


How a Classification System Can Aid in Brachymetatarsia Surgery
 Patients with brachymetatarsia have at least one shortened metatarsal, resulting in a suboptimal appearance and abnormal function. The deformity has two components: osseous (metatarsal and the corresponding phalangeal bones) and soft tissue. Congenital brachymetatarsia consists of a deficiency in metatarsal growth along with the corresponding phalangeal bones. In contrast, traumatic brachymetatarsia exhibits normal phalangeal length.
Patients with brachymetatarsia have at least one shortened metatarsal, resulting in a suboptimal appearance and abnormal function. The deformity has two components: osseous (metatarsal and the corresponding phalangeal bones) and soft tissue. Congenital brachymetatarsia consists of a deficiency in metatarsal growth along with the corresponding phalangeal bones. In contrast, traumatic brachymetatarsia exhibits normal phalangeal length.
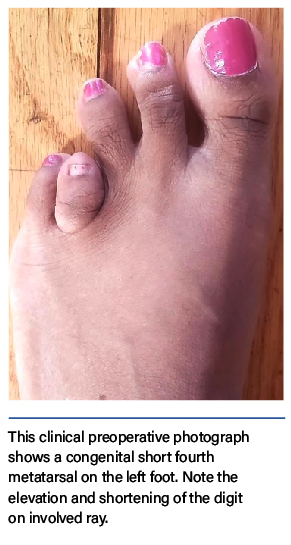
The ray with brachymetatarsia will clinically have a shortened toe that sits more dorsal than the adjacent toes, which then converge toward the space of a shortened toe. Greater amounts of metatarsal shortening cause deeper plantar skin creases. If the foot has more than one short metatarsal, the condition is known as brachymetapody.1
Anatomically, the lesser metatarsal physis is in the neck of the bone, and that of the first metatarsal is in the base. This means first metatarsal brachymetatarsia has a greater effect on the sagittal plane position, as evidenced by the increased declination in the sagittal plane moreso than the lesser metatarsals. Lesser metatarsal brachymetatarsia has normal sagittal plane declination but has a flexed metatarsal head/neck.1,2
 The frequency of brachymetatarsia ranges from 1 in less than 1000 to 1 in 2500 births.2,3 Brachymetatarsia is congenital, but with poorly understood genetics. The condition is not known to have a hereditary component, but the senior author has seen it on occasion.
The frequency of brachymetatarsia ranges from 1 in less than 1000 to 1 in 2500 births.2,3 Brachymetatarsia is congenital, but with poorly understood genetics. The condition is not known to have a hereditary component, but the senior author has seen it on occasion.
Our own recent study found a female to male brachymetatarsia ratio of 9:1, similar to a ratio of 10:1 in a recent review.4,5 In that same review, the authors found a 47% prevalence of bilateral brachymetatarsia, while we found a prevalence of 30% in our study.4,5 Of the 300 brachymetatarsals that we studied, the majority were of the fourth metatarsal (174 or 58%).5
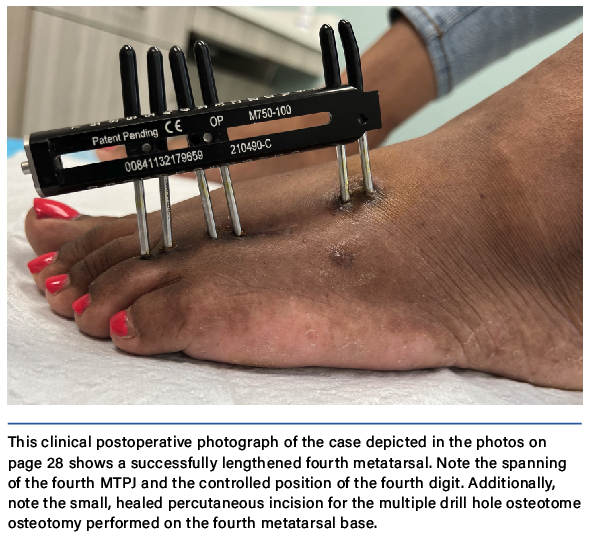
Surgeons have utilized various techniques for acute and gradual metatarsal lengthening, although there are documented complications.1–8 A commonly encountered complication of metatarsal lengthening is metatarsophalangeal joint (MTPJ) stiffness or dislocation/subluxation. To prevent this complication, utilize bridging of the external fixation across the MTPJ during gradual callus distraction.9 In limb lengthening surgery, surgeons have long utilized the concept of bridging the joint to minimize postoperative joint stiffness and contracture.9
Greater lengthening of the bone predisposes the joint to greater forces, which increases the risk of joint subluxation, chondrolysis, and postoperative joint stiffness. Performing the osteotomy farther from the joint lessens the forces that act on the joint, making a proximal metataphyseal-diaphyseal junction ostetotomy preferable. Negative side effects such as cartilage injury to the joint and stiffness in the MTPJ—regardless of how long an axial pin is maintained—can arise when one uses axial pinning to stabilize the digit to the metatarsal head. To prevent postop subluxation, stiffness, and chrondrolysis, the senior author developed a technique of spanning and protecting the MTPJ. The bridging fixator also provides acute digital deformity correction with simultaneous joint distraction, which maintains the long-term mobility of the MTPJ.9-11
