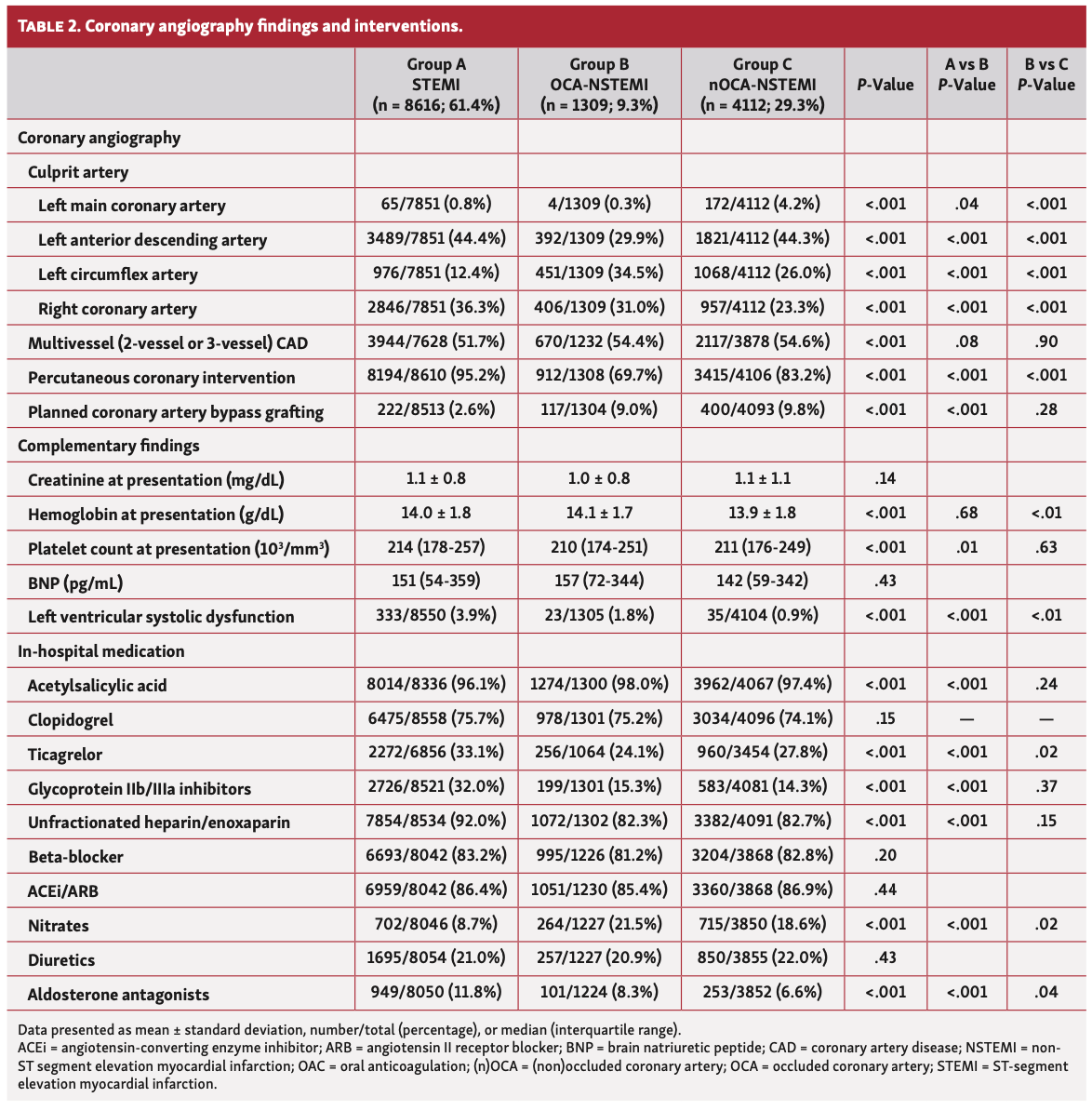
Coronary angiography findings and interventions (Table 2). The incidence of multivessel CAD did not differ in both paired comparisons. An OCA was found in 24.1% of the patients presenting with NSTEMI (n = 1309/5421). Regarding culprit artery distribution, the LCX was more frequently involved in group B than in groups A and C (12.4% A vs 34.5% B [P<.001] and 34.5% B vs 26.0% C; [P<.001]), the left anterior descending artery (LAD) was the culprit most frequently in groups A and C compared with group B (44.4% A vs 29.9% B [P<.001] and 29.9% B vs 44.3% C [P<.001]), and the right coronary artery more frequently in group A and less frequently in group C compared with group B (36.3% A vs 31.0% B [P<.001] and 31.0% B vs 23.3% C [P<.001]). PCI was less likely to be performed in group B compared with both groups A and C (95.2% A vs 69.7% B [P<.001] and 69.7% B vs 83.2% C [P<.001]), while CABG was equally performed in groups B and C. Group B presented lower incidence of LVSD than group A (19.9% A vs 12.2% B; P<.001) and higher incidence than group C (12.2% B vs 8.1% C; P<.001).
