

Outcomes of Patients With Acute Coronary Syndromes Undergoing Chronic Total Occlusion Percutaneous Coronary Intervention
Abstract
Background. The prevalence and outcomes of patients who presented with an acute coronary syndrome (ACS) and underwent chronic total occlusion (CTO) percutaneous coronary intervention (PCI) have received limited study. Methods. We examined the clinical characteristics and procedural outcomes of ACS patients who underwent CTO-PCI in the Prospective Global Registry for the Study of CTO Intervention (PROGRESS-CTO; NCT02061436). Results. Of the 8826 patients who underwent CTO-PCI between 2012 and 2022 at 38 centers, 558 (6.3%) presented with ACS. ACS presentation was with non-ST-segment elevation myocardial infarction (MI) in 54%, unstable angina in 33%, and ST-segment elevation MI in 6.5%. ACS patients were older (66 ± 11 years vs 64 ± 10 years; P<.001) and had higher prevalence of comorbidities such as diabetes mellitus (48% vs 42%; P=.02), prior MI (52% vs 45%; P<.01), and lower left ventricular ejection fraction (49 ± 14% vs 51 ± 13%; P<.01). While the PROGRESS-CTO score (1.4 ± 1.0 vs 1.2 ± 1.0; P<.001) was higher in the ACS group, the J-CTO score was comparable (2.3 ± 1.2 vs 2.4 ± 1.3; P=.68). Technical success (88% vs 86%; P=.12) and the incidence of in-hospital major adverse cardiovascular event (MACE) (0.9% vs 2.1%; P=.06) and adverse events at 3-month follow-up (3.4% vs 7.2%; Kaplan-Meier log-rank P=.16) were similar between ACS and non-ACS patients, respectively. Conclusion. Approximately 6% of patients who underwent CTO-PCI presented with an ACS. Technical success, in-hospital MACE, and the incidence of adverse events up to 3 months were similar between patients who presented with vs without an ACS.
Keywords: acute coronary syndrome, chronic total occlusion, indication, percutaneous coronary intervention
Most patients who undergo chronic total occlusion (CTO) percutaneous coronary intervention (PCI) present with “stable” chronic coronary artery disease.1 Occasionally, CTO-PCI may be needed in patients presenting with an acute coronary syndrome (ACS); for example, in patients presenting with saphenous vein graft failure in whom the graft cannot be recanalized2 or in patients who present with ST-segment elevation acute myocardial infarction (STEMI) and have multivessel coronary artery disease (CAD).
The frequency and outcomes of ACS patients who undergo CTO-PCI have received limited study. We examined the prevalence, treatment strategies, and outcomes of patients who presented with ACS, had a CTO as a non-culprit lesion, and underwent CTO-PCI in a large, international multicenter registry.
Methods
We examined the Prospective Global Registry for the Study of Chronic Total Occlusion Intervention (PROGRESS-CTO; NCT02061436) after stratifying patients based on CTO-PCI indication into 2 groups: ACS vs non-ACS. PROGRESS-CTO includes patient-level data for CTO-PCI procedures performed between 2012-2022 at experienced CTO-PCI centers from the United States, Canada, Greece, Turkey, Egypt, Russia, and Lebanon.3 Study data were collected and managed using REDCap (Research Electronic Data Capture) electronic data-capture tools hosted at the Minneapolis Heart Institute Foundation.4,5
Definitions. CTOs were defined according to the definition of CTO Academic Research Consortium, as absence of antegrade flow through the lesion with a presumed or documented duration of ≥3 months.6 Technical success was defined as the successful canalization of the CTO vessel with <30% residual stenosis and final Thrombolysis in Myocardial Infarction (TIMI) 3 flow. Calcification was assessed by angiography as mild (spots), moderate (involving ≤50% of the reference lesion diameter), or severe (involving ≥50% of the reference lesion diameter).
The Multicenter CTO Registry of Japan (J-CTO) score was calculated as described by Morino et al7 and the PROGRESS-CTO major adverse cardiovascular events (MACE) score as described by Simsek et al.8 ACS at presentation included unstable angina, non-ST-segment elevation MI (NSTEMI) or STEMI as defined according to the American College of Cardiology (ACC) National Cardiovascular Data Registry (NCDR) CathPCI registry definitions.10 The ACS group underwent CTO-PCI during the ACS hospitalization.
In-hospital MACE were defined as the composite of in-hospital all-cause mortality, MI, stroke, urgent repeat revascularization (re-PCI or surgery), or pericardiocentesis. Procedural success was defined as technical success in the absence of in-hospital MACE. Adverse events during follow-up were defined as the composite of death, ACS, stent thrombosis, angiography, PCI, coronary artery bypass graft (CABG) surgery, and stroke. Myocardial infarction (MI) during follow-up was defined using the Third Universal Definition of Myocardial Infarction.9
Decisions regarding the CTO-PCI procedure were made by the heart team, including patient preference. The study was approved by the institutional review board of each participating site.
Statistical analysis. Continuous variables were presented as mean ± standard deviation or median (interquartile range) and compared using the independent t test or Mann-Whitney U test, as appropriate. Categorical variables were presented as absolute numbers and percentages and compared using Chi-square or Fisher’s exact test, as appropriate. The adverse events during the follow-up period were compared with log-rank test. Statistical analyses were performed using Stata, version 17.0 (StataCorp).
