


How To Treat Lesser MPJ Disorders
Podiatric physicians routinely see disorders of the forefoot, especially the lesser metatarsophalangeal joints (MPJs). In fact, they are often the presenting complaint of the patient or the reason for the medical referral. Lesser MPJ disorders can also occur as a result of preexisting conditions such as trauma, infection, faulty biomechanics and previous podiatric surgery. Unfortunately, the term metatarsalgia has been used as a catch-all term to describe a condition without a true etiology. This can be very frustrating to both the patient and the doctor. Indeed, having a firm grasp of the forefoot anatomy is essential when it comes to understanding lesser MPJ pathology. The forefoot consists of the bones and all soft tissue structures from the distal aspect of all five digits to the bases of all five metatarsals at the metatarsocuneiform/cuboid (Lisfranc’s) joint. The MPJs are composed of the articulation between the base of the proximal phalanx of each digit and each metatarsal head. These joints are described as ellipsoid joints, which are created by the rounded metatarsal heads and the shallow cavities on the base of the proximal phalanx of each toe.1 Articular cartilage covers the distal and plantar portions of the metatarsal heads. There is no articular cartilage on the dorsal surface of the metatarsal. The articular cartilage of the phalangeal bases encompasses the entire cavity of the bone. Two collateral ligaments, running from dorsal proximal to plantar distal, maintain the integrity of the MPJ. These ligaments allow sagittal dorsiflexion and plantarflexion of the proximal phalanx on the metatarsal heads but prevent excessive transverse plane motion of abduction and adduction. Minimal frontal plane motion of inversion and eversion is possible. Disruption of these ligaments causes transverse deviation of the digits as well as dorsal contraction. The fibrous capsule surrounds the joints and is relatively thin dorsally but is synonymous with the thick plantar ligaments that comprise the plantar plate. All the MPJs are connected plantarly by the deep transverse intermetatarsal ligament. The lesser MPJs are located approximately 2.5 cm proximal to the web of the digits. The amount of joint dorsiflexion of the lesser MPJs can approach 90 degrees and is necessary for the extremes of forefoot function in walking, but most importantly in sports. The lesser MPJs are at a relative 25 degrees of dorsiflexion in stance, owing to the 20- to 25-degree plantarflexion of the metatarsals in stance. Muscles associated with this area are divided into extrinsic and intrinsic muscles. The extrinsic muscles at this level are composed entirely of tendinous material. Dorsally, the extensor digitorum longus tendon passes over the lesser MPJ and divides into three slips. The central slip inserts into the base of the intermediate phalanx. The remaining two slips rejoin to insert into the base of the distal phalanx. The extensor hood is comprised of soft tissue at the joint level that connects the extensor tendon to the plantar plate. The extensor tendon does not insert into the proximal phalanx but dorsiflexes the proximal phalanx on the metatarsal head through the extensor hood mechanism. The tendons of the extensor digitorum brevis tendon attach to the long extensor tendons at the level of the second, third and fourth MPJs. Plantarly, the tendon of the flexor digitorum longus courses along the long axis of the joint and inserts into the base of the distal phalanx. The tendon of the flexor digitorum brevis inserts into the center area of the middle phalanx. This aids in plantarflexion of the proximal and distal IPJ. There is no insertion of the flexor tendons on the proximal phalanx. The interosseous muscles and lumbricales comprise the intrinsic musculature of the forefoot. The interossei insert into the base of the proximal phalanx, the plantar plate and the extensor hood. They produce abduction and adduction of the lesser MPJs. The lumbricales insert into the extensor sling apparatus and aid in stabilizing the lesser MPJs. They also facilitate dorsiflexion and plantarflexion.
Why One Should Not Overlook The Plantar Plate And Plantar Fat Pad
The plantar plate is an important structure that has gained much attention recently in the literature.2 It is composed of the plantar aponeurosis and the plantar capsule. Researchers have shown it enhances stability of the lesser MPJ with help from the intrinsic muscles. Loss of stability causes digital contractures and joint pathology. Sometimes, the plantar fat pad is overlooked in this area. Unfortunately, this becomes an important factor in pathological conditions of the forefoot. Normally, it acts as a tremendous shock absorber for walking, especially during the mid-stance and propulsive stages of gait. Atrophy and distal displacement of the fat pad add to pathological symptoms and can present a challenge in determining treatment options.