It can be a challenge even for experienced surgeons to protect the surrounding soft tissues and to lengthen the bone at the proper rate, rhythm, and trajectory. The risk for complications rises with higher amounts of bone lengthening.12,13 In the absence of any consensus regarding methodology of metatarsal lengthening for brachymetatarsia, the senior author developed a comprehensive anatomic classification system, the Lamm Classification, which provides a surgical guide to treating each classification type.5
 A Practical Guide to the Lamm Classification for Brachymetatarsia
A Practical Guide to the Lamm Classification for Brachymetatarsia
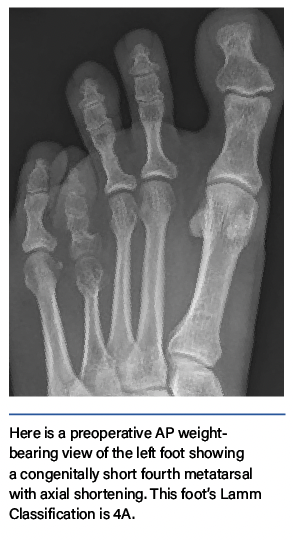
Brachymetatarsia deformities range from purely short metatarsals to irregularities of specific regions of the bone, including the shaft, head, and joint. The Lamm Classification is based on the normal foot radiographic measurements and angles.14
The classification includes three broad classification categories:
- Type A (axial distance deficiency) includes metatarsals that are normal in all respects except for their shortened length.
- Type B (bowing) involves angulation of the shaft of the affected metatarsal.
- Type C (congruency) exhibits joint imbalances and irregularities in the metatarsal head and phalangeal base.
 In addition to the A, B, and C types, the classification system uses one number ranging from 1–5 to indicate which metatarsal is short or hypoplastic.5 Therefore, if a patient has a short fourth metatarsal, bowing of the metatarsal shaft, and an incongruent MTPJ, this patient would be classified as a 4ABC.
In addition to the A, B, and C types, the classification system uses one number ranging from 1–5 to indicate which metatarsal is short or hypoplastic.5 Therefore, if a patient has a short fourth metatarsal, bowing of the metatarsal shaft, and an incongruent MTPJ, this patient would be classified as a 4ABC.
Acute lengthening with bone grafting has advantages for patients such as no need for external fixation. Disadvantages of acute lengthening include the need for bone grafting, for a donor site for autografting, for internal fixation, for acute compression of the joint cartilage, for a larger incision, and for a period of non-weight-bearing. In our study of 300 metatarsals, only 6% of metatarsals measured less than 10mm, and we do not recommend acute lengthening for metatarsal lengthening of 10 mm or more.5
 Our recent study reviewed 300 brachymetatarsals in 166 patients.5 Classification types included a total of 165 (55%) type A, a total of 6 (2%) type B, a total of 72 (24%) type AB, a total of 39 (13%) type AC, and a total of 18 (6%) type ABC. Fifty of the 166 (30%) patients had bilateral brachymetatarsia. Of the 300 metatarsals with brachymetatarsia, 64 (21%) were first metatarsals, 22 (7%) were second metatarsals, 28 (9%) were third metatarsals, 12 (4%) were fifth metatarsals, and 174 (58%) were fourth metatarsals. A total of 16 (10%) male and 150 (90%) female patients were evaluated. The mean preoperative amount of shortening of the metatarsal was 15 mm (range, 4–20 mm), as determined by the preoperative metatarsal parabola deficiency, equating to 30% of the preoperative metatarsal length.5
Our recent study reviewed 300 brachymetatarsals in 166 patients.5 Classification types included a total of 165 (55%) type A, a total of 6 (2%) type B, a total of 72 (24%) type AB, a total of 39 (13%) type AC, and a total of 18 (6%) type ABC. Fifty of the 166 (30%) patients had bilateral brachymetatarsia. Of the 300 metatarsals with brachymetatarsia, 64 (21%) were first metatarsals, 22 (7%) were second metatarsals, 28 (9%) were third metatarsals, 12 (4%) were fifth metatarsals, and 174 (58%) were fourth metatarsals. A total of 16 (10%) male and 150 (90%) female patients were evaluated. The mean preoperative amount of shortening of the metatarsal was 15 mm (range, 4–20 mm), as determined by the preoperative metatarsal parabola deficiency, equating to 30% of the preoperative metatarsal length.5
When Revisional Surgical Correction Is Required
