


Perceptions of Interventional Cardiologists on Diversity and Discrimination
© 2024 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
Abstract
Background. There are limited data on diversity and discrimination against interventional cardiologists (ICs).
Methods. We performed an online, anonymous, international survey of interventional cardiologists on their perceptions of diversity and discrimination in their field.
Results. A total of 445 ICs participated in the survey. The median age of participants was 46 to 50 years and most (60%) practice in the United States. Among the respondents, 13% identified as women, while 31% identified as Asian, 10% as Latino, and 3.2% as Black/African American. Women ICs were less likely to be married (62% vs 92%; P < .001) or have children (48% vs 87%; P < .001). Women, non-native English speakers, and non-white individuals had a higher likelihood of reporting discrimination from patients/families, peers, supervisors, support staff, and nursing staff, compared with men, native English speakers, and non-Hispanic white individuals, respectively. Women were less satisfied with the level of gender diversity in their workplace (25% vs 45%; P = .015) and were more likely to believe that women physicians have fewer opportunities in the field of IC compared with men (69% vs 35%; P < .001). Non-white individuals were more likely to believe that their race/ethnicity may impede the progress of their career (54% vs 15%; P < .001), that their race/ethnicity negatively impacted their fellowship prospects/acceptance (35% vs 11%; P < .001), and that their religion negatively impacted their fellowship prospects/acceptance (17% vs 4%; P = .003). Several participants (41%) expressed concerns that diversity, equity, and inclusion initiatives might result in unintended consequences.
Conclusions. Our survey suggests that ICs perceive high rates of discrimination in their field.
Introduction
A diverse medical workforce has been associated with enhanced quality of patient care and superior financial performance.1 However, women and various races and ethnicities are underrepresented in the field of interventional cardiology (IC).2-4 Cardiologists encounter gender, age, and race-based discrimination.5 However, data on diversity and discrimination among interventional cardiologists (ICs) are lacking. Gender-based discrimination has been identified as a leading factor that negatively impacts the pursuit of IC as a subspecialty among women cardiology fellows.6 We conducted a global, web-based survey of IC fellows and attendings to assess their perceptions of diversity and discrimination.
Methods
The survey questionnaire was collaboratively developed by the co-authors through an interactive process. The team of co-authors comprised individuals from diverse backgrounds, including interventional cardiologists, health equity experts, university-based physicians, and private practice physicians. The final survey consisted of 48 questions in the English language and encompassed 5 distinct segments: (1) demographic information; (2) perspectives on discrimination against physicians; (3) perspectives on gender diversity; (4) perspectives on race/ethnicity diversity; and (5) perspectives on patient diversity. The survey was conducted using REDCap (Research Electronic Data Capture)7,8 and was distributed to IC attendings and fellows via social media and email lists (6672 emails). The study was approved by the institutional review board, and consent was waived.
The participant group labeled as "non-white" included individuals who identified as Native American/Alaska Native, Asian, Black/African American, Native Hawaiian/Pacific Islander, and Hispanic white.
Analyses comparing the non-white with non-Hispanic white groups were exclusively conducted among participants practicing within the United States. Analyses comparing native English speakers to non-native English speakers were exclusively conducted among participants practicing in English-speaking countries (US, UK, Canada, and Australia).
Categorical variables were expressed as percentages and compared using the Pearson’s chi-square test. Continuous variables are presented as mean ± standard deviation or as median (interquartile range) unless otherwise specified and were compared using the independent-samples t test for normally distributed variables and the Mann-Whitney U test for non-parametric variables, as appropriate. All statistical analyses were performed using R Statistical Software, version 4.2.2 (R Foundation for Statistical Computing). A P-value of less than 0.05 was considered statistically significant.
Results
Participant demographics. A total of 445 ICs (379 IC attendings and 66 IC fellows) participated in the survey. The median age range of the participants was 46 to 50 years. Among the respondents, 13% were women, 31% identified as Asian, 10% as Latino, 3.2% as Black/African American, and 0.2% as Native American. Most participants practiced in the United States (60%), followed by the European Union (9%), India (9%), the United Kingdom (4%), and South America (3%). Most respondents were married (88%), and 82% had at least 1 child. The predominant setting for IC programs was academic (51% university-based and 15% university-affiliated), followed by private hospitals (13%), government hospitals (11%), and community-based settings (9%).
Women who took the survey were younger than men (median age 41-45 years vs 46-50 years; P = .013), less likely to be married (62% vs 92%; P < .001), and less likely to have at least 1 child (48% vs 87%; P [adjusted for age] < .001), or at least 2 children (26% vs 72%; P [adjusted for age] < .001). Women had fewer median years of experience compared with men (6-10 years vs 11-15 years; P = .001), but there were no differences observed between men and women in the median annual volume of percutaneous coronary interventions (PCI) and structural and peripheral cases.
Participants practicing in academic hospitals were older (median age 46-50 vs 41-45; P = .041), more likely to identify as non-Hispanic white (49% vs 37%; P = .015), and more likely to practice in the United States (68% vs 47%; P < .001) compared with participants practicing in non-academic programs.
Among participants practicing in the United States (n = 269), 25% identified as Asian, 8% as Latino, 3.7% as Black/African American, and 0.4% as Native American, and 53% of these participants were born in the United States. Most participants in the United States received medical training in the United States (95%), while 58% attended a US medical school.
Non-white participants were younger than non-Hispanic white participants (median age 41-45 years vs 51-55 years; P < .001), and less likely to have more than one child (66% vs 81%), however the difference was not significant after adjusting for age. US-born participants were older (median age 51-55 vs 46-50; P < .001), more likely to be non-Hispanic white (76% vs 25%; P < .001), and more likely to have children (91% vs 84%; P = .013) compared with participants practicing in the United States who were not born there.