A Primer On Metabolic, Degenerative And Traumatic Pathology
Pathology of the lesser MPJs may be metabolic, degenerative and/or traumatic. Metabolic conditions include disease entities that produce acute and chronic synovitis. Over a period of time, this causes a loss of articular cartilage and resulting pain, stiffness and possible ankylosis of the joint. Other symptoms include a loss of joint motion and an altered gait. Metabolic conditions also include inflammatory diseases such as rheumatoid arthritis, psoriatic arthritis and lupus. Careful medical evaluation is essential before proceeding with treatment options. Ensuring concurrent evaluation and treatment by an internist or rheumatologist is often helpful. Bone density evaluations are usually a good idea for these patients. Treatment of the underlying disease helps to ensure a better and more predictable outcome. Repetitive microtrauma, faulty biomechanics (both congenital and iatrogenic) and chronic overuse syndromes can cause degenerative changes in the articular cartilage of the joint. Loss of articular cartilage causes stiffness, loss of motion and subsequent ankylosis of the joint. To compensate for this, people may subsequently alter their gait. This may lead to compensatory pain in other joints in the lower extremity as well as general musculoskeletal symptoms. Direct trauma to the lesser MPJs can result in a variety of presentations. Fractures, with or without dislocation, can disrupt joint stability with resulting degenerative changes as described above. Osteochondritis (Freiberg’s infraction) is considered a direct trauma pathology due to the aseptic necrosis resulting from the trauma and ischemia to the metatarsal head. Soft tissue damage from trauma can also disrupt the delicate balance and stability of the joint, leading to abnormal wear and tear. This leads to destruction of the joint.
Weighing The Different Treatment Options
Certainly, one should initially pursue conservative treatment for the aforementioned conditions. (The only exception would be in the face of severe damage to the joint by trauma.) Conservative treatment options include rest, immobilization, shoe modifications, orthoses, ice, heat, physical therapy, steroid injections and NSAIDs (COX-1 or COX-2 inhibitors). When conservative treatment fails, one must choose an appropriate surgical procedure for the patient. Surgeons should ensure that they are on the same page as their patients when it comes to expectations of the given procedure. With this in mind, let us consider the available surgical options for the lesser MPJ. • Arthroplasty with resection of the base of the proximal phalanx. Arthroplasty is an accepted method of treatment. However, one should be aware of potential complications including: floppy toe; weight imbalance transfer causing lesser metatarsalgia and possible plantar lesions; and stress fractures of the affected metatarsal. Syndactylization helps to some degree with the floppiness but many patients are concerned with the cosmetic result. • Metatarsal head resection. This is not the best choice for many of the same reasons. This procedure destroys the fine stability of the lesser MPJ and one more frequently sees transfer lesions with this procedure. When these transfer lesions occur, the surgeon has to resort to “chasing” metatarsal heads for future surgical balancing of the metatarsal