Results
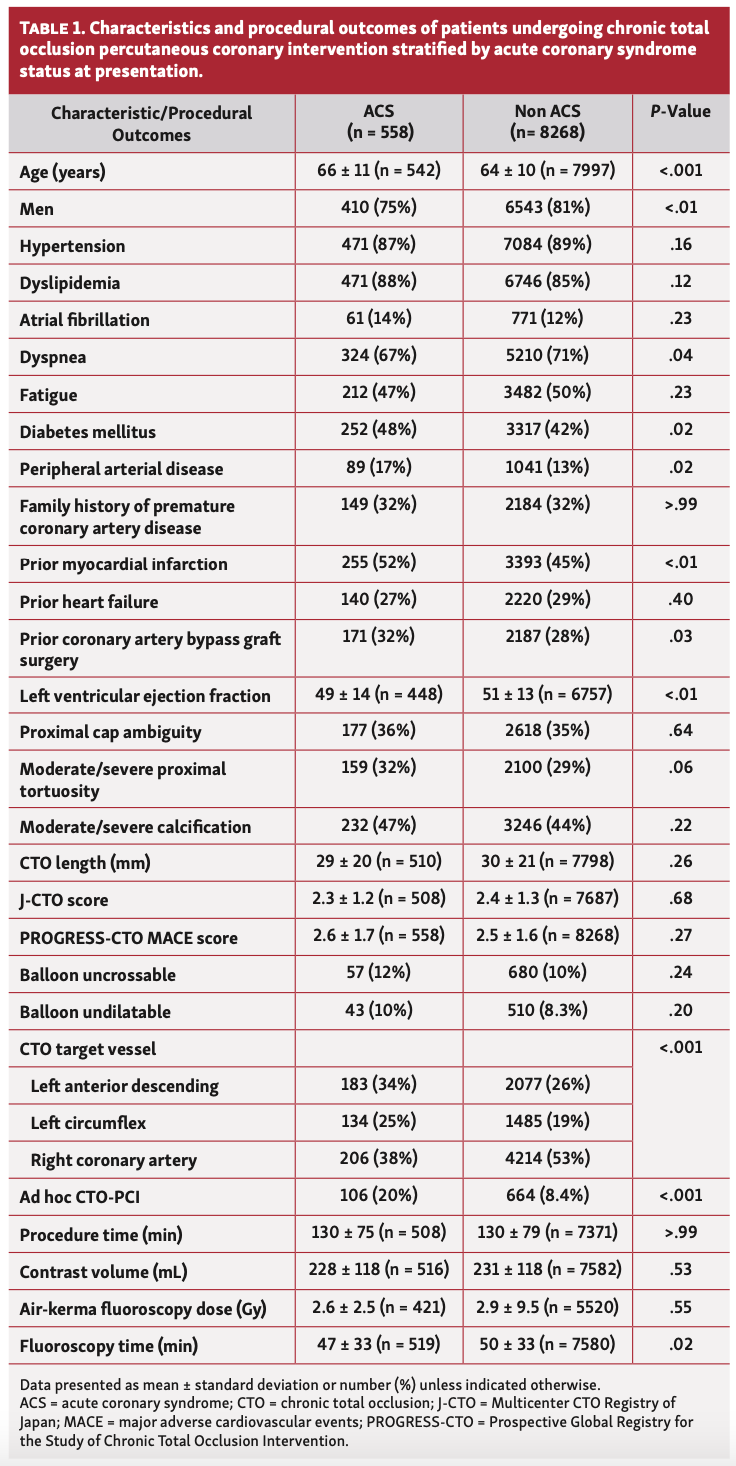
Clinical and angiographic characteristics. Of 8826 patients who underwent CTO-PCI during the study period, 558 (6.3%) presented with ACS; of these patients, the ACS type was available for 93.5%, with NSTEMI in 54%, unstable angina in 33%, and STEMI in 6.5%. ACS patients were older (66 ± 11 years vs 64 ± 10 years; P<.001) and had more comorbidities compared with non-ACS patients, including diabetes mellitus (48% vs 42%; P=.02), peripheral arterial disease (17% vs 13%; P=.02), prior MI (52% vs 45%; P<.01), and prior CABG (32% vs 28%; P=.03); they also had lower left ventricular ejection fraction (LVEF) (49 ± 14% vs 51 ± 13%; P<.01) (Table 1).
In ACS patients, the CTO vessel was more often the left anterior descending artery (34% vs 26%) and less often the right coronary artery (38% vs 53%) (overall P<.001). The successful crossing strategies were similar between ACS and non-ACS patients, with antegrade wiring in 61% vs 57%, retrograde wiring in 17% vs 16%, and antegrade dissection and re-entry in 12% vs 11%, respectively (overall P=.25).
