

Real-World Multicenter Coronary Lithotripsy Registry: Long-Term Clinical Follow-Up
Abstract
Objectives. Coronary lithotripsy (CL) works by fracturing the calcified plaque, allowing mean area gain, enhancing vessel compliance, and facilitating stent deployment. This study reports the safety, effectiveness, and durability of the clinical benefit of CL at long-term follow-up of a real-world multicenter registry. Methods. This was a prospective, multicenter, single-arm study that included consecutive patients with calcified lesions undergoing CL from August, 2018 to October, 2020 with a clinical follow-up of 20 months (interquartile range, 14.5-25). Exclusion criteria were a target lesion located in a vessel <2.5 mm and/or the presence of dissection prior to CL. The primary endpoint was the rate of major adverse cardiovascular event (MACE, defined as death or target-lesion revascularization [TLR] or myocardial infarction [MI]) at follow-up. Results. This registry included 109 patients (128 lesions). The population was elderly (mean age, 74 years old), with high rates of diabetic patients (58%), renal insufficiency (32%), and multivessel disease (76%). Most of the lesions were predilated with semicompliant/noncompliant balloons (25 with cutting balloon). Rotational atherectomy was used in 20 lesions. On average, CL required the use of 1 balloon delivering a mean of 60 pulses. Twelve patients presented with ST-segment-elevation MI and a culprit calcified coronary lesion undergoing CL. Successful CL was achieved in 99% of cases. There were few procedural complications, with 30-day freedom from MACE rate of 98%. The MACE rate at long-term follow-up was 5.6%. Conclusion. This is the first real-world, multicenter registry that confirms the safety and long-term efficacy of percutaneous coronary intervention for calcified lesions using CL in an unselected and high-risk population with a low long-term follow-up MACE rate.
J INVASIVE CARDIOL 2022;34(10):E701-E708. Epub 2022 August 30.
Key words: coronary calcified lesions, coronary lithotripsy, intravascular lithotripsy balloon, long-term clinical follow-up
Despite large advancements in percutaneous coronary intervention (PCI) throughout the last several years, coronary calcification is still a leading cause of PCI complexity and is associated with worse clinical outcomes.1 Advancing age and multiple comorbidities, such as diabetes mellitus, hypertension, chronic kidney disease, and peripheral artery disease, are associated with an increased prevalence of coronary calcium and its severity.2,3 Pooled analysis of the ACUITY and HORIZONS AMI trials demonstrated increased ischemia-driven target-lesion revascularization (TLR) at 1 year in patients with moderate and severe calcification.1 This coronary calcification may impede stent delivery and deployment, affect drug-elution kinetics, and impact suitable stent expansion and apposition, which increases the risk of stent failure.1
Currently, available techniques to prepare calcified coronary lesions before stenting can be divided into 2 groups: (1) atherectomy devices; and (2) balloon-based systems.4 Coronary lithotripsy (CL) is a balloon-based system that works by transmitting sonic waves in pulses to fracture the calcified plaque, thus allowing mean area gain, enhancing vessel compliance, and facilitating stent expansion and apposition.5-7 The combination of its short learning curve and its effect on deeper calcium than other plaque-modification devices may result in CL becoming the standard approach for treating calcified coronary lesions.7 Notably, the severity of endoluminal coronary calcium might be underestimated by coronary angiography or fluoroscopy; thus, intravascular imaging techniques are frequently required to achieve a precise evaluation of features such as calcium depth, length, and circumference, as well as fracturing results.8
Coronary lithotripsy has been evaluated in relatively small single-arm and nonrandomized studies, which have shown high rates of procedural success with promising early results, providing some insight into the mechanism of calcium modification.6,7,9-12 The Disrupt studies—CAD I,6 Disrupt CAD II,7 and Disrupt CAD III10,11—reported high device success rates with low complication rates in selected populations from the United States and Europe. Furthermore, the Disrupt CAD III study10,11 is the largest multicenter registry to date that has demonstrated the safety and effectiveness of this technique for the treatment of calcified coronary lesions at short-term follow-up. Similarly, the Disrupt CAD IV study12 showed a high procedural success rate with low complications in a Japanese population.
Currently, there are no data available on long-term clinical follow-up of patients undergoing CL. The aim of this study was to provide additional information on the safety, effectiveness, and durability of the clinical benefit of CL by reporting the long-term clinical follow-up results of a real-world, multicenter registry of an unselected high-risk population.
Methods
Study design and patients. This real-world registry was a prospective, multicenter, single-arm study that included 109 consecutive patients with a total of 128 calcified coronary lesions suitable for PCI and treated with the Shockwave Coronary IVL System (Shockwave Medical, Inc) from August, 2018 to October, 2020 with a clinical follow-up of 20 months (interquartile range [IQR], 14.5-25).
Participants were enrolled from 5 university centers in a single country. The inclusion criteria were: patients >18 years old; severe stenosis that induced ischemia with symptoms (≥50% diameter stenosis assessed by quantitative coronary angiography); and a severe calcified coronary lesion in vessels with diameter ≥2.5 mm. The exclusion criteria consisted of a target lesion in a small vessel (diameter <2.5 mm) and/or the presence of coronary dissection (> type B) before undergoing CL.
This study was conducted according to the provisions of the Declaration of Helsinki, ISO 14155, and clinical practice guidelines. The study protocol was approved by the ethics committee and complies with the institutional review board requirements. All patients provided written informed consent. Data at baseline and during follow-up were collected through an electronic case report form (e-CRF).
Study endpoints and definitions. The main study objective was to provide the safety, effectiveness, and long-term durability of the clinical benefit of CL for the treatment of calcified lesions by reporting long-term clinical outcomes from an unselected and high-risk population.
