


Scarring After Necrobiosis Lipoidica Ulceration: What Is the Impact?
© 2024 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Podiatry Today or HMP Global, their employees, and affiliates.
Necrobiosis lipoidica is a rare and difficult-to-treat condition that may present with associated ulcer formation. First described in 1929 in a person with diabetes1 and later recognized in nondiabetic persons2, the typical examination findings include waxy, yellow-brown skin changes, telangiectasic plaques with an elevated violaceous rim, and subcutaneous atrophy. Clinicians will commonly see these skin changes at the pretibial surface.3 The incidence of necrobiosis lipoidica in persons with diabetes is 0.3–1.2% with a female predominance. These often painful ulcerations can occur in up to 50% of persons with this condition, typically in cases with preceding trauma.4
The basis for diagnosis comes from clinical examination and histologic analysis. Histological findings of necrobiosis lipoidica include endothelial cell swelling and thickening of the blood vessel walls. Direct immunofluorescence shows IgM, IgA, fibrinogen and C3 in the blood vessels causing vascular thickening.5
While the etiology of necrobiosis lipoidica remains unclear, most cite an immune mediated causation, although collagen cross-linking increases because of elevated lysyl oxidase levels. Other observations include defective neutrophil migration, and TNFα elevated in the sera and skin.6–8
Common Roadblocks to Treatment
Clinicians may find treatment for ulcerations due to necrobiosis lipoidica frustrating. Cutaneous blood flow enhancers, corticosteroids, wound healing enhancers, immunomodulation, and surgery are among the available options.9 After these ulcerations heal, long-term consequences can include scarring, skin discoloration, and the potential for ulcer recurrence. The scarring is atrophic with continued loss of normal subcutaneous tissue, making recurrence from even minor trauma more likely.3
Scar tissue formation in wound healing is an expected occurrence.10 Macrophage phenotypes during wound healing have are an integral component of scarring. M1 macrophages are pro-inflammatory, whereas M2 types of macrophages are anti-inflammatory and pro-proliferative.11 There are many types of wound healing enhancers, now referred to as CAMPs (cellular, acellular matrix-like products). The level of retained cellular remnants (membrane components, long-strand DNA, etc) from the donor source directly relates to the macrophage phenotype predominant in the healing wound. A thoroughly decellularized CAMP is associated with M2 predominant macrophage phenotypes.12
The below case study seeks to evaluate long-term scarring through evaluation of subcutaneous tissue thickness after treatment of necrobiosis lipoidica ulceration at the same anatomic level with a cellular and acellular CAMP.
One Patient’s Experience With Scarring After Necrobiosis Lipoidica Ulceration

The patient in question is a 52-year-old Caucasian female with a 50-year history of type 1 diabetes. Her past medical history also includes peripheral arterial disease, coronary artery disease with myocardial infarction, stroke, hypertension, necrobiosis lipoidica ulcerations, hypothyroidism, gastroparesis, sleep apnea, arthritis, hyperlipidemia, hearing loss, retinopathy, renal insufficiency, and neuropathy. She has battled necrobiosis lipoidica ulcerations for more than 20 years and was part of a prior study published in 2013.13
She initially presented for this particular ulcerative occurrence to a hospital outpatient wound center for 3 months of therapy, including weekly debridement, corticosteroid therapy, topical collagen and antimicrobial products, culture-guided antibiotics, compression, and anti-platelet aggregation therapy. Unfortunately, clinicians noted no reduction in size or characteristics of the wound 3 months into this therapy (Figure 1) .

She then tried a novel decellularized porcine placental extracellular matrix (DECM, InnovaMatrix AC (ConvaTec). The treatment team in initiated weekly debridement and application of the DECM and noted epithelialization at the 8-week point of treatment. At 10 weeks the wound remained closed (Figure 2), and she began follow-up on a 2-month basis for long-term evaluation. Her follow-up appointments revealed very little scar tissue and apparent reformation of normal subcutaneous tissue. This was unexpected when compared to previously healed ulcerations at the same anatomic level that had undergone treatment with a cellular- and/or tissue-based product (CTP).