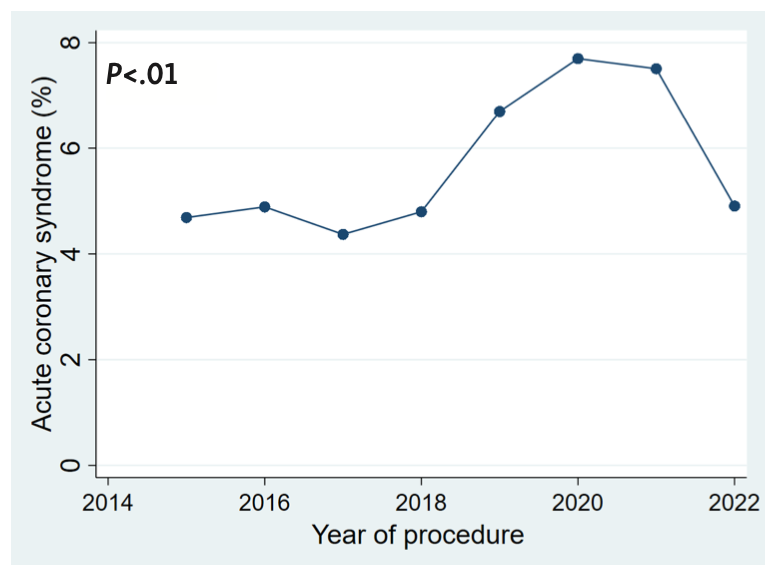
CTO lesion calcification, proximal cap ambiguity, CTO lesion length, and CTO vessel tortuosity were comparable between the ACS and non-ACS patients, as was the prevalence of balloon uncrossable and undilatable lesions. The prevalence of patients presenting with ACS who underwent CTO-PCI increased over time (Figure 1).
There was a trend for STEMI patients to be younger (66 ± 11 years vs 63 ± 13 years; P=.10) and to have lower prevalence of prior CABG (34% vs 18%; P=.07) compared with NSTEMI and unstable angina patients. Moreover, compared with NSTEMI and unstable angina patients, STEMI patients were less likely to have dyslipidemia (88% vs 68%; P<.001) and had more favorable angiographic characteristics including lower prevalence of distal cap at bifurcation (29% vs 10%; P=.02), lower PROGRESS-CTO score (1.4 ± 1.0 vs 0.9 ± 0.9; P<.01), and a trend for shorter fluoroscopy time (47 ± 33 minutes vs 36 ± 21 minutes; P=.058).