The primary endpoint was defined as a composite of the cumulative incidence of cardiovascular death, myocardial infarction, and target-lesion revascularization (TLR) at 1-year follow-up after the index admission in which CL was applied. The secondary endpoints were the clinical success rate of the procedure (residual stenosis <50%) without periprocedural complications and the incidence of in-hospital complications including coronary dissection, persistent slow-flow/no-reflow, coronary perforation, myocardial infarction, stroke, bleeding events, and death.
The clinical and angiographic endpoints followed the definitions of the Academic Research Consortium (ARC)-2 recommendations.13 CL success was defined as the successful deployment of the stent with a residual diameter stenosis <50%. Bleeding (as safety endpoint) was defined following the Bleeding Academic Research Consortium (BARC);14 BARC types 3–5 were considered major bleedings.
Major adverse cardiac event (MACE) was defined as cardiac death, myocardial infarction, or target-vessel revascularization (TVR).6 TLR was defined as repeat PCI to treat the same lesion treated during the index procedure. TVR was defined as PCI of a new severe lesion at another location other than the segment vessel treated at the index PCI. Non-TVR was defined as PCI of a different vessel treated at the index procedure. Target-lesion failure was defined as the composite of clinically-driven TLR, myocardial infarction, or cardiac death related to the target vessel.15
Study device and procedures. All coronary calcified lesions were treated with the Shockwave Coronary IVL System. A complete description of the study device is available in our previously published manuscript.9 Briefly, the IVL balloon is a rapid-exchange balloon catheter with emitters that