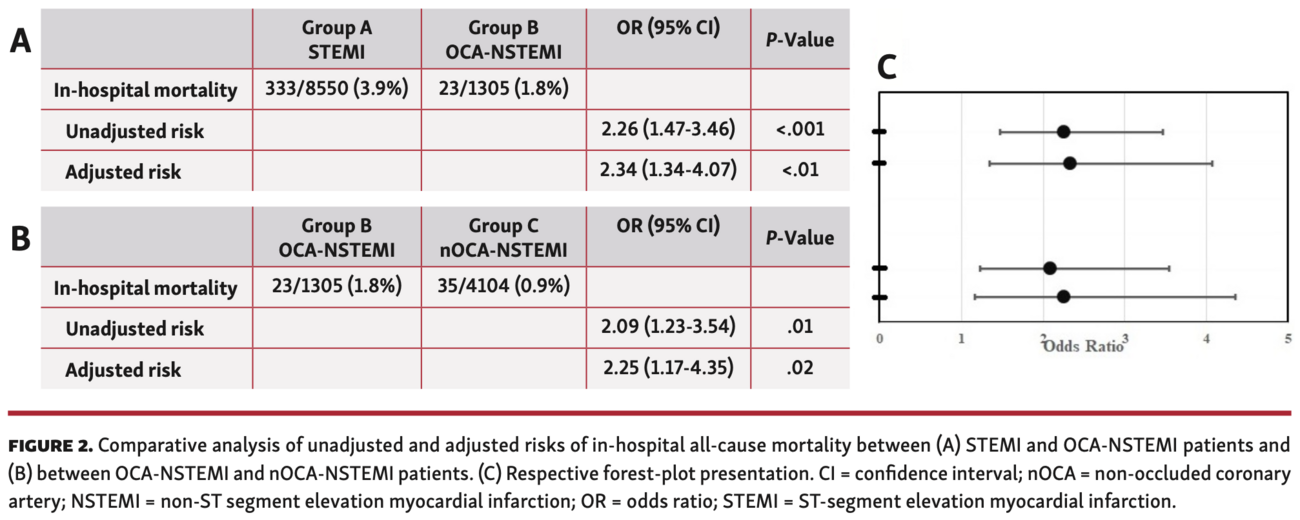
Primary endpoint. Overall, there were 391 IH deaths (2.8%). Unadjusted IH all-cause mortality was higher in the STEMI cohort in comparison with the OCA-NSTEMI group (OR, 2.26; 95% CI, 1.47-3.46; P<.001) and higher in the OCA-NSTEMI cohort than in the nOCA-NSTEMI cohort (OR, 2.09; 95% CI, 1.23-3.54; P<.01). After adjustment for known confounders, the primary endpoint rates remained higher among STEMI patients when compared with OCA-NSTEMI patients (OR, 2.34; 95% CI, 1.34-4.07; P<.01) and higher in the OCA-NSTEMI cohort than in the nOCA-NSTEMI group (OR, 2.25; 95% CI, 1.17-4.35; P=.02) (Figure 2).
Discussion
The main findings of this analysis of 3 prespecified groups in a relatively large cohort of patients with acute MI undergoing coronary angiogram are: (1) the prevalence of CVRF and previous cardiovascular events, as well as clinical presentation, differed across the 3 groups; (2) OCA was observed in 24% of the NSTEMI population, with the LCX being considered the “culprit” artery more frequently, and these patients were also less likely to undergo PCI; and (3) an increasing gradient of IH mortality was observed across the 3 groups, with the STEMI group having the worst outcomes, the nOCA-NSTEMI patients having the best outcomes, and the OCA-NSTEMI patients in the middle ground regarding short-term survival.