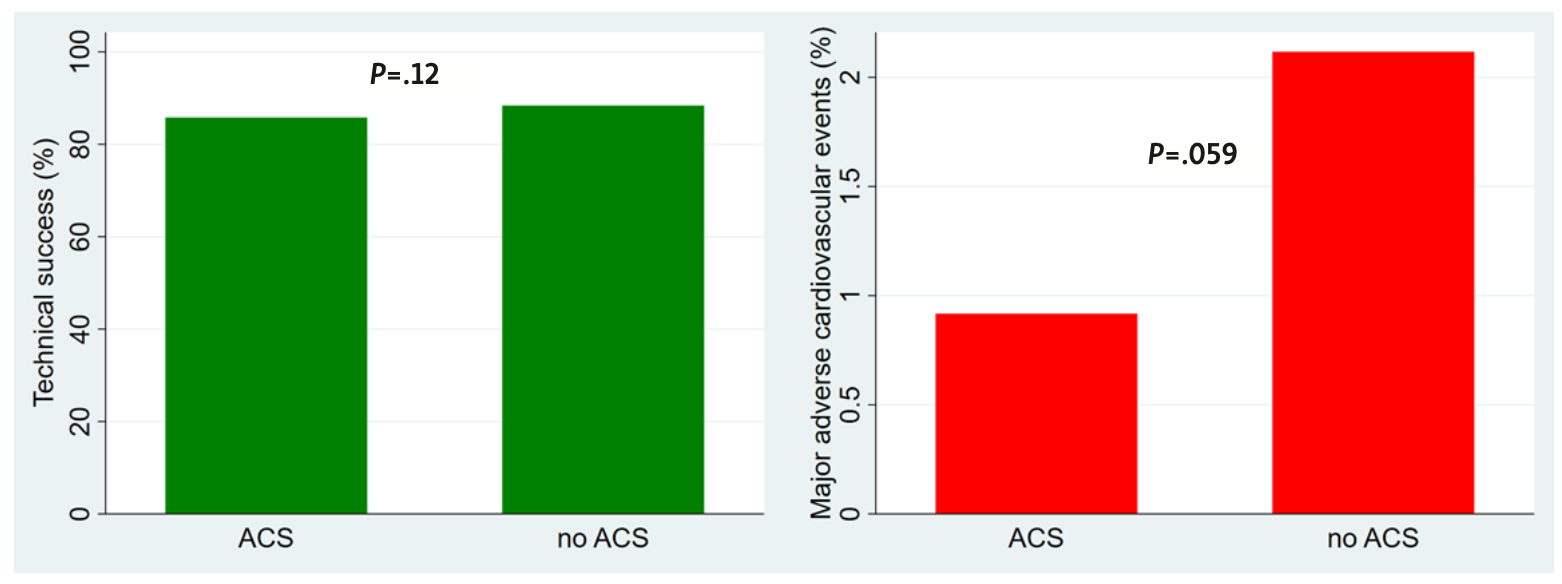
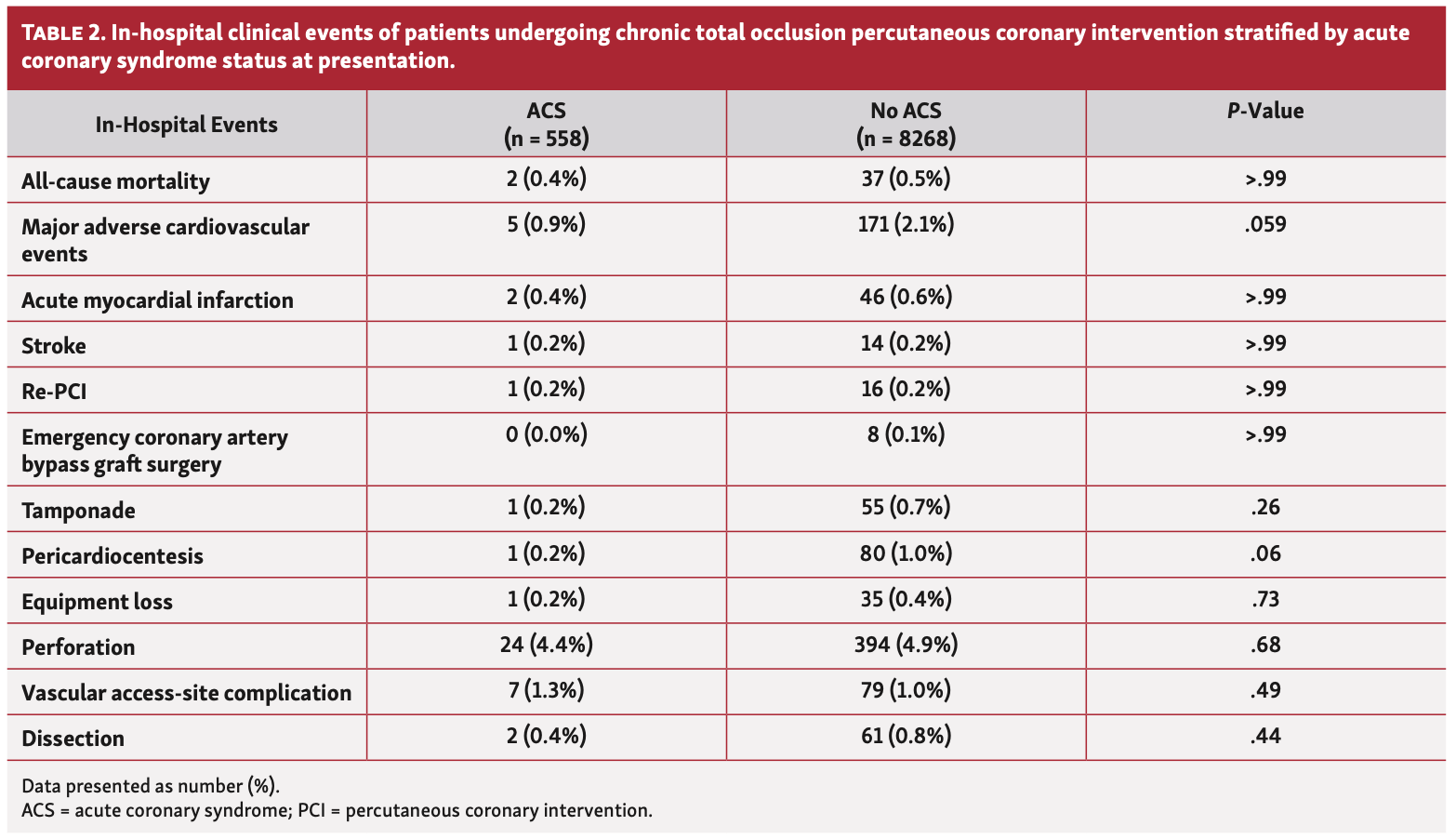
Procedural and in-hospital outcomes. Technical success (88% vs 86%; P=.12), procedural success (86% vs 84%; P=.30), and in-hospital MACE rates (0.9% vs 2.1%; P=.059) (Table 2) were similar between ACS vs non-ACS patients, respectively (Figure 2). Procedure time, contrast volume, and air-kerma fluoroscopy dose were similar between the ACS and non-ACS groups (Table 1).
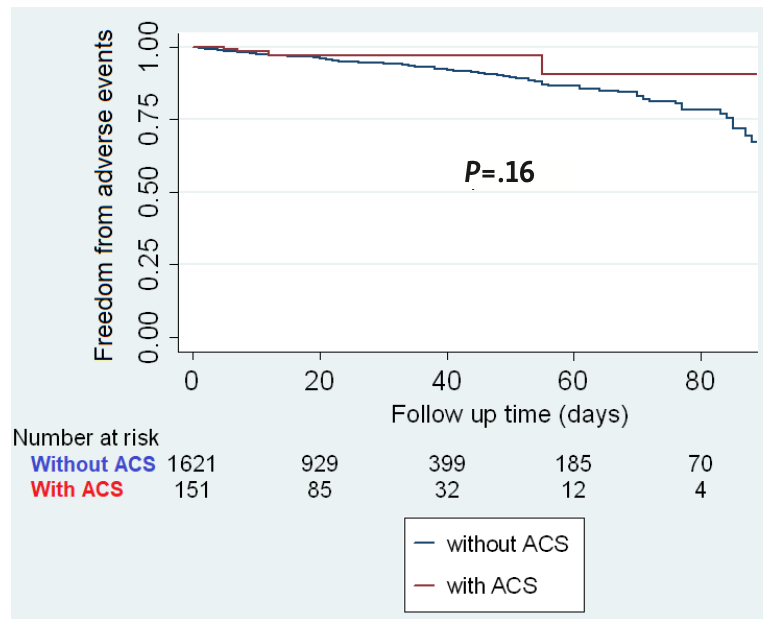
Follow-up outcomes. Limited follow-up data were available for 209 patients (37%) in the ACS group and 2749 patients (33%) in the non-ACS group. The median follow-up time was 31 days (IQR, 15-120) and 50 days (IQR, 19-308) for ACS and non-ACS groups, respectively. Within 90 days of discharge, 5 (2%) and 112 (4%) adverse events were observed in the ACS and non-ACS groups, respectively (P=.16) (Figure 3).