generate sonic waves to crack the calcium and to improve vessel compliance. The implantation of a drug-eluting stent (DES) is then performed at the discretion of the operator along with high-pressure (>16 atm) postdilation. Dual-antiplatelet therapy is administered following the established clinical practice guidelines. The concomitant use of other plaque-modification devices, such as rotational atherectomy or cutting balloon, was allowed in the presence of heavy calcium and at the operator’s discretion.
Statistical analysis. Continuous variables are shown as mean ± standard deviation or median (IQR). Categorical variables are expressed as frequencies and group percentages. Statistical analysis was performed using STATA software, version 16.0 (StataCorp).
Results
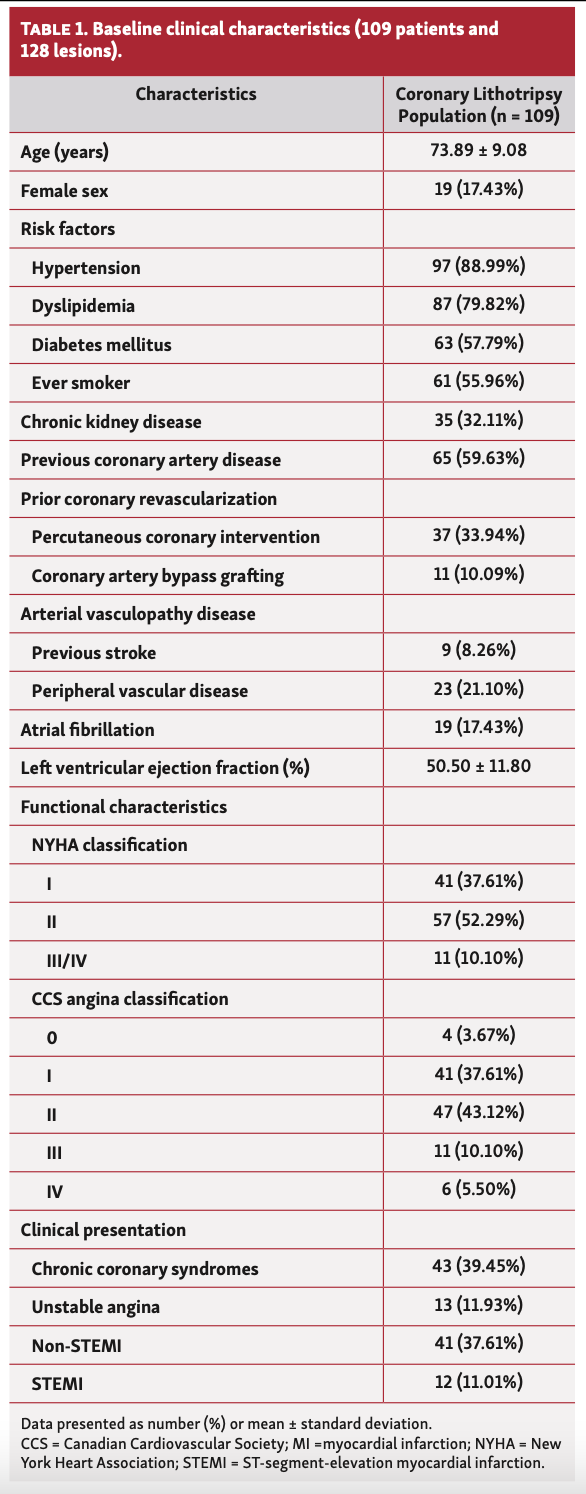
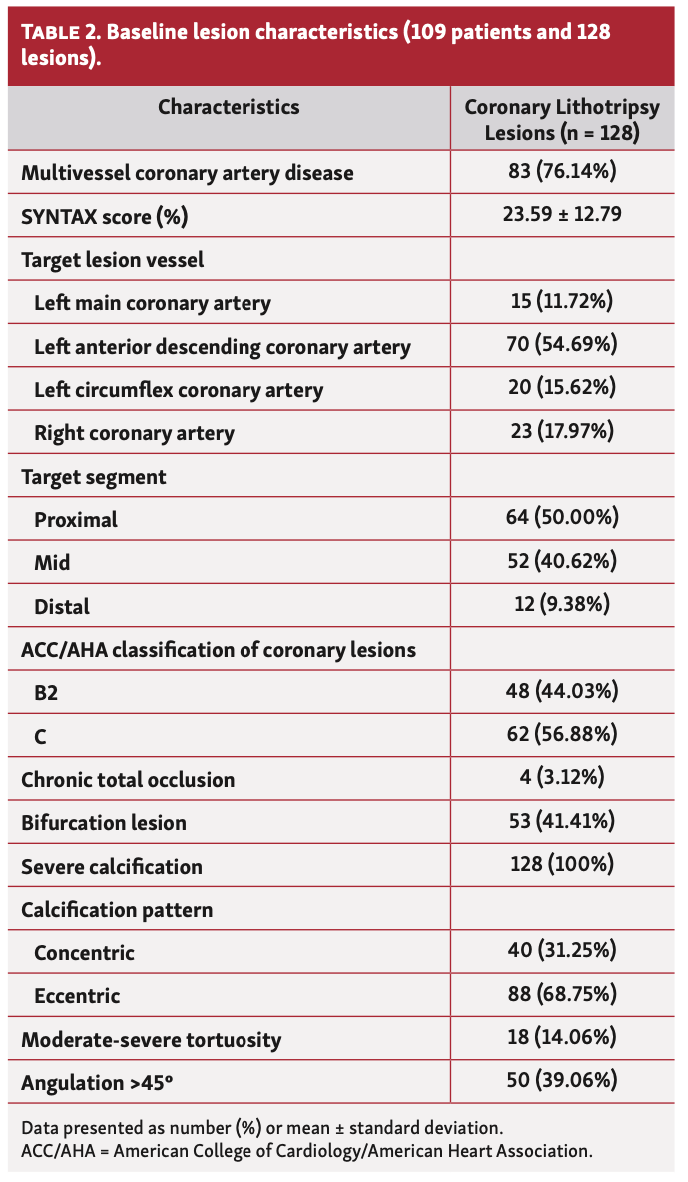
The present study enrolled a total of 109 patients with 128 severely calcified coronary lesions that were treated with the Shockwave Coronary IVL System from August, 2018 to October, 2020. The baseline clinical and angiographic characteristics are presented in Table 1 and Table 2. The study population included a relatively advanced age (73.9 ± 9.4 years). Most patients (83%) were male and presented a high prevalence of cardiovascular risk factors: hypertension (89%); dyslipidemia (80%); diabetes mellitus (58%); and chronic kidney disease (32%). Notably, a large percentage of patients had prior coronary artery disease (60%) with a significant proportion of previous revascularization (44%). Multivessel disease was found in a high percentage of patients (76%). The target lesion most frequently treated with IVL balloon was the left anterior descending coronary artery (55%). Half of target lesions were located at the proximal artery segment