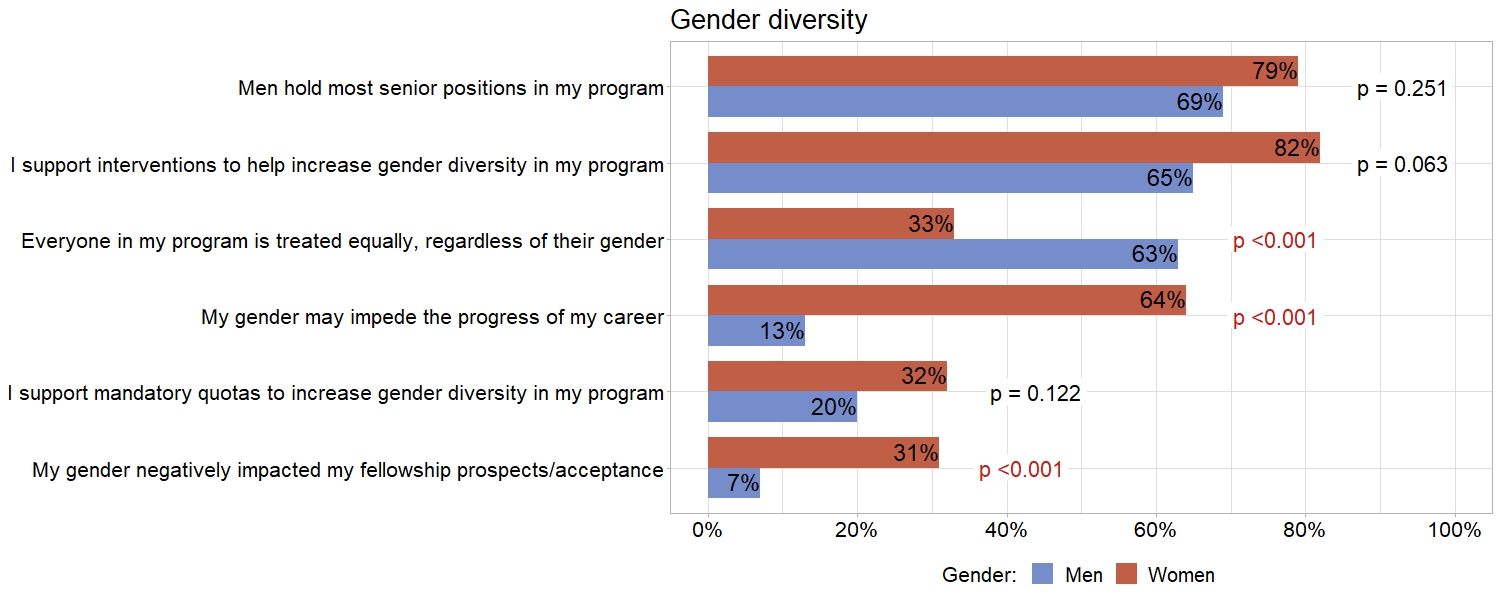
Gender diversity. Among survey participants, 43% expressed satisfaction with the current level of gender diversity at their workplace. However, women displayed significantly lower levels of satisfaction compared with men (25% vs 45%; P = .015). Women were less likely to believe that everyone in their program is treated equally regardless of their gender, and more likely to believe that their gender may impede the progress of their career and that their gender negatively impacted their fellowship prospects/acceptance (Figure 1). Additionally, women more often believed that non-male physicians have fewer opportunities in the field of IC (69% vs 35%; P < .001), and that interventions to improve physician gender diversity are required to enhance the quality of care provided, compared with men (69% vs 38%; P < .001).
The median reported paid maternity leave offered by programs was 10 to 12 weeks, but 25% of the respondents reported that their program did not offer paid maternity leave. Women were more likely to believe that taking maternity leave can adversely affect a physician’s career, compared with men (62% vs 37%; P = .005). The median length of paid maternity leave was shorter in the United States compared with non-US programs (6-8 weeks vs 20+ weeks; P < .001).
The median reported paid paternity leave offered by programs was 4 to 6 weeks, while 41% of the respondents reported that their programs do not provide paid maternity leave. Men were more likely to believe that taking a paternity leave can adversely affect a physician’s career, compared with women (34% vs 14%; P = .033). There was no difference in paternity leave duration between US and non-US programs.
Racial/ethnic diversity. Among the participants practicing in the United States (n = 269), 51% expressed satisfaction with the current level of racial/ethnic diversity at their workplace, with no significant difference between non-white and non-Hispanic white individuals. Non-white individuals were more likely to believe that their race/ethnicity may impede the progress of their career, that their race/ethnicity negatively impacted their fellowship prospects/acceptance, and that their religion negatively impacted their fellowship prospects/acceptance (Figure 2). They were also more likely to support mandatory quotas to increase racial/ethnic diversity in their program.