Discussion
The main findings of our study are as follows: (1) 6.3% of patients undergoing CTO-PCI presented with an ACS; and (2) ACS patients had a higher comorbidity burden but similar CTO-PCI success and in-hospital and follow-up adverse event rates.
Prevalence. CTOs are reported in 18%-52% of patients undergoing diagnostic angiography and in 54%-89% of prior CABG patients.11-14 Non-culprit CTOs are less common (10%) in patients who undergo primary PCI for STEMI.11,15,16 CTO-PCI in ACS patients increased after the COVID-19 pandemic, but recently returned to baseline (Figure 1). The prevalence of ACS patients in the OPEN-CTO (Outcomes, Patient Health Status, and Efficiency in Chronic Total Occlusion Hybrid Procedures) registry (7.3%) was similar with our study (6.3%).17
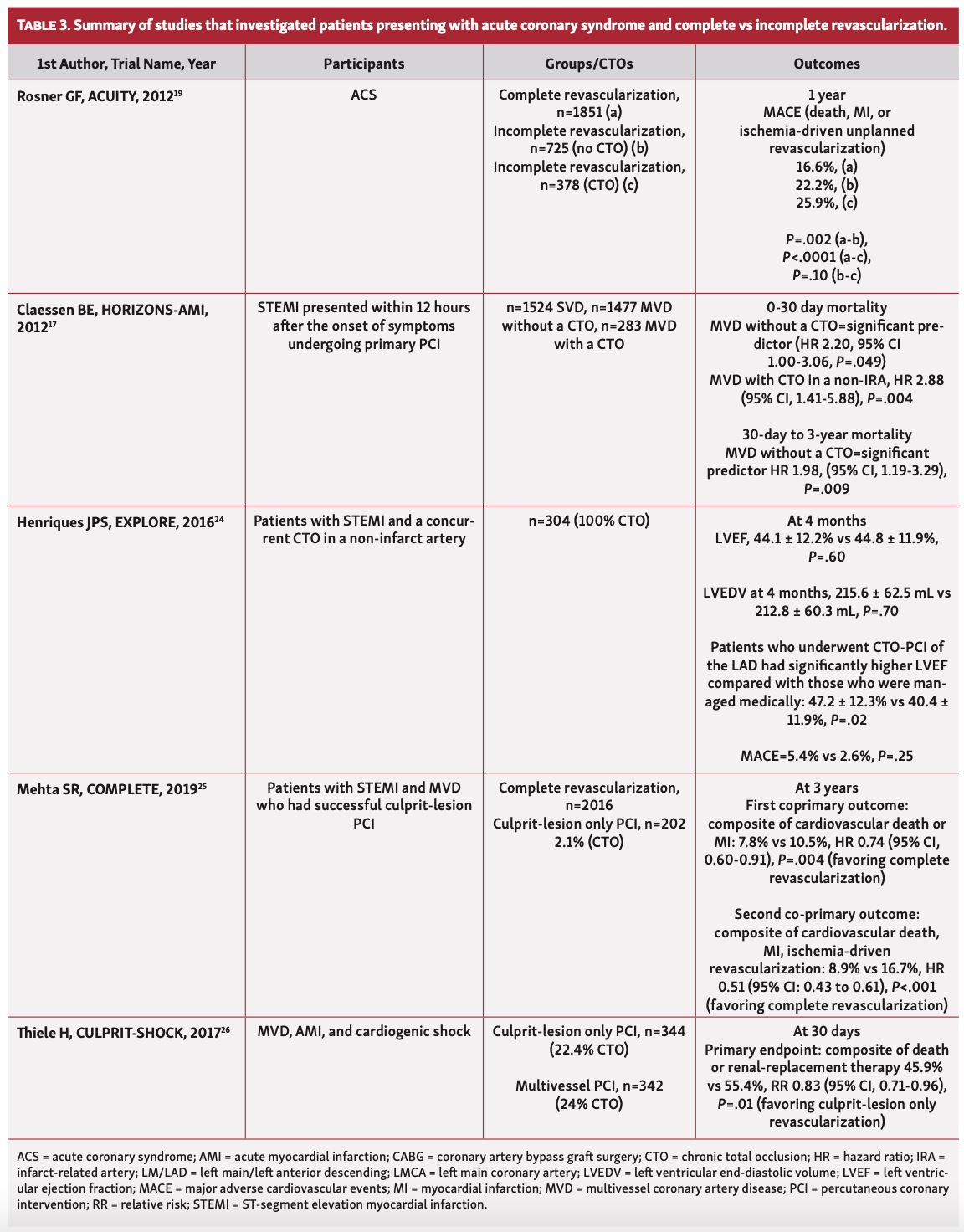
Outcomes and indications. While some studies indicate a potential benefit from revascularization of non-culprit CTOs in ACS, the results are inconclusive (Table 3). In the ACUITY (Acute Catheterization and Urgent Intervention Triage Strategy) trial, CTO patients who presented with unstable angina or NSTEMI and had incomplete revascularization had higher 1-year MACE compared with those who had complete revascularization.18
Multiple studies have shown worse outcomes in ACS patients who have a CTO vs those who do not. In the HORIZONS-AMI (Harmonizing Outcomes with Revascularization and Stents in Acute Myocardial Infarction) trial, among patients who presented with STEMI and 3-vessel coronary artery disease, those with CTOs had higher 3-year mortality.16 In another study of STEMI patients, the presence of a CTO was independently associated with 30-day mortality.15 Similar results have been observed in patients with multivessel disease, whereas those who had complete revascularization had significantly lower mortality and MACE compared with those who had incomplete revascularization with or without a CTO.19,20 Moreover, patients with CTOs who develop MI have been shown to have a higher risk of out-of-hospital cardiac arrest.21,22
In the EXPLORE (Evaluating Xience and Left Ventricular Function in Percutaneous Coronary Intervention on Occlusions After ST-Segment Elevation Myocardial Infarction) trial, at 4 months, LVEF and LV end-diastolic volume were similar between the CTO-PCI and no CTO-PCI groups. However, a subgroup analysis found that patients with LAD-CTOs randomized to CTO-PCI had significantly higher LVEFs compared with those who were randomized to no CTO-PCI.23
In the COMPLETE (The Complete versus Culprit-Only Revascularization Strategies to Treat Multivessel Disease after Early PCI for STEMI) trial, at a median follow-up of 3 years, the first co-primary outcome (composite of cardiovascular death and MI) was significantly lower in the complete revascularization group.24 However, CTOs represented 2.1% of the study cohort, thus, findings may not be applicable to CTO-PCI.