parabola. • Arthrodesis. Arthrodesis of the lesser MPJ completely destroys the soft tissue balance around the joint. More importantly, the patient will never be able to dorsiflex the joint after undergoing this procedure. This will limit the motion of the forefoot especially in toe-off during the gait cycle. Lesser metatarsalgia as well as other compensatory symptoms are most likely to occur. Also keep in mind there is a longer postoperative course. The possibility of a delayed or non-union would further complicate the procedure, extending the disability and subsequent postoperative period. These patients will also need special modifications to their shoes.
Why Joint Replacement Is The Best Surgical Option
• Joint replacement. Joint replacement is the treatment of choice. Recent advancements in the design and materials for this procedure facilitate a less complicated post-op recovery and a quicker return to normal activity. To perform this procedure correctly, one would resect minimal bone and maintain the soft tissue integrity around the joint. Doing so allows the return of a normal range of motion postoperatively. Previous implant designs were double stemmed and made of a silicon polymer.3-5 These implants failed due to design and material selection. With these implants, one achieved motion at the stems and not the hinge. The tissue reaction and greater bone resection caused less than optimal results. Researchers have shown that metal implants that replace only the articular cartilage of the phalanx base produce more reproducible results and better satisfaction.6 The implant I prefer to use is made of a cobalt-chromium alloy, which has a very low co-efficient of friction with minimal tissue reactivity. It is modeled almost exactly (except for size) to another implant for the first MPJ, which has good results over time and good patient satisfaction as documented in the literature.7
A Guide To Joint Replacement For Lesser MPJs
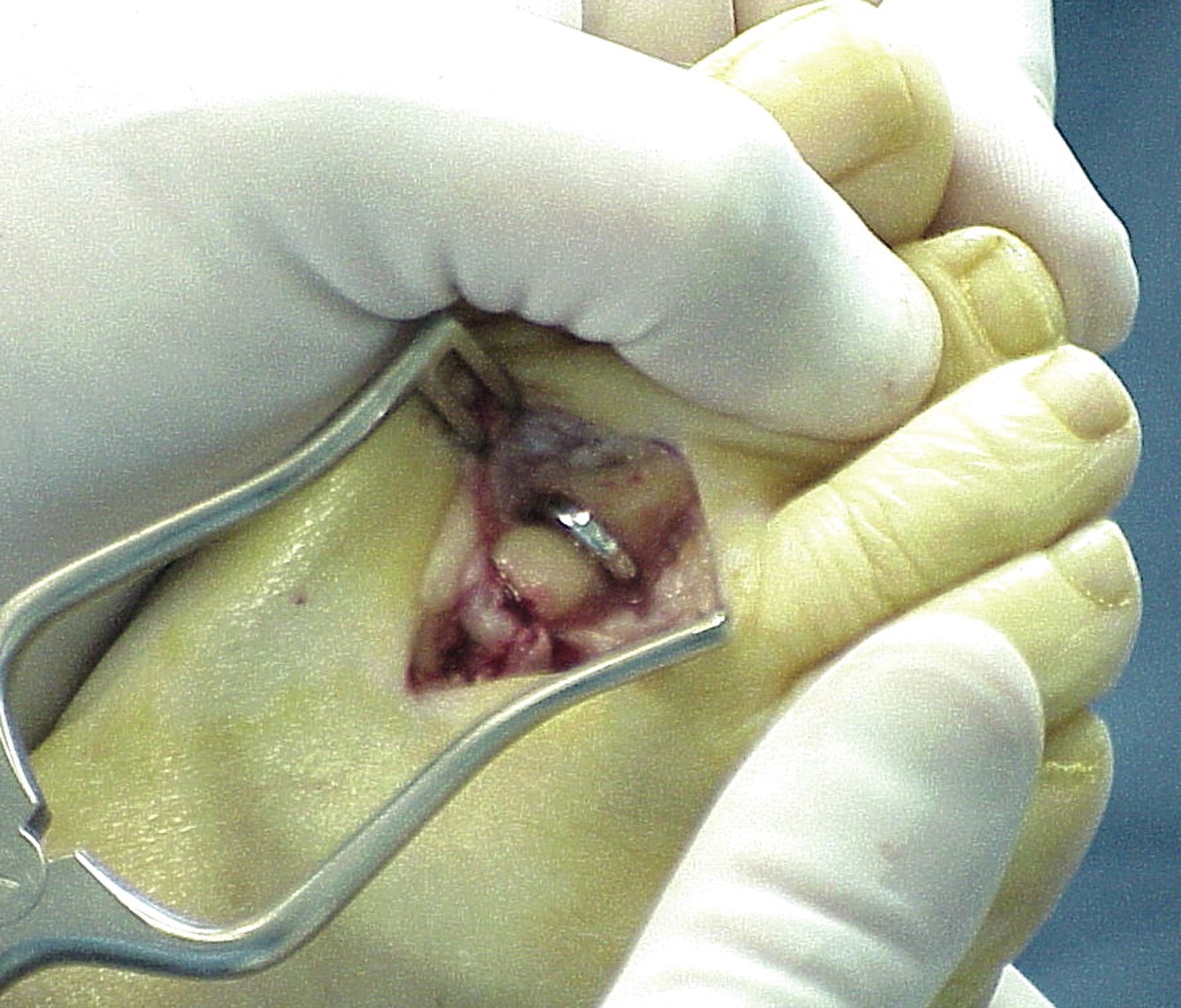
When it comes to the joint replacement procedure for lesser MPJs, one would start with a linear incision overlaying the affected lesser MPJ. Dissect down to the long extensor tendon. Retract the tendon either medially or laterally to expose the joint capsule. Perform a longitudinal capsulotomy to expose the MPJ. Dissect the capsular tissue away from the bone but take care to preserve as much of the soft tissue attachments as possible. Proceed to cut the base of the proximal phalanx and excise the phalanx from the surgical site. The advantage of using the cobalt-chromium alloy implant is that the size of the resected bone does not need to be any larger than the width of the implant. Utilize a sizing device to determine the proper implant size. Ream a canal in the shaft of the phalanx and test a trial sizer for fit. Place the toe through an extended range of motion. If the motion is acceptable, remove the sizer and place the properly sized implant into the proximal phalanx. Close the deep tissue and close the remaining tissue layers with the preferred sutures. Apply a sterile dressing and place the patient on partial weightbearing for the first two weeks. Have the patient proceed to full weightbearing by the third or fourth week. Patients can usually tolerate soft shoes by the fourth week. Be sure to begin range of motion exercises very shortly after surgery while the patient is still in the bandage.