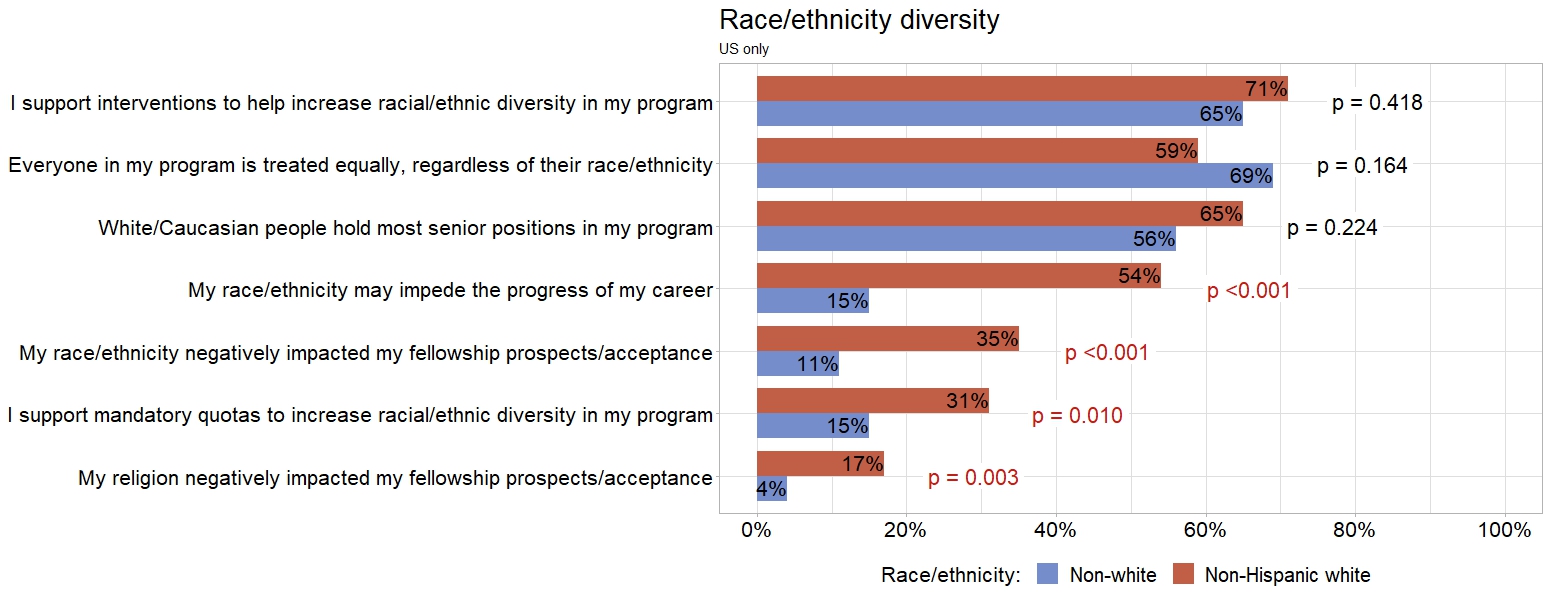
Forty-six percent of respondents believed that underrepresented minority physicians have fewer opportunities in the field of IC, with no difference between non-white and non-Hispanic white. Non-white respondents were more likely to believe that interventions to improve physician racial/ethnic diversity are required to enhance the quality of care provided, compared with non-Hispanic white respondents (57% vs 44%; P = .024). Diversity acceptance or cultural competency training was required in 59% of the US participants’ workplaces, while 15% of the responders did not know if there is required training at their workplace.
Discrimination against physicians. Participants identified several characteristics contributing to discrimination against physicians in their workplace: language accent (48%), race/ethnicity (44%), age (44%), gender (43%), appearance/clothing (40%), body size (34%), physical disability (29%), religion (25%), and sexual orientation (23%). The most common sources of discrimination reported, according to the participants, were patients and families (57%), followed by peers (49%), supervisors (46%), nursing staff (40%), and support staff (39%). Of the 9% of participants (n = 42) who reported incidents of discrimination to their respective organizations, only 19% (n = 8) expressed satisfaction with the response received.