and the mean lesion length was 23 mm. The IVL balloon was used in 15 left main coronary artery lesions and in 53 bifurcated lesions (41%). Severely calcified lesions were present in all patients and were classified as type B2 (44%) and C (57%) according to American College of Cardiology/American Heart Association classification. Twelve patients presented with ST-segment-elevation myocardial infarction (STEMI) and a culprit calcified coronary lesion that underwent CL.
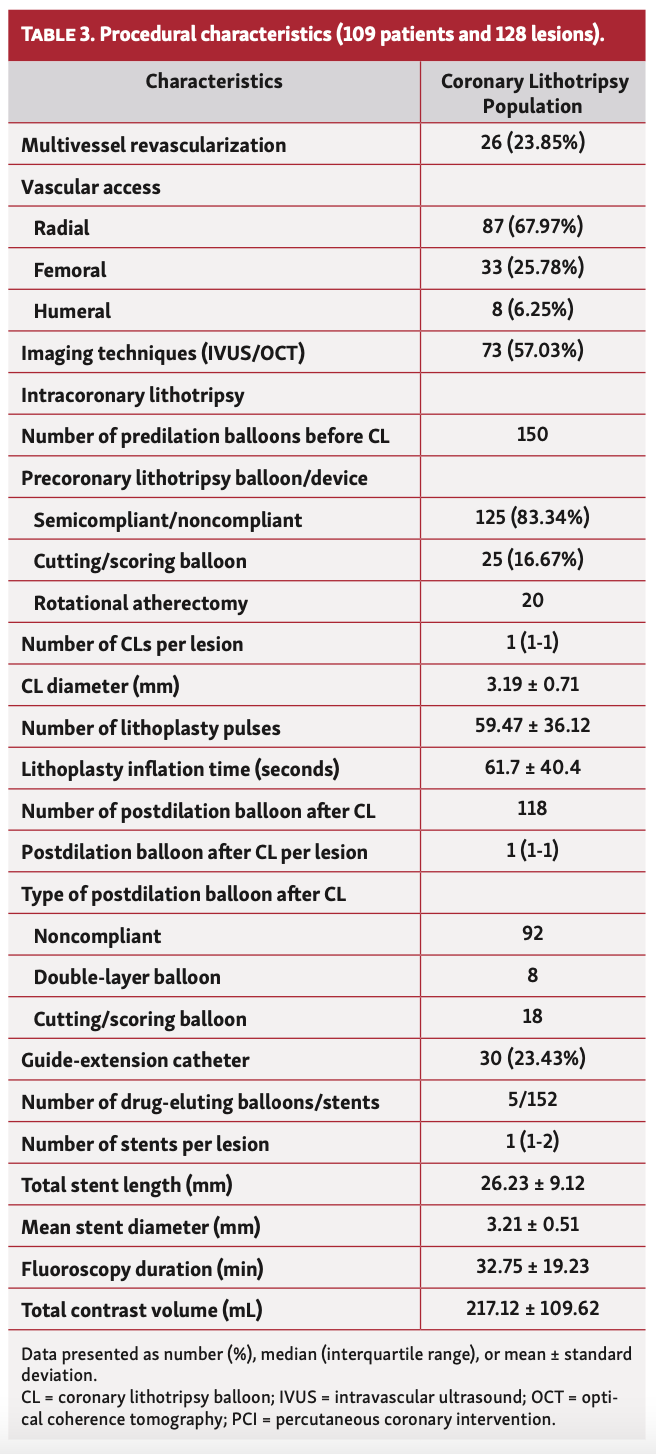
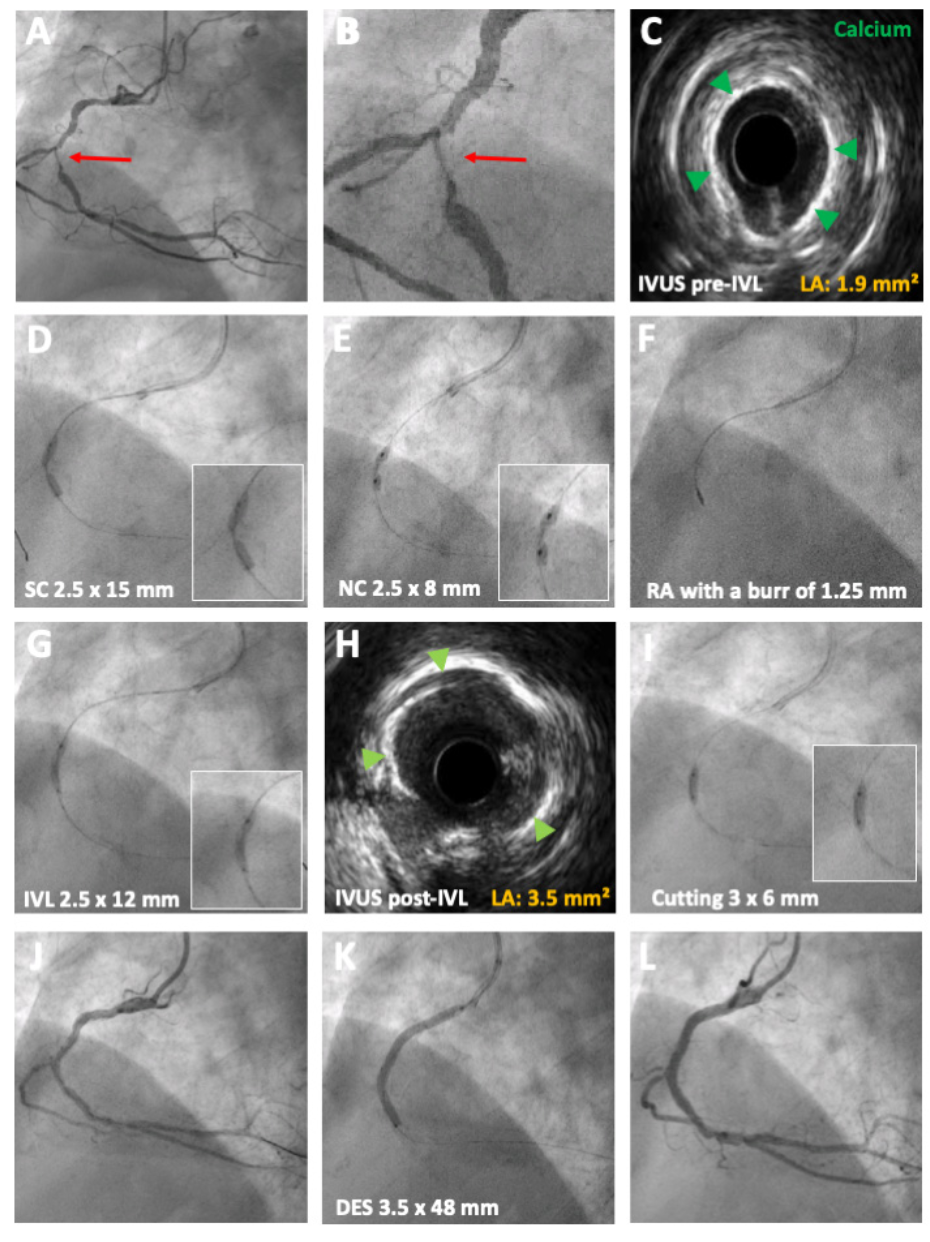
The procedural characteristics are summarized in Table 3. Thirty percent of patients underwent multivessel revascularization. The most common vascular access was radial (68%). The target calcified lesion was predilated with semicompliant/noncompliant balloons in 21% of cases before the use of CL. Of note, the concomitant use of other plaque-modification devices was performed using cutting balloon in 25 cases and rotational atherectomy in 20 cases (Figure 1). A catheter extender was used to deliver the IVL balloon into the lesion in 23%. The IVL balloon was successfully delivered in all target lesions. CL was performed with the use of 1 IVL balloon (range, 1-1) delivering on average 4 therapies (range, 3.5-5) with a mean of 59 pulses. A total of 10 IVL balloons were fissured during therapy application without any associated complications.
CL was successfully achieved in 99% of cases. There was 1 case without achieving <50% of residual diameter stenosis after the complete application of 2 IVL balloons and the additional use of cutting balloon; this patient was then treated with a drug-eluting balloon. Average number of stents per lesion was 1 (range, 1-2), mean stent diameter was 3.2 ± 0.5 mm, and mean total stent length was 26.2 ± 9.1 mm.