In the CULPRIT-SHOCK (The Culprit Lesion Only PCI versus Multivessel PCI in Cardiogenic Shock) trial, at 30 days, primary endpoint (composite of death and renal replacement therapy) was significantly lower in patients who underwent culprit-lesion only PCI. Moreover, the relative risk of death was also lower in the culprit-lesion only PCI group.25 Therefore, ad hoc CTO-PCI should not be attempted in ACS patients with cardiogenic shock; however, staged CTO recanalization could be considered by experienced operators to achieve complete revascularization.2
Careful angiographic review and procedural planning are recommended before CTO-PCI.26 Ad hoc CTO-PCI is not recommended, but was performed in approximately 10% of all CTO-PCI cases in our registry.27 These patients had lower J-CTO and PROGRESS-CTO scores, indicating lesser lesion complexity.27 Therefore, it is possible that operators with extensive experience in CTO-PCI aimed for total revascularization at the time of the index PCI. While CTO-PCI might offer benefit to a subgroup of ACS patients (eg, double jeopardy or in cases where the culprit vessel could not be recanalized), randomized controlled trials to date have not consistently shown any improvement in MACE following CTO-PCI.28-30
Study limitations. Our study has important limitations. First, the PROGRESS-CTO registry is observational and cases entered into the registry might be subject to selection bias. Second, events were not adjudicated by an independent clinical events adjudication committee. Third, PROGRESS-CTO operators are highly experienced in CTO-PCI, which could limit external validity. Fourth, our registry only collects CTO-PCI cases. As a result, we cannot determine the frequency of ad hoc CTO-PCI among all ACS patients. Fifth, follow-up was not available for all patients. Sixth, the type of MI at presentation (type 1, 2, 3, etc) was not collected.
Conclusion
Patients who present with ACS represent approximately 6% of those who undergo CTO-PCI and have higher comorbidity burden than non-ACS patients. While technical success and in-hospital MACE were similar between ACS and non-ACS presentations, meticulous procedural planning and risk/benefit assessment are crucial when contemplating CTO-PCI in this complex patient group.
Affiliations and Disclosures
From the 1Minneapolis Heart Institute and Minneapolis Heart Institute Foundation, Minneapolis, Minnesota; 2Department of Cardiology, Biruni University School of Medicine, Istanbul, Turkey; 3Division of Cardiology, Henry Ford Hospital, Detroit, Michigan; 4Massachusetts General Hospital, Harvard University, Boston, Massachusetts; 5Cleveland Clinic Foundation, Cleveland, Ohio; 6University Hospitals, Case Western Reserve University, Cleveland, Ohio; 7Department of Cardiology, Selcuk University, Konya, Turkey; 8North Oaks Healthcare System, Hammond, Louisiana; 9Department of Invasive Cardiology, Meshalkin National Medical Research Center, Ministry of Health of the Russian Federation, Novosibirsk, Russian Federation; 10Department of Cardiology, Central Arkansas Veterans Health System, and University of Arkansas for Medical Sciences, Little Rock, Arkansas; 11Department of Cardiology, Wellspan York Hospital, York, Pennsylvania; 12Memorial Bahcelievler Hospital, Istanbul, Turkey; 13Department of Cardiology, Aswan Heart Centre, Aswan, Egypt; 14Division of Cardiology, Tristar Hospitals, Tennessee; and the 15Division of Cardiovascular Medicine, UCSD Medical Center, La Jolla, California.