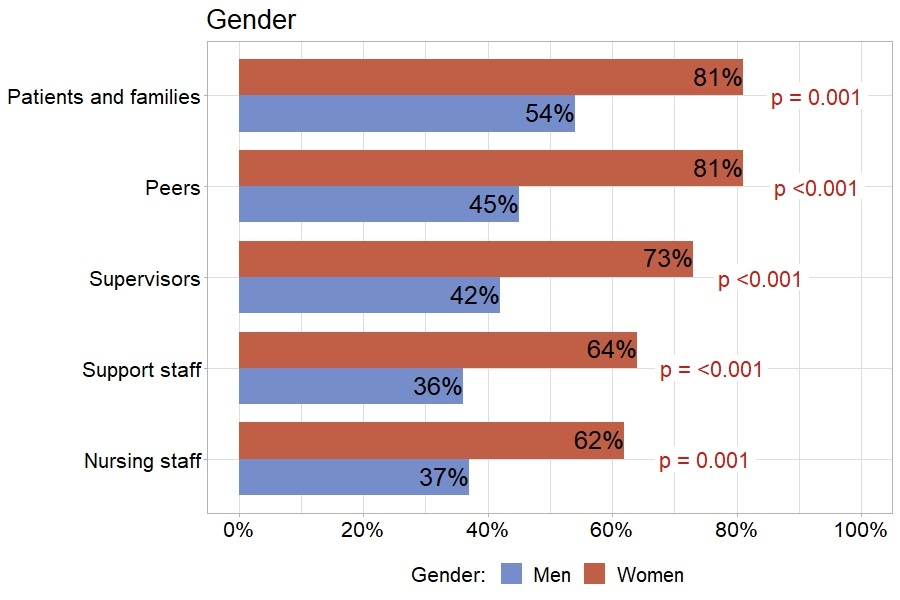
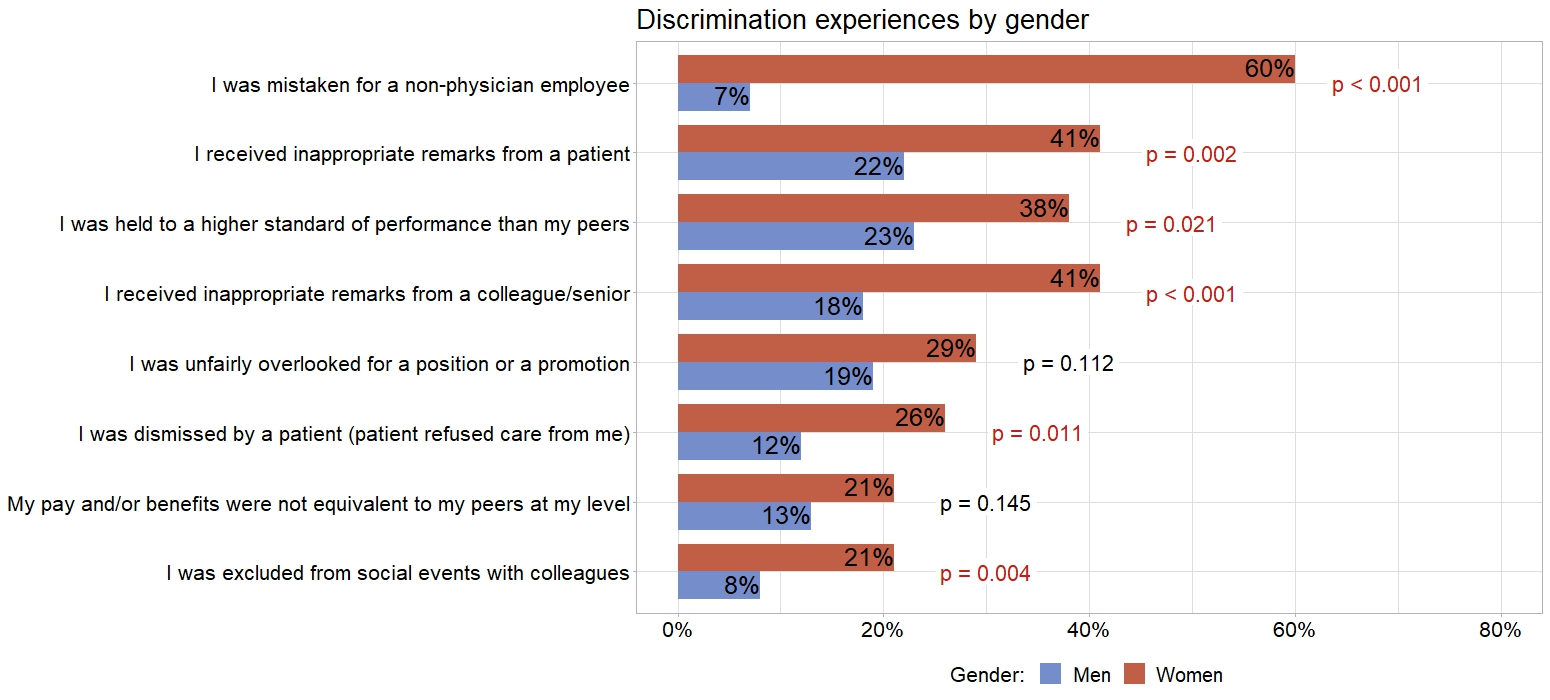
Women exhibited a higher likelihood of reporting discrimination from patients and families, peers, supervisors, support staff, and nursing staff, compared with men (Figure 3). Gender was singled out by women as the principal attribute leading to discrimination against them (69%), while 10% of female participants disclosed never having experienced any form of discrimination. Women reported a higher incidence of various forms of discrimination, compared with men (Figure 4).
There were no differences in reported discrimination between participants practicing in academic vs non-academic programs.
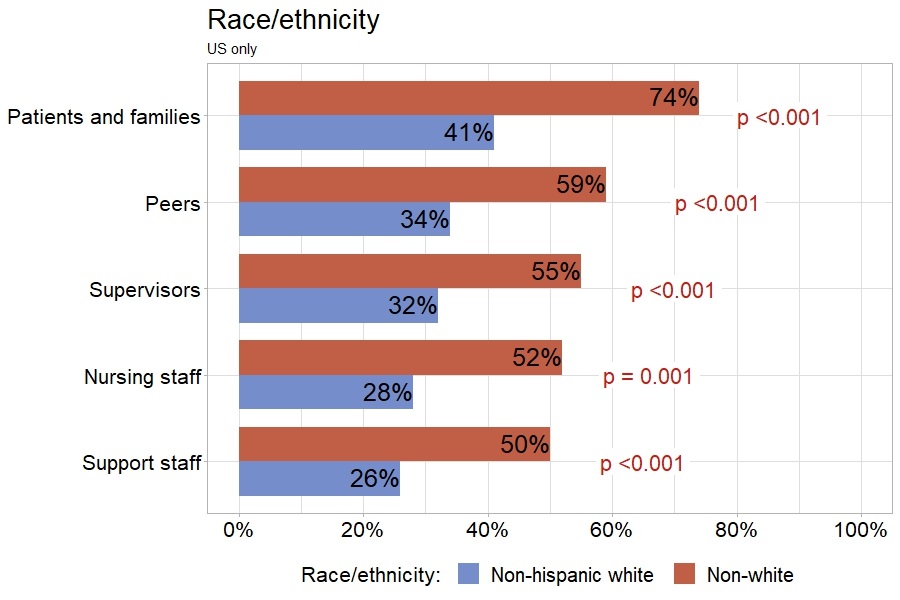
Among respondents practicing in the United States (n = 269), non-white physicians were more likely to report experiencing discrimination from patients and families, peers, supervisors, support staff, and nursing staff, compared with non-Hispanic white physicians (Figure 5). Non-white respondents were also more likely to report having been held to a higher standard of performance than their peers, compared with non-Hispanic white respondents (34% vs 18%; P = .003).