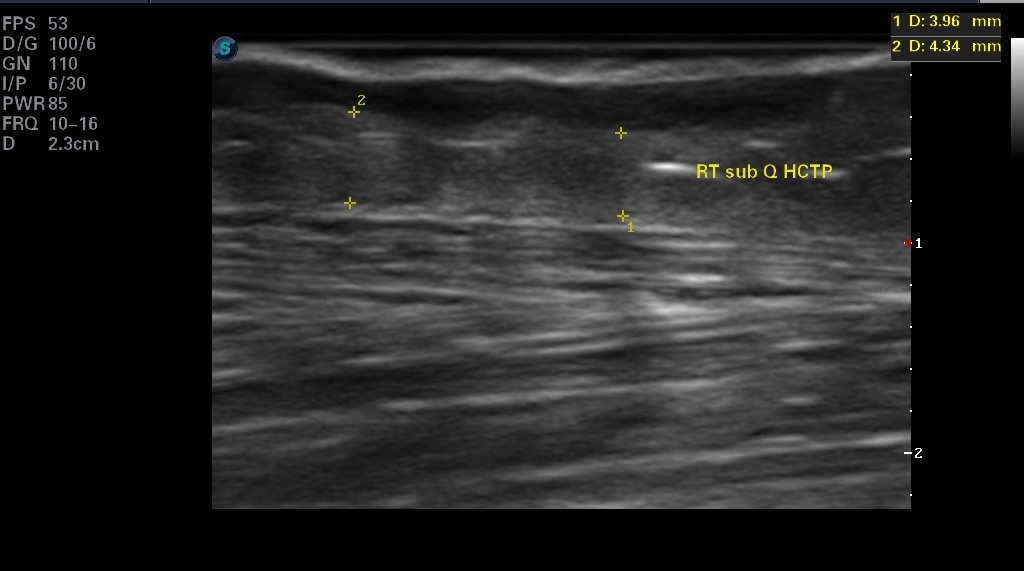
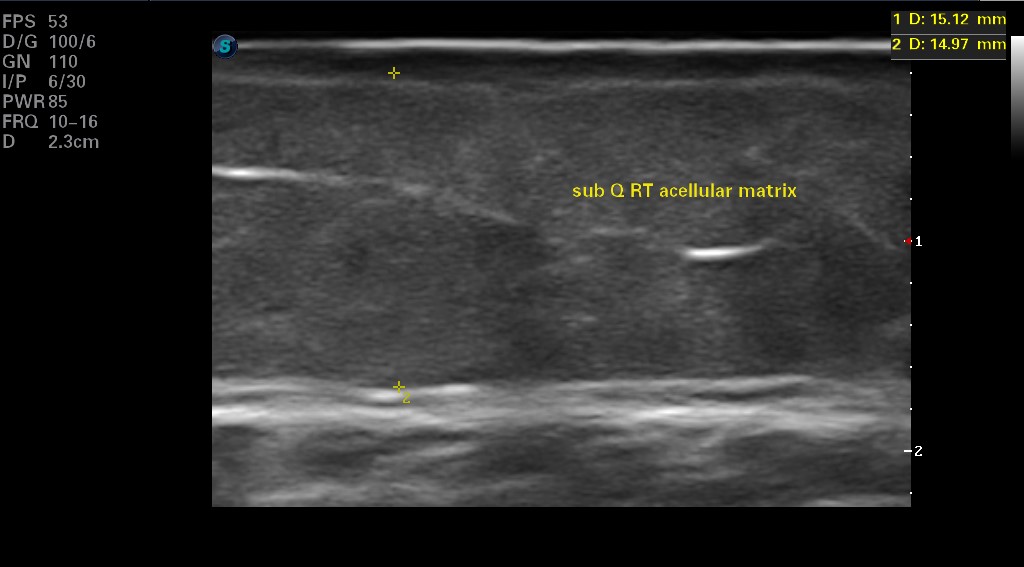
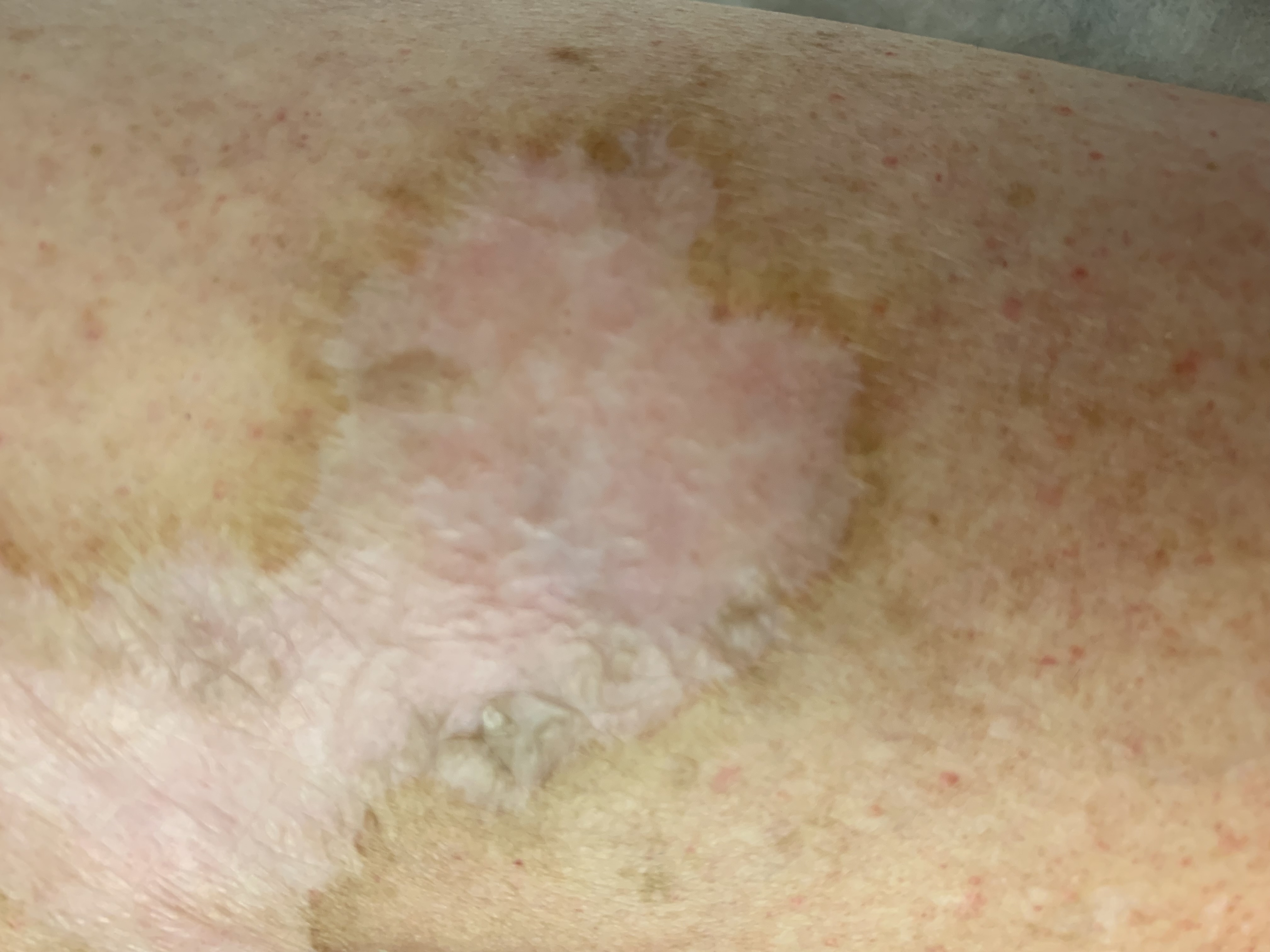
Sixteen months after initiating DECM therapy, the team performed ultrasound evaluation of the subcutaneous tissue for appearance and thickness of the fat, and the difference between the CTP and DECM healing was profound. On the right limb, the wound healed with a CTP occurred over the anterior compartment of the leg (just lateral to the tibial crest) and had remained healed for more than 5 years. The measurement of the subcutaneous tissue was 3.96–4.34mm thick (Figure 3). The physical appearance of that site was concave, atrophied, and with telangiectasia (Figure 4). The same limb healed with a DECM over the posterior compartment (just medial to the tibial crest) measured subcutaneous thickness of 14.97–15.12mm (Figure 5). The physical appearance was not concave, and the skin did not demonstrate telangiectasia, atrophy, or discoloration (Figure 6).