Atherosclerotic CAD is a leading cause of death and morbidity worldwide,12 having well-recognized risk factors, such as dyslipidemia, hypertension, and diabetes.13 Classically, and regardless of clinical presentation, the pathophysiological hallmark of type 1 MI is the development of atherosclerotic plaque rupture, ulceration, fissure, or erosion, with resulting intraluminal thrombus in 1 or more coronary arteries leading to decreased myocardial blood flow and/or distal embolization and subsequent myocardial necrosis.1,14 In our study, when compared with the STEMI group, OCA-NSTEMI patients presented with higher CVRF burden (except current smoking, otherwise more frequent among the former) and previous cardiovascular event rate, as well as less-severe clinical features at admission (eg, Killip class, GRACE score). These distinct clinical profiles have been previously observed not only in studies comparing STEMI with unselected NSTEMI patients,6,15,16 but also in a subanalysis of the occluded artery trial (OAT) comparing STEMI and OCA-NSTEMI patients.7 On the other hand, baseline characteristics and clinical presentation did not differ between NSTEMI patients with and without OCA, with few exceptions (such as older age in the latter), which replicates the findings from previous studies.4,17,18
Acute MI is classified according to the ST segment in the 12-lead ECG as STEMI or NSTEMI. This distinction is important and must be immediately established (within 10 minutes after FMC), since the presence of ST-segment elevation generally reflects an acute total or subtotal coronary occlusion causing transmural ischemia and these cases are the ones that mostly benefit from immediate reperfusion strategies.1,19 However, OCA can also be observed in a significant proportion of patients (19.9%-44.4%) initially diagnosed with NSTEMI,2,3,18 whose immediate reperfusion may be denied or delayed.2,19 Accordingly, in our study, OCA was observed in about one-quarter of the NSTEMI population. It is speculated that acute total occlusion of territories with dual blood supply and of vessels with well-developed collaterals or small infarction areas may explain some of these cases.4,20 However, the most relevant cause is attributed to the imperfect sensitivity of the “conventional” 12-lead ECG to detect acute inferolateral or posterolateral coronary circulation involvement, when the LCX is usually the culprit artery,4,17,21,22 contrary to the easily recognizable anterior and inferior circulation involvement.22 In fact, among our OCA-NSTEMI population, the culprit artery was more frequently the LCX (and less frequently the LAD) in comparison with the STEMI and nOCA-NSTEMI cohorts, which was also observed in several similar studies.3-5,7,21 It is also important to note that, compared with STEMI patients, the OCA-NSTEMI group presented more frequently with RBBB, a finding that may hamper the detection of transmural ischemia in patients presenting with chest pain and that usually denotes worse prognosis.19 According to current guidelines, patients presenting with chest pain plus RBBB or with recurrent/refractory chest pain despite absence of ST elevation should be managed as “STEMI-like” cases, since they are expected to benefit from emergent invasive strategy (<2 hours).1,19 However, in our study, OCA-NSTEMI patients presented with greater management delays, which might have contributed to the fact that they were less likely to receive PCI than both STEMI and nOCA-NSTEMI patients. To overcome the potential consequences of 12-lead ECG insensitivity, additional chest leads (V7-V9) may be used to better identify lateral- and/or posterior-wall MI. This is especially relevant whenever patients present with symptoms of ongoing ischemia and/or ST-segment depression in leads V1-V3, and transthoracic echocardiography should also be considered in these cases of high suspicion of LCX occlusion.19 In addition, multilead systems have been suggested to improve ST elevation detection in cases of acute MI and LCX-OCA, which may result in earlier diagnosis and reperfusion.23
Several contemporary observational studies suggest that IH mortality is generally higher in STEMI patients than in unselected NSTEMI populations;24-26 however, studies comparing IH death between STEMI and OCA-NSTEMI patients are scarce. Besides, the prognostic significance of OCA among patients presenting with NSTEMI is somewhat conflicting across the literature.3-5,18,27 In our study, IH all-cause death was relatively low and demonstrated a two-fold sequential increase across the 3 groups, with nOCA-NSTEMI patients presenting the lowest risk and STEMI patients the highest. Moreover, in our analysis, this gradient of IH mortality risk remains after adjustment for measured confounders, providing valuable information regarding IH outcomes in our 3 prespecified populations. On one hand, our results reproduce those from several studies reporting a negative impact of OCA on IH mortality among NSTEMI cohorts4,5,27 and by a meta-analysis of 41,077 NSTEMI patients that showed an association between OCA and worse short-term (IH or 30-day) all-cause mortality.2 This is particularly relevant taking into account the large number of NSTEMI patients (5421) included in our analysis, in comparison with similar studies systematically reviewed by Hung et al in 2018.20 We hypothesize that the worse outcome among OCA-NSTEMI patients might have been mainly driven by management delays leading to longer duration of myocardial ischemia and/or to lower rates of delivered PCI. Altogether, this may have contributed to the higher rates of LVSD in this group, which is typically associated with early mortality following ACS.28