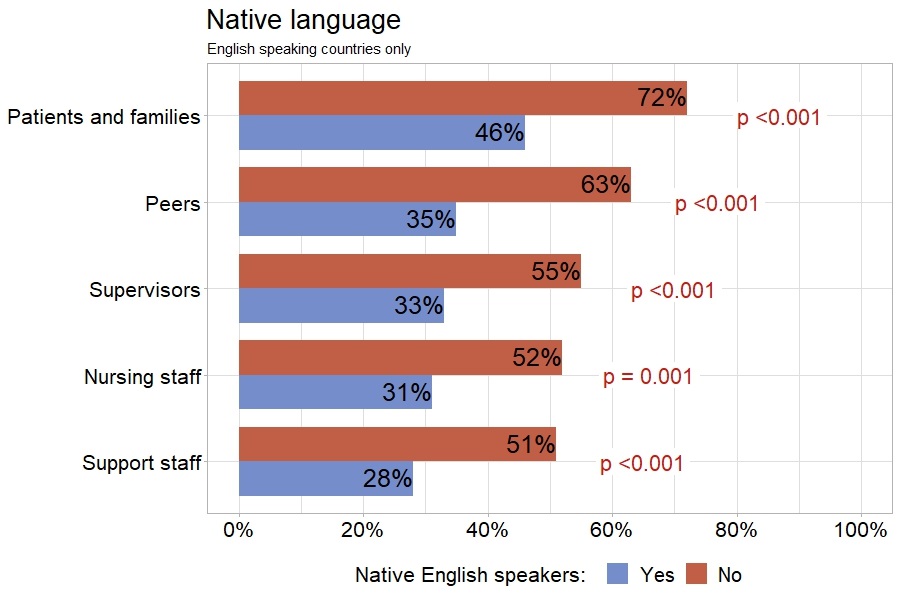
Among participants who practice in the United States, United Kingdom, Canada, and Australia (n = 296), physicians whose native language was not English demonstrated a higher likelihood of reporting discrimination from patients and families, peers, supervisors, support staff, and nursing staff, compared with native English speakers (Figure 6). They were also more likely to report being held to a higher standard of performance than their peers (33% vs 22%; P = .042), being unfairly overlooked for a position or promotion (31% vs 13%; P < .001), and receiving inappropriate remarks from a colleague/senior (28% vs 17%; P = .038), compared with native English speakers.
Unintended consequences. Forty-one percent of participants were concerned about unintended consequences of Diversity, Equity, and Inclusion (DEI) initiatives: 29% of women vs 43% of men (P = .102), and 46% of non-white responders vs 58% of non-Hispanic white responders (P = .077).
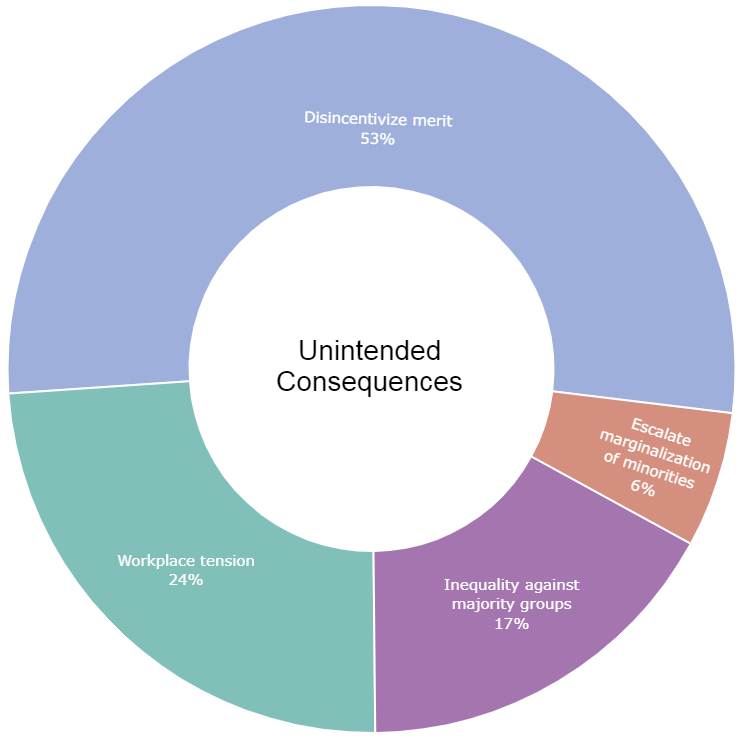
Participants were provided with a free-form textbox to describe why they believe DEI initiatives could have unintended consequences. The 83 responses received were divided into 4 categories. Most respondents (53%) believed that DEI initiatives could disincentivize merit when selecting physicians, 24% believed that DEI initiatives can create tension in the workplace, 17% believed that DEI initiatives could lead to inequality against majority groups, and 6% believed that they could escalate the marginalization of minority groups (Figure 7).
Discussion
Our study provides a current snapshot of opinions on discrimination and diversity among interventional cardiologists. The main findings of our study are that (a) women practicing IC are less likely to be married or have children (results were adjusted for age); (b) women, non-native English speakers, and non-white individuals have a higher likelihood of reporting discrimination from patients and families, peers, supervisors, support staff, and nursing staff, compared with men, native English speakers, and non-Hispanic white individuals; (c) women are less likely to be satisfied with the level of gender diversity in their workplace and more often believe that non-male physicians have fewer opportunities in the field of IC; (d) non-white individuals are more likely to believe that their race/ethnicity may impede the progress of their career, that their race/ethnicity negatively impacted their fellowship prospects/acceptance, and that their religion negatively impacted their fellowship prospects/acceptance; (e) a portion of the participants (41%) expressed concerns that DEI initiatives might result in unintended consequences, including disincentivizing merit, workplace tension, inequality against majority groups, and escalation of the marginalization against minorities.