Analysis then compared the same anatomic sites on the left limb. The nonulcerated site at the same anatomic level of the anterior compartment on the left leg measured the subcutaneous tissue thickness at 12.44mm. A previously healed necrobiosis lipoidica ulcer was present at the posterior compartment just medial to the tibial crest on the left (contralateral) limb, also previously treated with a CTP more than 5 years prior. It has a concave, atrophied, telangiectasic appearance also. The subcutaneous thickness at this healed site is 3.24mm. The subcutaneous tissue thickness of 12.44mm at the unaffected contralateral limb compares favorably with the DECM treated ulcer (14.97–15.12mm). The CTP subcutaneous thickness at the CTP sites is 3–4 times thinner.
Discussing the Key Findings
The observation that CTP and nature-derived extracellular matrix (NECM) products used in healing difficult necrobiosis lipoidica ulcerations produced markedly different clinical and ultrasonographic appearances after remodeling phase healing evaluation begs for a proposed explanation.
Now, we recognize that macrophage phenotypes are regulators of scar tissue formation.11 Cellular remnants in CAMPs provoke an innate immune response and are proinflammatory with M1 macrophages predominating. Thoroughly decellularized extracellular matrices promote the predominance of M2 macrophages, which are anti-inflammatory and pro-proliferative.11
Because a thoroughly decellularized extracellular matrix promotes a M2 type macrophage phenotype,12 the difference in scar formation in this case seems to clinically validate findings in the existing literature. In this case study, the DECM-treated site produced little scar tissue, normal subcutaneous tissue, and a more normal skin appearance than the CTP-treated site. This concept warrants further investigation with more robust sample sizes to enhance the evidence.
Dr. Rader is the Medical Director of Memorial Hospital Wound Center and Indiana Foot & Ankle in Jasper, IN.
References
1. Oppenheim M. Eigentümlich disseminierte Degeneration des Bindegewebes der Haut bei einem Diabetiker. Z Hautkr. 1929-30;32:179.
2. Kozak GP, Kroll LP. Disorder of skin in diabetes. In: Joslin Diabetes Mellitus. (12th ed.) KM Varghese Company; 1985: 770–771.
3. Lepe K, Riley CA, Salazar FJ. Necrobiosis lipoidicaIn: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024. Available from: https://www.ncbi.nlm.nih.gov/books/NBK459318/ .
4. Erfurt-Berge C, Seitz AT, Rehse C, Wollina U, Schwede K, Renner R. Update on clinical and laboratory features in necrobiosis lipoidica: a retrospective multicentre study of 52 patients. Eur J Dermatol. 2012;22(6):770-775.
5. Ullman S, Dahl MV. Necrobiosis lipoidica. An immunofluorescence study. Arch Dermatol. 1977;113(12):1671-1673.
6. Hammer E, Lilienthal E, Hofer SE, Schulz S, Bollow E, Holl RW, DPV Initiative and the German BMBF Competence Network for Diabetes Mellitus. Risk factors for necrobiosis lipoidica in Type 1 diabetes mellitus. Diabet Med. 2017;34(1):86-92.
7. Franklin C, Stoffels-Weindorf M, Hillen U, Dissemond J. Ulcerated necrobiosis lipoidica as a rare cause for chronic leg ulcers: case report series of ten patients. Int Wound J. 2015;12(5):548-554.
8. Ehlers S. Tumor necrosis factor and its blockade in granulomatous infections: differential modes of action of infliximab and etanercept? Clin Infect Dis. 2005;41 Suppl 3:S199-203.
9. Nihal A, Caplan AS, Rosenbach M, Damsky W, Mangold AR, Shields BE. Treatment options for necrobiosis lipoidica: a systematic review. Int J Dermatol. 2023;62:1529-1537.
10. Marshall CD, Hu MS, Leavitt T, Barnes LA, Lorenz HP, Longaker MT. Cutaneous scarring: basic science, current treatments, and future directions. Adv Wound Care (New Rochelle). 2018;7(2):29-45.
11. Hesketh M, Sahin KB, West ZE, Murray RZ. Macrophage phenotypes regulate scar formation and chronic wound healing. Int J Mol Sci. 2017;18(7):1545.
12. Keane TJ, Londono R, Turner NJ, Badylak SF. Consequences of ineffective decellularization of biologic scaffolds on the host response. Biomaterials. 2012;33(6):1771-1781.
13. Rader AJ, Wilson M. Bioengineered human dermal tissue grafting of necrobiosis lipoidica diabeticorum ulcerations: a case series. Wounds. 2013 Nov;25(11):310-2. PMID: 25867630.