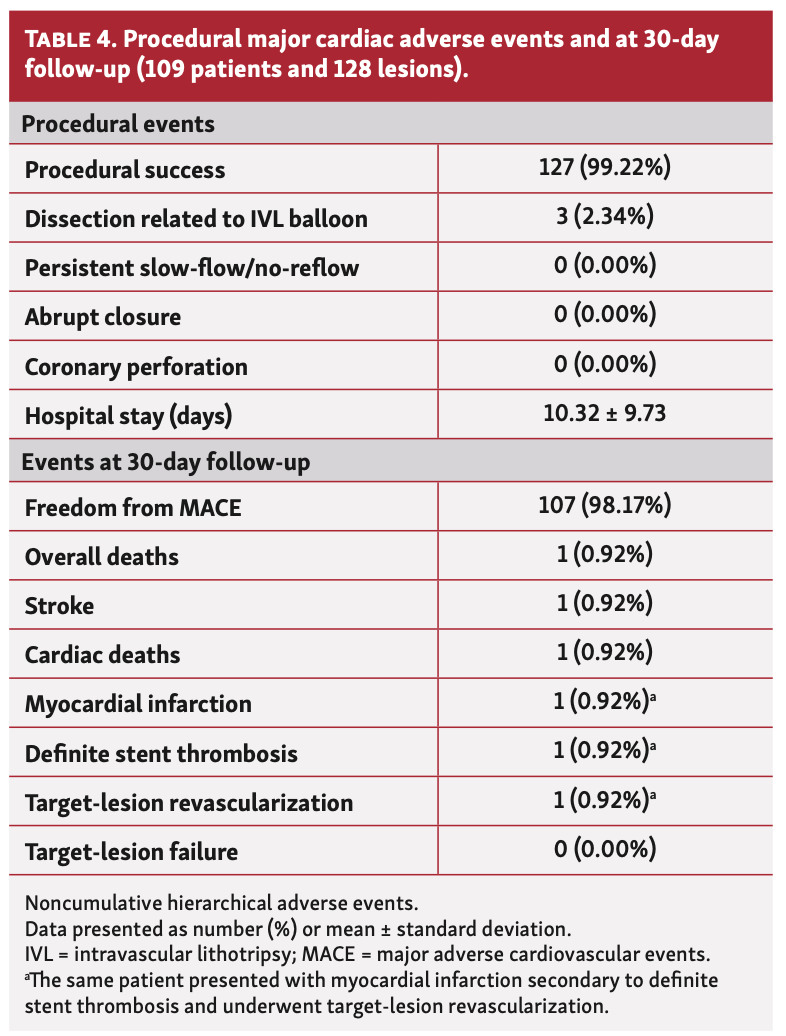
In-hospital clinical results and 30-day follow-up. Procedural and clinical events at 1-month follow-up are listed in Table 4. During the procedure, there were 3 dissection related to IVL balloon, which were resolved with the implantation of 1 drug-eluting stent. There were no reports of slow-flow/no-reflow, perforation, or target-lesion failure. There was 1 patient who presented with a stroke during the hospital stay. There was 1 cardiac death, but it was unrelated to the procedure. From the overall population, 30-day ischemia-driven TVR rate was 0.92%, consisting of 1 patient with definite stent thrombosis presenting as STEMI 48 hours after CL due to a slight malapposition of the proximal edge of the stent as assessed by optical coherence tomography; the patient underwent primary PCI and successful TLR. There were no other MACEs.
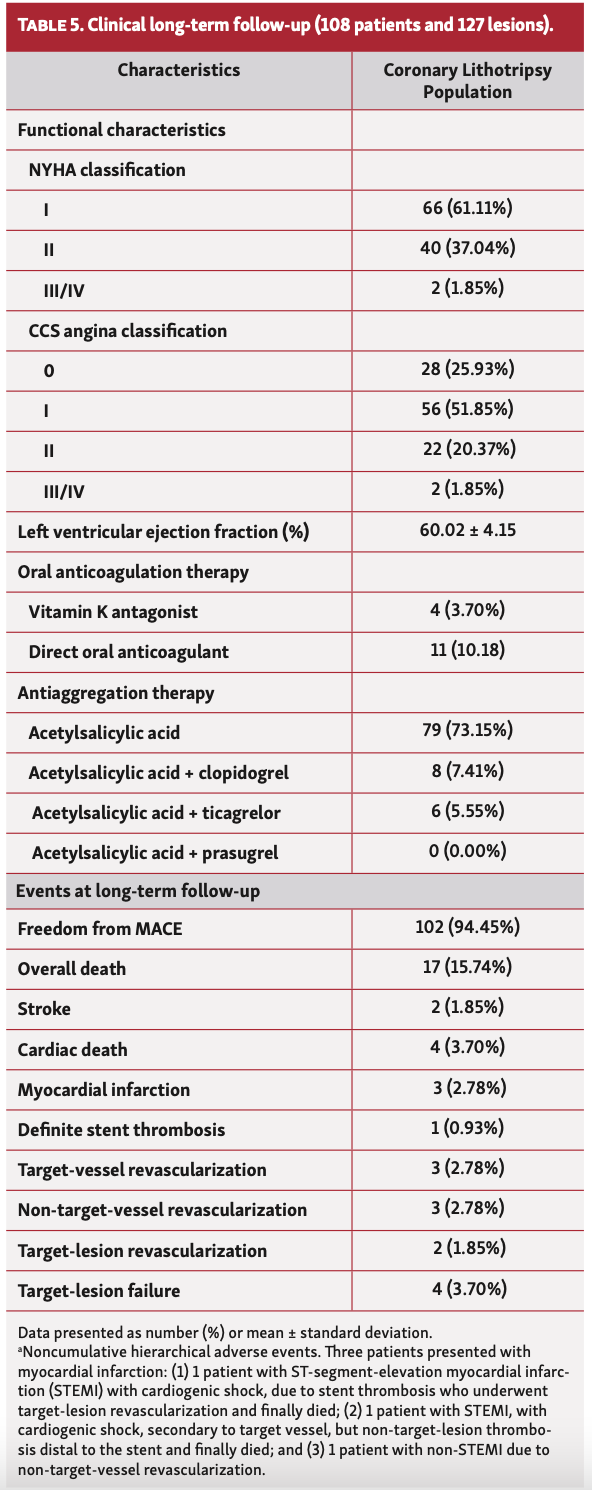
Long-term follow-up. Clinical characteristics and events at >1-year follow-up (20 months [IQR, 14.5-25]) are presented in Table 5. Most of patients were in Canadian Cardiovascular Society angina class 0-I (78%). Notably, mean left ventricular ejection fraction improved at long-term clinical follow-up (60%). At follow-up, most patients (73%) were on single-antiplatelet therapy. Fifteen patients, with previous diagnosis of atrial fibrillation, were only on oral anticoagulation (11 with direct oral anticoagulation).