The 2021 physician specialty data report by the Association of American Medical Colleges (AAMC) revealed that interventional cardiology is one of the medical fields with the lowest women representation in the United States (8.2%), while Hispanic (5.6%) and Black/African American (4%) individuals are also underrepresented.2 Among the European Society of Cardiology (ESC) organizations, the European Association of Percutaneous Coronary Intervention (EAPCI) has the lowest female representation (15.3%).4 A study of medical practitioners in Australia and New Zealand found that women make up 4.8% of interventional cardiologists.3 In our study, the representation of women interventionalists was similar with that found in the literature (13%), as was the representation of Latino (8%) and Black/African American (3.7%) individuals practicing in the United States.
Pregnancy and family planning are key considerations for women pursuing a career in IC, with the present survey demonstrating that women interventionalists are less likely to be married or have 1 or more children. A 2016 EAPCI survey found that women practicing IC were less frequently married (57.0% vs 79.8%; P < .001) and more likely to not have children (46.6% vs 20.5%; P < .001), compared with men.9 The Gender-CATH (Gender-Catheterization laboratory) study in Italy demonstrated similar findings, with women being more frequently unmarried (22.1% vs 8.7%; P = .002) and childless (43.9% vs 56.1%; P < .001).10
One of the primary challenges faced by women in IC, particularly in the United States, is limited maternity leave. According to our survey, the median duration of maternity leave offered by US programs is 6 to 8 weeks, and 62% of women believe that taking maternity leave could have a negative impact on their career. A survey conducted in 2017 among female members of the American College of Cardiology (ACC) found that out of 607 pregnancies, 48% of women took a maternity leave of less than 8 weeks, while 51% felt pressured to take shorter leaves than what was available to them.11 In the same study, 43% of women reported being asked about their intentions regarding having children during job interviews.11 Another concern specific to IC is the potential risk of radiation exposure during pregnancy, which emerged as one of the main deterrents for female cardiology fellows considering IC as a subspecialty.6
Gender-based discrimination was also one of the main barriers to choosing IC for female cardiology fellows.6 A 2022 survey of 6512 physicians from all specialties revealed that women were significantly more prone to sexist remarks (51.0% vs 15.1%; P < .001) and unwelcome sexual advances (29.6% vs 15.0%; P < .001) from patients, families, or visitors, compared with men; 27.5% of female physicians had a patient refuse their care.12 A 2021 American College of Cardiology survey of 5931 cardiologists showed that women experienced discrimination more frequently than men (56% vs 22%; P < .001), and gender-based discrimination was the most common form (44%).5 Among participants of that survey, administrative staff (49%) and colleagues (45%) were identified as the primary sources of discrimination, followed by patients (32%) and senior colleagues (29%).5
Our survey focusing on IC found that women were more likely to feel discrimination from all sources, including patients/families, peers, supervisors, support staff, and nursing staff (Figure 3). However, the primary sources of reported discrimination were different compared with the ones found in the general cardiology survey by ACC, with patients/families being the most frequent source in our survey. Female participants in our survey were also more likely to report experiencing certain forms of discrimination: the most common form was being mistaken for a non-physician employee (Figure 4).
Racial/ethnic diversity of the medical workforce can improve patient satisfaction, as race-concordant visits are typically longer and associated with greater patient positive affect.13 Given that Black/African American and Native American individuals are disproportionally affected by cardiovascular disease, diversity in the field of cardiology becomes even more crucial.14 Furthermore, racially/ethnically diverse populations are underrepresented in clinical trials and thus benefit less from scientific discoveries.15 A diverse medical workforce can enhance minority participation in clinical trials. Lastly, a diverse teaching environment has been shown to better prepare students for treating diverse populations.16 However, in our study, respondents practicing in an academic setting were older (median age 46-50 vs 41-45; P = .041) and more likely to identify as non-Hispanic white (49% vs 37%; P = .015).
Race/ethnicity-based discrimination is prevalent in medicine and has a significant impact on physician diversity.17,18 A survey of physicians from all specialties showed that non-Hispanic Black physicians (55.8%), non-Hispanic Asian, Native Hawaiian, or Pacific Islander physicians (55.4%), and non-Hispanic Indigenous or other physicians (52.5%) were more likely to experience offensive racial or ethnic remarks by patients, family members, or visitors, compared with White physicians (22.0%; P < .001).12 Data from the 2015 professional life survey (PLS) from ACC revealed that among 2245 cardiologists underrepresented minorities (52.3%) and Asians/Pacific Islanders (45.5%) were more likely to report experiencing discrimination compared with Whites (36.4%; P < .01).19 Similarly, in our study, non-white US interventionalists in the United States reported more discrimination (Figure 5), and were more likely to report being held to a higher standard of performance than their peers, compared with non-Hispanic white respondents.
Language accent has been shown to affect the patient’s perception of the physician’s competence, leading to bias against foreign-accented doctors.20 In our survey, non-native English speakers practicing IC in English-speaking countries reported facing significantly more discrimination than their native-speaking counterparts (Figure 6).