On the other hand, OCA-NSTEMI patients still had lower rates of IH mortality compared with the STEMI cohort. Although the times from symptom onset to FMC and to hospital admission were far shorter in STEMI patients, who were also more likely to receive PCI, they developed LVSD more frequently than OCA-NSTEMI patients and we speculate that this may explain the worse outcomes. In this regard, comparing the 2 groups according to the distribution of the culprit artery, it is important to highlight that the LAD and the RCA were more frequently involved in the STEMI cohort, whereas the OCA-NSTEMI group predominantly presented with LCX occlusion. As the LAD supplies 40%-50% of the left ventricular myocardium (more than the LCX and the RCA if non-dominant), anterior infarcts are usually larger22 and have been previously associated with higher mortality.4 In fact, a contemporary study by Karwowski et al3 including 4581 STEMI patients showed that in patients with anterior MI, LAD total occlusion was associated with higher incidence of LVSD when compared with cases without total occlusion, and was an independent predictor of 1-month and 36-month mortality. Moreover, our results resemble those reported by Stribling et al29 in a study including 56 patients in which NSTEMI patients with occluded LCX were significantly less likely to die during hospitalization than STEMI patients. The authors hypothesize that this may be justified by the higher prevalence of left or mixed coronary dominance within the STEMI cohort.
According to our results and the most relevant evidence available, we favor the hypothesis previously raised by Stribling et al22 that OCA-NSTEMI patients constitute a group of intermediate risk, with underlying larger infarcts and worse IH outcomes than nOCA-NSTEMI patients, but smaller infarcts and better IH outcome than STEMI patients. Given this continuum of mortality risk, patients presenting with ischemic symptoms and absence of ST elevation or isolated precordial ST-segment depression on the 12-lead ECG must undergo additional investigation (including posterior ECG leads and echocardiography) to assess eventual signs of transmural ischemia secondary to total coronary occlusion, especially within the territory of the LCX. Accordingly, those with evidence of ST elevation on additional leads, RBBB, and/or high-risk features (such as recurrent/refractory ischemic symptoms or hemodynamic instability) likely resemble the STEMI risk profile and benefit from emergent invasive strategy, while those without significant ECG changes or ongoing symptoms likely resemble the NSTEMI risk profile and may be managed more conservatively.
Study limitations. The present study is subject to some intrinsic limitations associated with its retrospective, observational nature, from which causal inferences cannot be drawn. In fact, given that physician utilization of the ProACS registry is on a voluntary basis, our data may not be as representative as a population-based sample and there is also room for missing data, leading to some bias. One major limitation specifically inherent to our study was that culprit lesion locations were determined by treating cardiologists without central adjudication and may be subject to bias, particularly among the NSTEMI group; however, this bias should be equally distributed between OCA and nOCA groups. Additionally, we excluded patients without obstructive CAD from the analysis to minimize the potential bias of including patients with MI with non-obstructive CAD, a condition usually associated with better prognosis.30,31 Another important limitation was the relatively low IH mortality rate registered (2.8%), which may also lead to bias; yet, this rate was comparable to the 2.7% reported in a contemporary French registry.32 Although we attempted to adjust for multiple measured potential confounders, it is not possible to exclude confounding by unmeasured variables. Indeed, the exact times from symptom onset and FMC to wire passage were important variables that we could not obtain for the NSTEMI patients since the registry is designed to only keep track of these values for patients undergoing primary PCI. However, significant delays for this population can be inferred given the information available regarding times from symptom onset and FMC to hospital admission.
Conclusion
In our population, OCA was found in about one-quarter of the NSTEMI patients and the LCX was considered the culprit artery more frequently in this subgroup compared with the STEMI and nOCA-NSTEMI cohorts. Our study showed that OCA-NSTEMI patients presented with larger infarcts and higher IH mortality than nOCA-NSTEMI patients as well as smaller infarcts and lower IH mortality than STEMI patients, suggesting a continuum of increasing risk across these 3 prespecified populations. Thus, additional efforts (eg, additional chest leads, bedside echocardiogram) should be made to screen patients with ongoing ischemic symptoms and no initial ST elevation who may eventually benefit from emergent invasive strategy due to potential OCA existence. However, the authors hope to see these results replicated in similar ACS registries/large-scale studies, since this was the first to directly compare the IH outcomes of these 3 acute MI groups in the same analysis.