Case Study: When There Is Trauma To The Second MPJ
A 24-year-old male dropped a 200-lb. iron plate on his right foot while at work. The initial diagnosis was fracture dislocation of the second MPJ. After six weeks of cast immobilization and six subsequent weeks of physical therapy, the patient presented to my office. The physical examination revealed normal neurovascular findings. However, the patient had extreme pain at the second MPJ and was unable to move the second toe due to stiffness and pain. Radiographs revealed a non-healed intraarticular fracture of the second MPJ. We repaired the fracture fragment with absorbable pins and inserted a hemi-implant. Six months later, the patient had full, non-painful range of motion of the second MPJ and returned to his original employment as a construction worker.
In Conclusion
Many patients with lesser MPJ disorders respond to conservative treatment options. When surgery is indicated for an end-stage MPJ that is painful, stiff, causes gait alterations and affects the patient’s lifestyle, a metallic hemi-implant is the implant of choice. It is relatively easy to use and produces reproducible results with a very high patient satisfaction. Dr. Muscarella is the Acting Chairman of the Department of Surgery at the Temple University School of Podiatric Medicine (TUSPM). He is an Associate Professor in the Departments of Surgery and Orthopedics at TUSPM. Dr. Muscarella is board-certified by the American Board of Podiatric Surgery. He is a Fellow of the American College of Foot and Ankle Surgeons. References 1. Warwick R, Williams P. Gray's Anatomy, 35th British edition, 1973. 2. Mizel M, Yodlowski M. Disorders of the Lesser Metatarsophalangeal Joints. Journal of the American Academy of Orthopaedic Surgeons 3(3):166-173, May/June 1995. 3. Fox I, Pro A. Lesser Metatarsophalangeal Joint Implants, The Journal of Foot Surgery 26(2):159-163, 1987. 4. Lawrence B, PapierII M. Implant Arthroplasty of the Lesser Metatarsophalangeal Joint-A Modified Technique, The Journal of Foot Surgery 19(1):16-18, 1980. 5. Sgarlato T, Sutter. Double-Stem Silicone Implant Arthroplasty of the Lesser Metatarsophalangeal Joints, The Journal of Foot Surgery 28(5):410-413, 1989. 6. Townley, et. al, A Metallic Hemiarthroplasty Resurfacing Prosthesis for the Hallux Metatarsophalangeal Joint. Foot & Ankle International 15(11), 1994. 7. Taranow and Townley. Metallic Proximal Hemiarthroplasty For Hallux Rigidus. Operative Techniques in Orthopedics 9(1), 1999.
References:
CE Exam #131 Choose the single best response to each question listed below. 1. Which of the preexisting conditions can cause lesser metatarsophalangeal joint (MPJ) disorders? a) Faulty biomechanics b) Infection c) Trauma d) All of the above 2. Which of the following statements about the plantar plate is false? a) It is comprised of the plantar aponeurosis and the plantar capsule. b) It enhances stability of lesser MPJs with help from the intrinsic muscles. c) It acts as a tremendous shock absorber for walking during the propulsive phases of gait. d) None of the above 3. Which of the following statements about articular cartilage is true? a) One commonly sees articular cartilage on the dorsal surface of the metatarsal. b) Articular cartilage covers the distal and plantar portions of the metatarsal heads. c) The articular cartilage of the phalangeal bases encompasses half of the cavity of the bone. d) None of the above 4. Lesser MPJs have relatively __ degrees of dorsiflexion in stance. a) 25 degrees b) 50 degrees c) 75 degrees d) 90 degrees 5. Pathology of the lesser MPJs may be … a) metabolic b) degenerative c) traumatic d) all of the above 6. Which is a possible post-op complication of arthrodesis on the lesser MPJ? a) Plantar lesions b) A lack of dorsiflexion of the joint c) Stress fractures of the affected metatarsal d) None of the above 7. Surgeons frequently see transfer lesions with … a) arthroplasty and resection of the base of the proximal phalanx b) metatarsal head resection c) joint replacement d) all of the above 8. In the author’s experience, which of the following procedures for lesser MPJs completely destroys the soft tissue balance around the joint? a) Arthrodesis b) Arthroplasty with resection of the base of the proximal phalanx c) Joint replacement d) Metatarsal head resection 9. To perform the joint replacement procedure for lesser MPJs correctly, one should … a) ensure minimal bone resection b) maintain soft tissue integrity around the joint c) a and b d) none of the above 10. When dissecting capsular tissue away from bone during the aforementioned joint replacement procedure, one should take care to preserve … a) the long extensor tendon b) soft tissue attachments c) the proximal phalanx d) none of the above Instructions for Submitting Exams Fill out the enclosed card that appears on the following page or fax the form to NACCME at (610) 560-0502. Within 60 days, you will be advised that you have passed or failed the exam. A score of 70 percent or above will comprise a passing grade. A certificate will be awarded to participants who successfully complete the exam. Responses will be accepted up to 12 months from the publication date.


{kind=link}
{kind=link}
{kind=link}