Long-term ischemia-driven TVR rate was 2.78% (3 patients). The MACE rate was 5.6%. Two patients presented with a stroke at long-term follow-up. There was a total of 17 overall deaths (15%), 4 of which were cardiac deaths (3.7%): 1 patient with target-lesion failure due to restenosis and multivessel disease before performing coronary artery bypass graft, 1 patient who died because of a ventricular arrhythmia, 1 patient with STEMI complicated by cardiogenic shock at 2 months after the procedure who underwent TLR, and 1 patient with STEMI complicated by cardiogenic shock at 15 months after the procedure secondary to target-vessel (but non-target lesion) thrombosis distal to the stent.
There were 3 myocardial infarctions, including the 2 STEMIs previously described and 1 non-STEMI due to a lesion in a different vessel. One patient with angina of minimal effort and deterioration of left ventricular ejection fraction underwent coronary angiography that showed in-stent restenosis of the left anterior descending coronary artery previously treated with CL undergoing TLR and PCI of a de novo lesion in the right coronary artery (non-TVR).
Discussion
This is the first report of the long-term clinical follow-up of a real-world multicenter CL registry, which demonstrates the safety, effectiveness, and durability of the clinical benefit of the CL for treating calcified lesions by reporting long-term clinical outcomes of an unselected and high-risk population. The major findings of this study are: (1) the long-term MACE rate in this unselected and high-risk population with complex anatomy undergoing CL was notably low and similar compared with the outcomes of historical stent registries, and lower in comparison with previous plaque-modification studies in this difficult-to-treat population; (2) the rate of clinical success of CL was high, with a remarkably low rate of in-hospital and 30-day complications; (3) the IVL balloon, which facilitates stent implantation in calcified coronary lesions, resulted in improved CCS angina class; (4) CL seems safe and effective in specific clinical scenarios, such as STEMI with a culprit calcified coronary lesion; and (5) the IVL balloon demonstrates the durability of the clinical benefit of its concomitant use with other plaque-modification devices (cutting balloon and rotational atherectomy).
Short-term results: 30-day follow-up. Severe coronary calcium is a strong predictor of MACE after PCI.1 The main dedicated tools that are available to treat calcified coronary lesion before stent implantation are rotational and orbital atherectomy.16,17 However, their use remains limited due to the long and demanding learning curve associated to become proficient with them and the relatively high procedural complication rate. Of note, these established plaque-modification tools have shown a high MACE rate at follow-up.16-18 The ORBIT II study,17 which included 443 patients with calcified coronary lesion undergoing orbital atherectomy followed by stent implantation, showed a MACE rate of 10% at 30 days. The European multicenter Euro4C registry,19 which included 966 patients undergoing rotational atherectomy followed by stenting, showed a 30-day MACE rate of 5.6%.
Coronary lithotripsy has been successfully proven for the management of calcified lesions.6,7,9-13 The first study to demonstrate the feasibility of CL was Disrupt CAD I,6 which included 60 patients with a procedural success rate of 98.5% and a freedom from MACE rate of 95% at 30 days. The Disrupt CAD II study,7 which included 120 patients, was a prospective postmarket study designed to determine the management of CL in a real-world population and showed a procedural success rate of 100% and a freedom from in-hospital MACE rate of 94.2%. The Disrupt CAD III study,10 which was designed for United States regulatory approval and included 431 patients, showed a procedural success rate of 92.4% and a freedom from MACE rate of 92.2% at 30 days. The Disrupt IV study,12 which included 64 patients from Japan, showed a procedural success rate of 93.8% and a freedom from MACE rate of 93.8% at 30 days. All of these studies were single-arm, prospective, multicenter, and nonrandomized trials that demonstrated high rates of procedural success and promising early results.6,7,9-13 Despite the unselected and high-risk population and inclusion of non-de novo lesions, our results at 30 days support the findings of Disrupt CAD I,6 II,7 III,10 and IV,12 showing a procedural success rate of 99% and a freedom from MACE rate of 98% at 30 days.
In addition, our study shows the safety of the concomitant use of other plaque-modification devices, such as cutting balloon and rotational atherectomy. The present registry included 15 calcified coronary lesions affecting the left main coronary artery that were successfully treated with CL and 12 patients with STEMI and a culprit calcified coronary lesion successfully treated with IVL balloon during the primary angioplasty procedure.
Long-term results: >1-year follow-up. The Disrupt CAD studies I,6 II,7 III10 and IV;12 as well as our previous published study,9 which included 57 patients (67 lesions) treated with IVL balloon, have all demonstrated high rates of procedural success and excellent in-hospital and short-term follow-up results. However, there are no data available about long-term clinical follow-up of patients undergoing CL. The present study is the first report of the long-term clinical follow-up of a real-world, unselected, and high-risk population that underwent CL.
Regarding clinical long-term outcomes of other plaque-modification devices such as rotational atherectomy, data from the European multicenter Euro4C registry,19 which included 966 patients from 8 European countries undergoing rotational atherectomy, showed a MACE rate (defined as cardiovascular death, myocardial infarction, stroke, TLR, or coronary artery bypass graft surgery) of 13.2% at 1-year follow-up. The rate of all-cause death was 9.7% and the cardiac death rate was 5.7%, with a TLR rate of 2.4% at 1-year follow-up.