Affiliations and Disclosures
From the 1Department of Cardiology, Leiria Hospital Centre, Leiria, Portugal; and 2National Centre for Data Collection in Cardiology, Portuguese Society of Cardiology, Coimbra, Portugal.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. Dr Morais reports honoraria for lectures from Amgen, Astra Zeneca, Bayer, Bial, Boehringer Ingelheim, Merck Sharp & Dhome, Novartis, and Servier; honoraria for advisory activities from Astra Zeneca, Bayer, Bial, and Novartis. The remaining authors report no conflicts of interest regarding the content herein.
Manuscript accepted January 27, 2021.
Address for correspondence: Luís Graça Santos, MD, Leiria Hospital Centre – Rua de Santo André, 2410-197, Leiria, Portugal. Email: luismscp1@gmail.com
Related Articles
- Vascular Complications of Percutaneous Coronary Intervention Via Distal Radial Artery Approach in Patients With Acute Myocardial Infarction With and Without ST-Segment Elevation
- Safety of Same-Day Discharge After Percutaneous Coronary Intervention in Selected Patients With Non-ST Elevation Acute Coronary Syndrome
- Prehospital Prasugrel Versus Ticagrelor in Real-World Patients With ST-Elevation Myocardial Infarction Referred for Primary PCI: Procedural and 30-Day Outcomes
- Importance of Right Marginal Branch Protection During Primary Angioplasty in Inferior ST-Elevation Myocardial Infarction With Right Ventricular Involvement
References
1. Collet JP, Thiele H, Barbato E, et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur Heart J. 2021;42:1289-1367.
2. Khan AR, Golwala H, Tripathi A, et al. Impact of total occlusion of culprit artery in acute non-ST elevation myocardial infarction: a systematic review and meta-analysis. Eur Heart J. 2017;38:3082-3089.
3. Karwowski J, Gierlotka M, Gąsior M, et al. Relationship between infarct artery location, acute total coronary occlusion, and mortality in STEMI and NSTEMI patients. Pol Arch Intern Med. 2017;127:401-411.
4. Wang TY, Zhang M, Fu Y, et al. Incidence, distribution, and prognostic impact of occluded culprit arteries among patients with non–ST-elevation acute coronary syndromes undergoing diagnostic angiography. Am Heart J. 2009;157:716-723.
5. Kim MC, Ahn Y, Rhew SH, et al. Impact of total occlusion of an infarct-related artery on long-term mortality in acute non-ST-elevation myocardial infarction patients who underwent early percutaneous coronary intervention. Int Heart J. 2012;53:160-164.
6. Montalescot G, Dallongeville J, Van Belle E, et al. STEMI and NSTEMI: are they so different? 1 year outcomes in acute myocardial infarction as defined by the ESC/ACC definition (the OPERA registry). Eur Heart J. 2006;28:1409-1417.
7. Menon V, Ruzyllo W, Carvalho AC, et al. Infarct artery distribution and clinical outcomes in occluded artery trial subjects presenting with non–ST-segment elevation myocardial infarction (from the long-term follow-up of occluded artery trial [OAT]). Am J Cardiol. 2013;111:930-935.
8. Rasoul S, de Boer MJ, Suryapranata H, et al. Circumflex artery-related acute myocardial infarction: limited ECG abnormalities but poor outcome. Neth Heart J. 2007;15:286-290.
9. Timóteo AT, Mimoso J. Registo Nacional de Síndromes Coronárias Agudas: 15 anos de um registo prospetivo contínuo. Rev Port Cardiol. 2018;37:563-573.
10. Thygesen K, Alpert JS, Jaffe AS, et al. Fourth universal definition of myocardial infarction (2018). Eur Heart J. 2019;40:237-269.
11. Ponikowski P, Voors AA, Anker SD, et al. 2016 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure: the task force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J. 2016;37:2129-2200.
12. Weber C, Noels H. Atherosclerosis: current pathogenesis and therapeutic options. Nat Med. 2011;17:1410-1422.
13. Lloyd-Jones DM, Morris PB, Ballantyne CM, et al. 2017 focused update of the 2016 ACC expert consensus decision pathway on the role of non-statin therapies for LDL-cholesterol lowering in the management of atherosclerotic cardiovascular disease risk. J Am Coll Cardiol. 2017;70:1785-1822.