We can also use the Lamm classification for revision surgical cases as the metatarsal length maybe short, correct, or long. These revision brachymetatarsia cases are complex and challenging since the deformity remains as type B (bowing of the metatarsal) and/or type C (incongruity of the MTPJ). Advanced imaging with computed tomography (CT) and magnetic resonance imaging (MRI) has developed our understanding of brachymetatarsia. The abnormal shape of the metatarsal head and base of the proximal phalanx and joint position are factors affecting the success of the lengthening especially as it relates to the final toe position. CT and MRI are extremely helpful in the initial planning for surgical treatment, especially for revisional surgical treatment of brachymetatarsia.
 A stiff and/or dislocated MTPJ is a common complication that requires revision surgery. When the MTPJ is not protected or the toe is pinned axially across the MTPJ during metatarsal lengthening, the toe becomes malpositioned and/or stiff, which results in a classification type C. The type of revisional surgery is patient specific but one must be careful to maintain the patient’s neurovascular status and restore the joint position, joint space and toe function. The preferable treatment is external fixation distraction of the MTPJ for 12 weeks together with osseous deformity correction using acute or gradual methods as well as open soft tissue balancing.
A stiff and/or dislocated MTPJ is a common complication that requires revision surgery. When the MTPJ is not protected or the toe is pinned axially across the MTPJ during metatarsal lengthening, the toe becomes malpositioned and/or stiff, which results in a classification type C. The type of revisional surgery is patient specific but one must be careful to maintain the patient’s neurovascular status and restore the joint position, joint space and toe function. The preferable treatment is external fixation distraction of the MTPJ for 12 weeks together with osseous deformity correction using acute or gradual methods as well as open soft tissue balancing.
What You Should Know About Bunions and Brachymetatarsia
Patients can experience hallux abductovalgus together with brachymetatarsia and in our recent study, hallux abductovalgus was present in 68 patients (41%).5 As the lesser brachymetatarsia toe(s) sits up on the dorsal foot and the adjacent toe(s) angulate(s) laterally toward the short toe space, which allows the big toe to laterally angulate. This creates/exacerbates the bunion.
 Surgeons typically correct hallux valgus deformity simultaneously with metatarsal lengthening using either internal or external fixation. The senior author finds it preferable to combine minimally invasive bunion correction with percutaneous metatarsal lengthening. In our experience, patients prefer this combination lengthening since the results of this procedure restore foot function and are aesthetically pleasing. Unlike the bunion deformity, the adjacent transverse angulation of the lesser toes typically self-corrects with the metatarsal lengthening. To correct the transverse plane deformity, one may need to perform an adjacent toe MTPJ capsulotomy. We do not recommend tenotomy or open tendon lengthening on initial metatarsal lengthening surgeries.
Surgeons typically correct hallux valgus deformity simultaneously with metatarsal lengthening using either internal or external fixation. The senior author finds it preferable to combine minimally invasive bunion correction with percutaneous metatarsal lengthening. In our experience, patients prefer this combination lengthening since the results of this procedure restore foot function and are aesthetically pleasing. Unlike the bunion deformity, the adjacent transverse angulation of the lesser toes typically self-corrects with the metatarsal lengthening. To correct the transverse plane deformity, one may need to perform an adjacent toe MTPJ capsulotomy. We do not recommend tenotomy or open tendon lengthening on initial metatarsal lengthening surgeries.
In Summary
Brachymetatarsia is a complex congential deformity, which until now has not been critically analyzed/classified. The senior author has treated many patients with brachymetatarsia successfully and also performed successful revision surgery utilizing the Lamm classification. The particular challenges of revision brachymetatarsia surgery spurred the development of a surgically based classification system to guide treatment.