Funding: The authors are grateful for the philanthropic support of our generous anonymous donors, and the philanthropic support of Drs Mary Ann and Donald A. Sens; Mrs Diane and Dr Cline Hickok; Mrs Wilma and Mr Dale Johnson; Mrs Charlotte and Mr Jerry Golinvaux Family Fund; the Roehl Family Foundation; the Joseph Durda Foundation. The generous gifts of these donors to the Minneapolis Heart Institute Foundation’s Science Center for Coronary Artery Disease (CCAD) helped support this research project.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. Dr Alaswad is a consultant and speaker for Boston Scientific, Abbott Cardiovascular, Teleflex, and CSI. Dr Jaffer reports research sponsored by Canon, Siemens, Shockwave, Teleflex, Mercator, Boston Scientific; consultant for Boston Scientific, Siemens, Magenta Medical, IMDS, Asahi Intecc, Biotronik, Philips, Intravascular Imaging; equity interest in Intravascular Imaging, Inc, DurVena; licensing arrangements with Massachusetts General Hospital with Terumo, Canon, Spectrawave, for which he has the right to receive royalties. Dr Doshi reports speaker’s bureau for Abbott Vascular, Boston Scientific, and Medtronic; research support from Biotronik. Dr Khatri reports personal honoria for proctoring and speaking from Abbott Vascular, Asahi Intecc, Terumo, Boston Scientific. Dr Davies reports honoraria/consulting from Medtronic, Siemens Healthineers, and Asahi intec. Dr El Guindy reports consulting honoraria from Medtronic, Boston Scientific, Asahi Intecc, Abbott; proctorship fees from Medtronic, Boston Scientific, Asahi Intecc, Terumo; educational grants from Medtronic. Dr M. Patel reports consulting honoraria from Abbott, Medtronic, Terumo, Cardiovascular Systems, Inc. Dr Burke is a shareholder in Egg Medical and MHI Ventures. Dr Brilakis reports consulting/speaker honoraria from Abbott Vascular, American Heart Association (associate editor, Circulation), Amgen, Asahi Intecc, Biotronik, Boston Scientific, Cardiovascular Innovations Foundation (Board of Directors), ControlRad, CSI, Elsevier, GE Healthcare, IMDS, InfraRedx, Medicure, Medtronic, Opsens, Siemens, and Teleflex; research support from Boston Scientific, GE Healthcare; owner of Hippocrates LLC; shareholder in MHI Ventures, Cleerly Health, Stallion Medical. The remaining authors report no conflicts of interest regarding the content herein.
Manuscript accepted September 21, 2022.
Address for correspondence: Emmanouil S. Brilakis, MD, PhD, Center for Complex Coronary Interventions, Minneapolis Heart Institute, Center for Coronary Artery Disease at the Minneapolis Heart Institute Foundation, 920 East 28th Street #300, Minneapolis, MN 55407. Email: esbrilakis@gmail.com
References
1. Tajti P, Karmpaliotis D, Alaswad K, et al. The hybrid approach to chronic total occlusion percutaneous coronary intervention: update from the PROGRESS CTO Registry. JACC Cardiovasc Interv. 2018;11(14):1325-1335. Epub 2018 Apr 26. doi:10.1016/j.jcin.2018.02.036
2. Brilakis ES, Banerjee S, Lombardi WL. Retrograde recanalization of native coronary artery chronic occlusions via acutely occluded vein grafts. Catheter Cardiovasc Interv. 2010;75(1):109-113. doi:10.1002/ccd.22196
3. Xenogiannis I, Gkargkoulas F, Karmpaliotis D, et al. Temporal trends in chronic total occlusion percutaneous coronary interventions: insights from the PROGRESS-CTO Registry. J Invasive Cardiol. 2020;32(4):153-160. Epub 2020 Mar 20.
4. Harris PA, Taylor R, Minor BL, et al. The REDCap consortium: building an international community of software platform partners. J Biomed Inform. 2019;95:103208. Epub 2019 May 9. doi:10.1016/j.jbi.2019.103208
5. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)—a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(2):377-381. Epub 2008 Sep 30. doi:10.1016/j.jbi.2008.08.010
6. Ybarra LF, Rinfret S, Brilakis ES, et al. Definitions and clinical trial design principles for coronary artery chronic total occlusion therapies: CTO-ARC consensus recommendations. Circulation. 2021;143(5):479-500. Epub 2021 Feb 1. doi:10.1161/CIRCULATIONAHA.120.046754
7. Morino Y, Abe M, Morimoto T, et al. Predicting successful guidewire crossing through chronic total occlusion of native coronary lesions within 30 minutes: the J-CTO (Multicenter CTO Registry in Japan) score as a difficulty grading and time assessment tool. JACC Cardiovasc Interv. 2011;4(2):213-221. doi: 10.1016/j.jcin.2010.09.024
8. Simsek B, Kostantinis S, Karacsonyi J, et al. Predicting periprocedural complications in chronic total occlusion percutaneous coronary intervention: the PROGRESS-CTO complication scores. JACC Cardiovasc Interv. 2022;15(14):1413-1422. doi:10.1016/j.jcin.2022.06.007
9. Thygesen K, Alpert JS, Jaffe AS, et al. Third universal definition of myocardial infarction. Circulation. 2012;126(16):2020-2035. Epub 2012 Aug 24. doi:10.1161/CIR.0b013e31826e1058.