A meta-analysis that pooled 18,441 patients (18 trials) with calcified coronary lesions treated with drug-eluting stent implantation reported a 1-year MACE rate of 9.4% for patients without diabetes and 13.9% for patients with diabetes.20 It is noteworthy that these outcomes agree with prior registries focused on rotational atherectomy (with 1-year MACE rates from 13.2%-21.6%).19,21-23
Our results at long-term follow-up at a median of 20 months (IQR, 14.5-25) confirm the safety, effectiveness, and clinical durability of CL for the treatment of calcified coronary lesions, showing remarkably lower rates of MACE (5.6%), cardiac death (3.7%), and TLR (1.85%). The rate of all-cause death was 15%, which probably reflects the aging and high-risk level of patients rather than the CL technique itself.
Our long-term results with the use of CL showed a relevant improvement regarding MACE rates from studies that used an atherectomy technique. CL seems to be a safe tool, with a low rate of TLR at long-term follow-up; thus, the initial trauma inflicted to the vessel wall while emitting acoustic pressure to fracture calcium may not have a significant repercussion on restenosis (clinically-driven TLR).
Study limitations. This was an observational study, not a randomized controlled trial, with the absence of a comparison group and self-reported events. This study shows the long-term follow-up from a real-world, unselected, and high-risk population. The present study included specific clinical presentations, such as STEMI, and the concomitant use of other plaque-modification techniques, such as rotational atherectomy and cutting balloon; thus, further investigation is needed to understand the potential use of this user-friendly device. Routine systematic quantitative coronary angiography analysis, intravascular ultrasound, and optical coherence tomography were not performed. Finally, there was no systematic angiographic control at long-term follow-up due to most patients remaining asymptomatic.
Conclusion
This is the first real-world multicenter registry to confirm the feasibility, safety, and long-term efficacy of PCI for calcified lesions using CL in an unselected and high-risk population with a remarkable low MACE rate at long-term follow-up. In addition, the present study supports the safe use of CL in specific clinical scenarios, such as STEMI, and demonstrates the durability of the clinical benefit of the concomitant use of other plaque-modification techniques with the IVL balloon.
Affiliations and Disclosures
From 1the Interventional Cardiology Unit, Department of Cardiology, Hospital del Mar, Barcelona, Spain; 2Heart Diseases Biomedical Research Group, Hospital del Mar Medical Research Institute-IMIM, Barcelona, Spain; 3Heart Diseases Institute, Hospital de Bellvitge, Instituto de Investigación Biomédica de Bellvitge-(IDIBELL), University of Barcelona, Barcelona, Spain; 4Interventional Cardiology Unit, Department of Cardiology, Hospital Clínico Universitario de Valladolid, Instituto de Ciencias del Corazón (ICICOR), Spain; 5Interventional Cardiology Unit, Department of Cardiology, Hospital Universitario Joan XXIII University Rovira Virgili, Tarragona, Spain; 6Heart Area, Hospital Universitario Central de Asturias, Instituto de Investigación Sanitaria del Principado de Asturias (ISPA), Oviedo, Spain, University of Oviedo, Spain; and 7Autonomous University of Barcelona, Barcelona, Spain.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
The authors report that patient consent was provided for publication of the images used herein.
Manuscript accepted March 17, 2022.
Address for correspondence: Hector Cubero-Gallego, MD, PhD, Hospital del Mar (Parc de Salut Mar), Passeig Maritim 25-29, 08003 Barcelona, Spain. Email: hektorkubero@hotmail.com
References
1. Généreux P, Madhavan MV, Mintz GS, et al. Ischemic outcomes after coronary intervention of calcified vessels in acute coronary syndromes. Pooled analysis from the HORIZONS-AMI (Harmonizing Outcomes With Revascularization and Stents in Acute Myocardial Infarction) and ACUITY (Acute Catheterization and Urgent Intervention Triage Strategy) trials. J Am Coll Cardiol. 2014;63(18):1845-1854. Epub 2014 Feb 19. doi:10.1016/j.jacc.2014.01.034
2. Bourantas CV, Zhang YJ, Garg S, et al. Prognostic implications of coronary calcification in patients with obstructive coronary artery disease treated by percutaneous coronary intervention: a patient-level pooled analysis of 7 contemporary stent trials. Heart. 2014;100(15):1158-1164. Epub 2014 May 20. doi:10.1136/heartjnl-2013-305180
3. Madhavan MV, Tarigopula M, Mintz GS, et al. Coronary artery calcification: pathogenesis and prognostic implications. J Am Coll Cardiol. 2014;63(17):1703-1714. Epub 2014 Feb 12. doi:10.1016/j.jacc.2014.01.017
4. De Silva K, Roy J, Webb I, et al. A calcific, undilatable stenosis: lithoplasty, a new tool in the box? JACC Cardiovasc Interv. 2017;10(3):304-306. doi:10.1016/j.jcin.2016.11.048
5. Ali ZA, Brinton TJ, Hill JM, et al. Optical coherence tomography characterization of coronary lithoplasty for treatment of calcified lesions: first description. JACC Cardiovasc Imaging. 2017;10(8):897-906. doi:10.1016/j.jcmg.2017.05.012
6. Brinton TJ, Ali ZA, Hill JM, et al. Feasibility of shockwave coronary intravascular lithotripsy for the treatment of calcified coronary stenoses. Circulation. 2019;139(6):834-836. doi:10.1161/CIRCULATIONAHA.118.036531
7. Ali ZA, Nef H, Escaned J, et al. Safety and effectiveness of coronary intravascular lithotripsy for treatment of severely calcified coronary stenosis. Circ Cardiovasc Interv. 2019;12(10):e008434. Epub 2019 Sep 25. doi:10.1161/CIRCINTERVENTIONS.119.008434
8. Wang X, Matsumura M, Mintz GS, et al. In vivo calcium detection by comparing optical coherence tomography, intravascular ultrasound, and angiography. JACC Cardiovasc Imaging. 2017;10(8):869-879. doi:10.1016/j.jcmg.2017.05.014.