The Lamm classifaction system permits a better understanding and a recommended surgical treatment guide for brachymetatarsia, and is the first system to provide a better understanding of the anatomical variations that occur with brachymetatarsia. Our study outlines a comprehensive classification system to guide the surgical treatment of brachymetatarsia.5 The classification shows metatarsal length discrepancy is not the only descriptive characteristic of brachymetatarsia and also is not the sole predictor of surgical technique. Still, the experience of the surgeon in bone lengthening, external fixation, and foot and ankle surgery remains paramount for the successful treatment of this complex congenital deformity.
The goals of metatarsal lengthening are to restore the metatarsal parabola for weight-bearing, to give the patient a better selection of shoe gear, to improve foot function, and to improve pedal cosmesis. Like limb lengthening, lengthening of metatarsals requires extensive knowledge of congential deformities, a sufficient understanding of external fixation, and a comperhensive surgical approach based on the new Lamm classification.
Dr. Bradley M. Lamm is the Chief of Foot and Ankle Surgery at St. Mary’s Medical Center and The Palm Beach Children’s Hospital as well as the Director of the Foot and Ankle Deformity Correction Center and Fellowship at the Paley Orthopedic and Spine Institute in West Palm Beach, Florida. He is the Rotation Director for the Podiatric Residency at Harvard Medical School. Dr. Lamm is a Fellow of the American College of Foot and Ankle Surgeons and serves as a section editor for the Journal of Foot and Ankle Surgery.
Tyler B. Lamm is a student at Oxbridge Academy in West Palm Beach Florida.
For further reading, see “Correcting Brachymetatarsia Of 45 Years” or “Striving For Optimal Cosmetic And Functional Results In Addressing Brachymetatarsia.”
References
1. Lamm BM. Metatarsal lengthening. In: Rozbruch RS, Ilizarov S, eds. Limb lengthening and reconstruction surgery. Informa Healthcare; 2007:291–302.
2. Davidson RS. Metatarsal lengthening. Foot Ankle Clin. 2001; 6(3):499–518.
3. Fox IM. Treatment of brachymetatarsia by the callus distraction method. J Foot Ankle Surg. 1998; 37(5):391–395.
4. Cordoba-Fernandez A, Vera-Gomez ML. Literature review on brachymetatarsia. Orthop Nurs. 2018; 37(5):292-302.
5. Lamm BM, Lamm TB. Brachymetatarsia: A classification for surgical treatment. J Foot Ankle Surg. 2022; epub June 11.
6. Lamm BM, Paley D, Herzenberg JE. Percutaneous distraction osteogenesis for treatment of brachymetatarsia. In: Scuderi GR, Tria AJ. Minimally Invasive Surgery in Orthopedics. Springer Science + Business Media; 2010:435-442,
7. Lamm BM, Gourdine-Shaw, MC. Problems, obstacles, and complications of metatarsal lengthening for the treatment of brachymetatarsia. Clin Pod Med Surg. 2010; 27(4):561-582.
8. Lamm BM. Moore KR. Knight JM. Pugh E. Baker JR. Gesheff MG. Intramedullary metatarsal fixation for treatment of delayed regenerate bone in lengthening of brachymetatarsia. J Foot Ankle Surg. 2018; 57(5):987-994.
9. Lamm BM. Percutaneous distraction osteogenesis for treatment of brachymetatarsia. J Foot Ankle Surg. 2009; 49(2):197–204.
10. Lamm BM. Brachymetatarsia: Distraction osteogenesis. In: Rozbruch RS, Hamdy RC, eds. Limb Lengthening and Reconstruction Surgery Case Atlas: Trauma, Foot and Ankle. Springer International Publishing Switzerland, 2016.
11. Lamm BM, Pugh ED, Knight JM. Pediatric brachymetatarsia. In: Butterworth ML, Marcoux JT, eds. The Pediatric Foot and Ankle. Springer Nature Switzerland AG; 2020:107-117,
12. Paley D. Principles of Deformity Correction. Springer, Heidelberg, 2002.
13. Kim HS, Lee YS, Jung JH, Shim JS. Complications of distraction in brachymetatarsia: Comparison between the first and fourth brachymetatarsia. J Foot Ankle Surg. 2019; 25(2):113–118.
14. Lamm BM, Stasko PA, Gesheff MG, Bhave A. Normal foot and ankle radiographic angles, measurements, and reference points. J Foot Ankle Surg. 2016; 55(5):991-998.