10. American College of Cardiology. Chest pain—MI registry inclusion criteria v3. 2019. Accessed December 6, 2022. https://cvquality.acc.org/docs/default-source/ncdr/registries/cpmiv3_inclusioncriteria_7-20-20.pdf?sfvrsn=92f786bf_0
11. Fefer P, Knudtson ML, Cheema AN, et al. Current perspectives on coronary chronic total occlusions: the Canadian Multicenter Chronic Total Occlusions Registry. J Am Coll Cardiol. 2012;59(11):991-997. doi:10.1016/j.jacc.2011.12.007
12. Shi Y, He S, Luo J, Jian W, Shen X, Liu J. Lesion characteristics and procedural complications of chronic total occlusion percutaneous coronary intervention in patients with prior bypass surgery: a meta-analysis. Clin Cardiol. 2022;45(1):18-30. Epub 2022 Jan 6. doi:10.1002/clc.23766
13. Christofferson RD, Lehmann KG, Martin GV, Every N, Caldwell JH, Kapadia SR. Effect of chronic total coronary occlusion on treatment strategy. Am J Cardiol. 2005;95(9):1088-1091. doi:10.1016/j.amjcard.2004.12.065
14. Jeroudi OM, Alomar ME, Michael TT, et al. Prevalence and management of coronary chronic total occlusions in a tertiary Veterans Affairs hospital. Catheter Cardiovasc Interv. 2014;84(4):637-643. Epub 2013 Nov 13. doi:10.1002/ccd.25264
15. Claessen BE, van der Schaaf RJ, Verouden NJ, et al. Evaluation of the effect of a concurrent chronic total occlusion on long-term mortality and left ventricular function in patients after primary percutaneous coronary intervention. JACC Cardiovasc Interv. 2009;2(11):1128-1134. doi:10.1016/j.jcin.2009.08.024
16. Claessen BE, Dangas GD, Weisz G, et al. Prognostic impact of a chronic total occlusion in a non-infarct-related artery in patients with ST-segment elevation myocardial infarction: 3-year results from the HORIZONS-AMI trial. Eur Heart J 2012;33(6):768-775. Epub 2012 Jan 12. doi:10.1093/eurheartj/ehr471
17. Sapontis J, Salisbury AC, Yeh RW, et al. Early procedural and health status outcomes after chronic total occlusion angioplasty: a report from the OPEN-CTO Registry (Outcomes, Patient Health Status, and Efficiency in Chronic Total Occlusion Hybrid Procedures). JACC Cardiovasc Interv. 2017;10(15):1523-1534. doi:10.1016/j.jcin.2017.05.065
18. Rosner GF, Kirtane AJ, Genereux P, et al. Impact of the presence and extent of incomplete angiographic revascularization after percutaneous coronary intervention in acute coronary syndromes: the Acute Catheterization and Urgent Intervention Triage Strategy (ACUITY) trial. Circulation. 2012;125(21):2613-2620. Epub 2012 May 1. doi:10.1161/CIRCULATIONAHA.111.069237
19. Hannan EL, Wu C, Walford G, et al. Incomplete revascularization in the era of drug-eluting stents: impact on adverse outcomes. JACC Cardiovasc Interv. 2009;2(1):17-25. doi:10.1016/j.jcin.2008.08.021
20. Hannan EL, Racz M, Holmes DR, et al. Impact of completeness of percutaneous coronary intervention revascularization on long-term outcomes in the stent era. Circulation. 2006;113(20):2406-2412. Epub 2006 May 15. doi:10.1161/CIRCULATIONAHA.106.612267
21. Reynolds JC. A funny thing happened on the way to the hospital. J Am Coll Cardiol. 2020;76(17):1944-1946. doi:10.1016/j.jacc.2020.09.006
22. Kosugi S, Shinouchi K, Ueda Y, et al. Clinical and angiographic features of patients with out-of-hospital cardiac arrest and acute myocardial infarction. J Am Coll Cardiol. 2020;76(17):1934-1943. doi:10.1016/j.jacc.2020.08.057
23. Henriques JP, Hoebers LP, Råmunddal T, et al. Percutaneous intervention for concurrent chronic total occlusions in patients with STEMI: the EXPLORE trial. J Am Coll Cardiol. 2016;68(15):1622-1632. doi:10.1016/j.jacc.2016.07.744
24. Mehta SR, Wood DA, Storey RF, et al. Complete revascularization with multivessel PCI for myocardial infarction. N Engl J Med. 2019;381(15):1411-1421. Epub 2019 Sep 1. doi:10.1056/NEJMoa1907775
25. Thiele H, Akin I, Sandri M, et al. PCI strategies in patients with acute myocardial infarction and cardiogenic shock. N Engl J Med. 2017;377(25):2419-2432. Epub 2017 Oct 30. doi:10.1056/NEJMoa1710261
26. Lembo NJ, Karmpaliotis D, Kandzari DE. CTO-PCI procedural planning. Interv Cardiol Clin. 2012;1(3):299-308. Epub 2012 Jun 5. doi:10.1016/j.iccl.2012.04.002
27. Sandoval Y, Tajti P, Karatasakis A, et al. Frequency and outcomes of ad hoc versus planned chronic total occlusion percutaneous coronary intervention: multicenter experience. J Invasive Cardiol. 2019;31(5):133-139. Epub 2019 Jan 15.
28. Werner GS, Martin-Yuste V, Hildick-Smith D, et al. A randomized multicentre trial to compare revascularization with optimal medical therapy for the treatment of chronic total coronary occlusions. Eur Heart J. 2018;39(26):2484-2493. doi:10.1093/eurheartj/ehy220
29. Lee SW, Lee PH, Ahn JM, et al. Randomized trial evaluating percutaneous coronary intervention for the treatment of chronic total occlusion. Circulation. 2019;139(14):1674-1683. doi:10.1161/CIRCULATIONAHA.118.031313
30. Brilakis ES, Mashayekhi K, Burke MN. How DECISION-CTO can help guide the decision to perform chronic total occlusion percutaneous coronary intervention. Circulation. 2019;139(14):1684-1687. doi:10.1161/CIRCULATIONAHA.119.039835











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}