Despite our finding of a significant perception of discrimination experienced by ICs with respect to gender, race/ethnicity, and native language, a considerable portion, including those belonging to "disadvantaged" groups, expressed their belief that diversity, equity, and inclusion (DEI) initiatives may have unintended consequences (Figure 7). Dover et al propose that organizations frequently adopt DEI initiatives to reduce discrimination without relying on substantial evidence.21 They further suggest that although these initiatives are well-intentioned, when not grounded in evidence they can lead to unintended consequences by impeding the identification and resolution of discrimination directed towards “disadvantaged” groups, increasing sensitivity of discrimination against “advantaged” groups, evoking feelings of threat and victimization among “advantaged” groups, and generating uncertainties regarding the competence and attributions of individuals belonging to “disadvantaged” groups.21
This situation gives rise to a major worry. If a substantial number of individuals from underrepresented backgrounds, including women, believe they are discriminated against and acknowledge the necessity for greater diversity, but also perceive negative repercussions from diversity, equity, and inclusion efforts, they might find themselves in a difficult position. Instead of actively intervening to foster diversity and inclusion, they might consider enduring the hostile environment resulting from a lack of diversity and waiting for the field to naturally become more diverse. However, research indicates that comprehensive training can effectively reduce implicit bias and promote an inclusive workplace atmosphere.22 Despite this, institutions often prefer short, 1-time training sessions, which research has shown to be ineffective.22 Notwithstanding the legal prohibition of discriminatory practices based on race, color, religion, national origin, or sex, the actual prevention of such discrimination and the promotion of workplace diversity presents a significant challenge.
Limitations. Participants might be more interested in diversity and discrimination than non-responders, which might result in selection bias. The utilization of email lists and social media for participant recruitment may introduce additional selection bias. Given the global nature of this survey, disparities in cultural norms, expectations, and linguistic barriers could influence the interpretation of "discrimination" across different regions. To tackle this limitation, we abstained from explicitly defining the term, opting instead to permit respondents to individually interpret and contribute their own cultural context and personal experiences.
Conclusions
Our study demonstrates that there is a high prevalence of perceived discrimination against physicians and an increasing need for diversity in the field of interventional cardiology. Women and non-white individuals encounter obstacles in career advancement and face bias, both by patients and colleagues. The optimal ways to decrease discrimination and increase diversity remain to be determined.
Affiliations and Disclosures
Athanasios Rempakos, MD1; Michaella Alexandrou, MD1; Bahadir Simsek, MD1; Spyridon Kostantinis, MD1; Judit Karacsonyi, MD, PhD1; Deniz Mutlu, MD1; Allison Hall, MD2; Arnold H. Seto, MD3; Barbara Danek, MD4; Binita Shah, MD5; Courtney Baechler, MD, MS1; Delaine Thomas, MPH1; James W. Choi, MD6; Jeremy Rier, DO7; Kathleen E. Kearney, MD4; Ki Park, MD, MS8; Mosi Bennett, MD, PhD1; Santiago Garcia, MD9; Thao Duong, MD10; Jimmy Kerrigan, MD11; Ahmed Al-Ogaili, MD1; Bavana V. Rangan, BDS, MPH1; Olga C. Mastrodemos, BA1; Salman S. Allana, MD1; Yader Sandoval, MD1; M. Nicholas Burke, MD1; Emmanouil S. Brilakis, MD, PhD1
From the 1Minneapolis Heart Institute and Minneapolis Heart Institute Foundation, Abbott Northwestern Hospital, Minneapolis, Minnesota, USA; 2Eastern Health, Memorial University of Newfoundland, St. John's, Newfoundland, Canada; 3Long Beach VA Health Care System, Long Beach, California, USA; 4Division of Cardiology, University of Washington, Seattle, Washington, USA; 5Division of Cardiology, Department of Medicine, NYU Grossman School of Medicine, New York, New York; 6Texas Health Presbyterian Hospital, Dallas, Texas, USA; 7WellSpan York Hospital, York, Pennsylvania, USA; 8Cardiovascular Medicine, University of Florida College of Medicine, Gainesville, Florida, USA; 9The Christ Hospital, Cincinnati, Ohio, USA; 10HCA Midwest Health, Overland Park, Kansas, USA; 11Division of Cardiology, Ascension Saint Thomas Heart, Nashville, Tennessee, USA.
Acknowledgments: The authors are grateful for the philanthropic support of our generous anonymous donors, and the philanthropic support of Drs. Mary Ann and Donald A Sens; Mrs. Diane and Dr. Cline Hickok; Mrs. Wilma and Mr. Dale Johnson; Mrs. Charlotte and Mr. Jerry Golinvaux Family Fund; the Roehl Family Foundation; the Joseph Durda Foundation. The generous gifts of these donors to the Minneapolis Heart Institute Foundation’s Science Center for Coronary Artery Disease (CCAD) helped support this research project.
Disclosures: Dr Hall receives speaker honoraria from Medtronic, OpSens Medical, and the Cardiovascular Innovations Foundation. Dr Seto receives research grants from Philips and ACIST; honoraria from Getinge, General Electric, and Terumo; and holds equity in Frond Medical. Dr Shah serves on advisory boards for Philips Volcano and Horizon Therapeutics and is a consultant for Terumo Medical. Dr Choi serves on the Medtronic advisory board. Dr Garcia receives institutional research grants from Edwards Lifesciences, Abbott Vascular, BSCI, and Biotronik; is a consultant for NeoChord, Medtronic, BSCI, and Abbott Vascular; and is a proctor for Edwards Lifesciences. Dr Brilakis receives consulting/speaker honoraria from Abbott Vascular, the American Heart Association (associate editor, Circulation), Amgen, Asahi Intecc, Biotronik, Boston Scientific, Cardiovascular Innovations Foundation (Board of Directors), CSI, Elsevier, GE Healthcare, IMDS, Medicure, Medtronic, Siemens, Teleflex, and Terumo; research support from Boston Scientific, GE Healthcare; is the owner of Hippocrates LLC; and is a shareholder in MHI Ventures, Cleerly Health, and Stallion Medical.
Address for correspondence: Emmanouil S. Brilakis, MD, PhD, Minneapolis Heart Institute, 920 E 28th Street #300, Minneapolis, MN 55407, USA. Email: esbrilakis@gmail.com.