14. Bentzon JF, Otsuka F, Virmani R, Falk E. Mechanisms of plaque formation and rupture. Circ Res. 2014;114:1852-1866.
15. McManus DD, Gore J, Yarzebski J, et al. Recent trends in the incidence, treatment, and outcomes of patients with STEMI and NSTEMI. Am J Med. 2011;124:40-47.
16. Polonski L, Gasior M, Gierlotka M, et al. A comparison of ST elevation versus non-ST elevation myocardial infarction outcomes in a large registry database. Int J Cardiol. 2011;152:70-77.
17. Bahrmann P, Rach J, Desch S, et al. Incidence and distribution of occluded culprit arteries and impact of coronary collaterals on outcome in patients with non-ST-segment elevation myocardial infarction and early invasive treatment strategy. Clin Res Cardiol. 2011;100:457-467.
18. Warren J, Mehran R, Yu J, et al. Incidence and impact of totally occluded culprit coronary arteries in patients presenting with non-ST segment elevation myocardial infarction. Am J Cardiol. 2015;115:428-433.
19. Ibanez B, James S, Agewall S, et al. 2017 ESC guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: the task force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J. 2017;39:119-177.
20. Hung CS, Chen YH, Huang CC, et al. Prevalence and outcome of patients with non-ST segment elevation myocardial infarction with occluded “culprit” artery — a systemic review and meta-analysis. Crit Care. 2018;22:34.
21. From AM, Best PJM, Lennon RJ, et al. Acute myocardial infarction due to left circumflex artery occlusion and significance of ST-segment elevation. Am J Cardiol. 2010;106:1081-1085.
22. Stribling WK, Kontos MC, Abbate A, et al. Left circumflex occlusion in acute myocardial infarction (from the National Cardiovascular Data Registry). Am J Cardiol. 2011;108:959-963.
23. Daly MJ, Scott PJ, Harbinson MT, Adgey JA. Improving the diagnosis of culprit left circumflex occlusion with acute myocardial infarction in patients with a nondiagnostic 12‐lead ECG at presentation: a retrospective cohort study. J Am Heart Assoc. 2019;8;e011029.
24. Miyachi H, Takagi A, Miyauchi K, et al. Current characteristics and management of ST elevation and non-ST elevation myocardial infarction in the Tokyo metropolitan area: from the Tokyo CCU network registered cohort. Heart Vessels. 2016;31:1740-1751.
25. Neumann JT, Goßling A, Sörensen NA, et al. Temporal trends in incidence and outcome of acute coronary syndrome. Clin Res Cardiol. 2020;109:1186-1192.
26. Borrayo-Sánchez G, Rosas-Peralta M, Ramírez-Arias E, et al. STEMI and NSTEMI: real-world study in Mexico (RENASCA). Arch Med Res. 2018;49:609-619.
27. Dixon WC, Wang TY, Dai D. Anatomic distribution of the dulprit lesion in patients with non–ST-segment elevation myocardial infarction undergoing percutaneous coronary intervention. J Am Coll Cardiol. 2008;52:1347-1348.
28. Brezinov OP, Klempfner R, Zekry SB, et al. Prognostic value of ejection fraction in patients admitted with acute coronary syndrome: a real world study. Medicine (Baltimore). 2017;96:e6226.
29. Stribling WK, Kontos MC, Abbate A, et al. Clinical outcomes in patients with acute left circumflex/obtuse marginal occlusion presenting with myocardial infarction. J Interv Cardiol. 2011;24:27-33.
30. Pelliccia F, Pasceri V, Niccoli G, et al. Predictors of mortality in myocardial infarction and nonobstructed coronary arteries: a systematic review and meta-regression. Am J Med. 2020;133:73-83.e4.
31. Sá FM, Ruivo C, Santos LG, et al. Myocardial infarction with nonobstructive coronary arteries: a single-center retrospective study. Coron Artery Dis. 2018;29:511-515.
32. Belle L, Cayla G, Cottin Y, et al. French registry on acute ST-elevation and non-ST-elevation myocardial infarction 2015 (FAST-MI 2015). Design and baseline data. Arch Cardiovasc Dis. 2017;110:366-378.














{kind=link}
{kind=link}
{kind=link}
{kind=link}