9. Cubero-Gallego H, Millán R, Fuertes M, et al. Coronary lithoplasty for calcified lesions: real-world multicenter registry. Rev Esp Cardiol (Engl Ed). 2020;73(12):1003-1010. Epub 2020 May 17. doi:10.1016/j.rec.2020.02.010
10. Hill JM, Kereiakes DJ, Shlofmitz RA, et al. Intravascular lithotripsy for treatment of severely calcified coronary artery disease. J Am Coll Cardiol. 2020;76(22):2635-2646. Epub 2020 Oct 15. doi:10.1016/j.jacc.2020.09.603
11. Kereiakes DJ, Hill JM, Ben-Yehuda O, et al. Evaluation of safety and efficacy of coronary intravascular lithotripsy for treatment of severely calcified coronary stenoses: design and rationale for the Disrupt CAD III trial. Am Heart J. 2020;225: 10-18. Epub 2020 Apr 18. doi:10.1016/j.ahj.2020.04.005
12. Saito S, Yamazaki S, Takahashi A, et al. Intravascular lithotripsy for vessel preparation in severely calcified coronary arteries prior to stent placement—primary outcomes from the Japanese Disrupt CAD IV study. Circ J. 2021;85(6):826-833. Epub 2021 Feb 5. doi:10.1253/circj.CJ-20-1174
13. Garcia-Garcia HM, McFadden EP, Farb A, et al. Standardized end point definitions for coronary intervention trials: the Academic Research Consortium-2 Consensus Document. Circulation. 2018;137(24):2635-2650. doi:10.1161/CIRCULATIONAHA.117.029289
14. Mehran R, Rao SV, Bhatt DL, et al. Standardized bleeding definitions for cardiovascular clinical trials: a consensus report from the Bleeding Academic Research Consortium. Circulation. 2011;123(23):2736-2747. doi:10.1161/CIRCULATIONAHA.110.009449
15. Stolker JM, Cohen DJ, Kennedy DF, et al. Repeat revascularization after contemporary percutaneous coronary intervention: an evaluation of staged, target lesion, and other unplanned revascularization procedures during the first year. Circ Cardiovasc Interv. 2012;5(6):772-782. Epub 2012 Oct 23. doi:10.1161/CIRCINTERVENTIONS.111.967802
16. Abdel-Wahab M, Richardt G, Joachim Buttner H, et al. High-speed rotational atherectomy before paclitaxel-eluting stent implantation in complex calcified coronary lesions: the randomized ROTAXUS (Rotational Atherectomy Prior to Taxus Stent Treatment for Complex Native Coronary Artery Disease) trial. JACC Cardiovasc Interv. 2013;6(1):10-19. Epub 2012 Dec 19. doi:10.1016/j.jcin.2012.07.017
17. Chambers JW, Feldman RL, Himmelstein SI, et al. Pivotal trial to evaluate the safety and efficacy of the orbital atherectomy system in treating de novo, severely calcified coronary lesions (ORBIT II). JACC Cardiovasc Interv. 2014;7(5):510-518. doi:10.1016/j.jcin.2014.01.158
18. Sakakura K, Inohara T, Kohsaka S, et al. Incidence and determinants of complications in rotational atherectomy: insights from the national clinical data (J-PCI registry). Circ Cardiovasc Interv. 2016;9(11):e004278. doi:10.1161/CIRCINTERVENTIONS.116.004278
19. Bouisset F, Barbato E, Reczuch K. et al. Clinical outcomes of PCI with rotational atherectomy: the European multicentre Euro4C registry. EuroIntervention. 2020;16(4):e305-e312. doi:10.4244/EIJ-D-19-01129
20. Kedhi E, Généreux P, Palmerini T, et al. Impact of coronary lesion complexity on drug-eluting stent outcomes in patients with and without diabetes mellitus: analysis from 18 pooled randomized trials. J Am Coll Cardiol. 2014;63(20):2111-2118. Epub 2014 Mar 13. doi:10.1016/j.jacc.2014.01.064
21. Couper LT, Loane P, Andrianopoulos N, et al. Utility of rotational atherectomy and outcomes over an eight-year period. Catheter Cardiovasc Interv. 2015;86(4):626-631. Epub 2015 Jul 8. doi:10.1002/ccd.26077
22. Kawamoto H, Latib A, Ruparelia N, et al. In-hospital and midterm clinical outcomes of rotational atherectomy followed by stent implantation: the ROTATE multicentre registry. EuroIntervention. 2016;12(12):1448-1456. doi:10.4244/EIJ-D-16-00386
23. Okamoto N, Ueda H, Bhatheja S, et al. Procedural and one-year outcomes of patients treated with orbital and rotational atherectomy with mechanistic insights from optical coherence tomography. EuroIntervention. 2019;14(17):1760-1767. doi:10.4244/EIJ-D-17-01060
Related Reading
- Coronary Orbital Atherectomy in Patients With Severe Aortic Stenosis
- Endovascular eSheath Predilation to Facilitate Transfemoral Transcatheter Aortic Valve Delivery
- Coronary Caverns: Spontaneous Recanalized Chronic Total Occlusion With Multiple Microchannels
- Comparison of Different Stenting Techniques in Left Main Bifurcation Disease: Evidence From a Network Meta-Analysis












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}