References
1. Gomez LE, Bernet P. Diversity improves performance and outcomes. J Natl Med Assoc. 2019;111(4):383-392. doi:10.1016/j.jnma.2019.01.006
2. Colleges AoAM. 2022 Physician Specialty Data Report. 2023. Accessed July 10, 2023. https://www.aamc.org/data-reports/data/2022-physician-specialty-data-report-executive-summary
3. Burgess S, Shaw E, Ellenberger K, Thomas L, Grines C, Zaman S. Women in medicine: addressing the gender gap in interventional cardiology. J Am Coll Cardiol. 2018;72(21):2663-2667. doi:10.1016/j.jacc.2018.08.2198
4. Buchanan GL, Paradies V, Karam N, et al. Overcoming professional barriers encountered by women in interventional cardiology: an EAPCI statement. Eur Heart J. 2023;44(15):1301-1312. doi:10.1093/eurheartj/ehad053
5. Sharma G, Douglas PS, Hayes SN, et al. Global prevalence and impact of hostility, discrimination, and harassment in the cardiology workplace. J Am Coll Cardiol. 2021;77(19):2398-2409. doi:10.1016/j.jacc.2021.03.301
6. Yong CM, Abnousi F, Rzeszut AK, et al; American College of Cardiology Women in Cardiology Leadership Council (ACC WIC); Society for Cardiovascular Angiography and Interventions Women in Innovations (SCAI WIN). Sex differences in the pursuit of interventional cardiology as a subspecialty among cardiovascular fellows-in-training. JACC Cardiovasc Interv. 2019;12(3):219-228. doi:10.1016/j.jcin.2018.09.036
7. Harris PA, Taylor R, Minor BL, et al; REDCap Consortium. The REDCap consortium: building an international community of software platform partners. J Biomed Inform. 2019;95:103208. doi:10.1016/j.jbi.2019.103208
8. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N and Conde JG. Research electronic data capture (REDCap)--a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(2):377-381. doi:10.1016/j.jbi.2008.08.010
9. Capranzano P, Kunadian V, Mauri J, et al. Motivations for and barriers to choosing an interventional cardiology career path: results from the EAPCI Women Committee worldwide survey. EuroIntervention. 2016;12(1):53-59. doi:10.4244/EIJY15M07_03
10. Bernelli C, Cerrato E, Ortega R, et al. Gender issues in Italian catheterization laboratories: the Gender-CATH study. J Am Heart Assoc. 2021;10(5):e017537. doi:10.1161/JAHA.120.017537
11. Sarma AA, Nkonde-Price C, Gulati M, Duvernoy CS, Lewis SJ, Wood MJ; American College of Cardiology Women in Cardiology Leadership Council. Cardiovascular medicine and society: the pregnant cardiologist. J Am Coll Cardiol. 2017;69(1):92-101. doi:10.1016/j.jacc.2016.09.978
12. Dyrbye LN, West CP, Sinsky CA, et al. Physicians' experiences with mistreatment and discrimination by patients, families, and visitors and association with burnout. JAMA Netw Open. 2022;5(5):e2213080. doi:10.1001/jamanetworkopen.2022.13080
13. Cooper LA, Roter DL, Johnson RL, Ford DE, Steinwachs DM, Powe NR. Patient-centered communication, ratings of care, and concordance of patient and physician race. Ann Intern Med. 2003;139(11):907-915. doi:10.7326/0003-4819-139-11-200312020-00009
14. Javed Z, Haisum Maqsood M, Yahya T, et al. Race, racism, and cardiovascular health: applying a social determinants of health framework to racial/ethnic disparities in cardiovascular disease. Circ Cardiovasc Qual Outcomes. 2022;15(1):e007917. doi:10.1161/CIRCOUTCOMES.121.007917
15. National Academies of Sciences E, Medicine, Policy, Global A, Committee on Women in Science E, Medicine, Committee on Improving the Representation of W, Underrepresented Minorities in Clinical T and Research. The National Academies Collection: Reports funded by National Institutes of Health. In: K. Bibbins-Domingo and A. Helman, eds. Improving Representation in Clinical Trials and Research: Building Research Equity for Women and Underrepresented Groups. National Academies Press (US); 2022:23-46.
16. Saha S, Guiton G, Wimmers PF, Wilkerson L. Student body racial and ethnic composition and diversity-related outcomes in US medical schools. JAMA. 2008;300(10):1135-1145. doi:10.1001/jama.300.10.1135
17. Filut A, Alvarez M, Carnes M. Discrimination toward physicians of color: a systematic review. J Natl Med Assoc. 2020;112(2):117-140. doi:10.1016/j.jnma.2020.02.008
18. Williams DR. Race, socioeconomic status, and health. The added effects of racism and discrimination. Ann N Y Acad Sci. 1999;896:173-188. doi:10.1111/j.1749-6632.1999.tb08114.x
19. Thomas KL, Mehta LS, Rzeszut AK, Lewis SJ, Duvernoy CS, Douglas PS; ACC Diversity & Inclusion Task Force and ACC Women in Cardiology Section. Perspectives of racially and ethnically diverse U.S. cardiologists: insights from the ACC professional life survey. J Am Coll Cardiol. 2021;78(17):1746-1750. doi:10.1016/j.jacc.2021.09.002
20. Baquiran CLC, Nicoladis E. A doctor's foreign accent affects perceptions of competence. Health Communication. 2020;35(6):726-730. doi:10.1080/10410236.2019.1584779
21. Dover TL, Kaiser CR, Major B. Mixed signals: the unintended effects of diversity initiatives. 2020;14(1):152-181.doi:10.1111/sipr.12059
22. FitzGerald C, Martin A, Berner D, Hurst S. Interventions designed to reduce implicit prejudices and implicit stereotypes in real world contexts: a systematic review. BMC psychology. 2019;7:29. doi:10.1186/s40359-019-0299-7











