What Is the Cause of These Waxy, Dermal Papules?
© 2023 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of The Dermatologist or HMP Global, their employees, and affiliates.
Case Report

A 45-year-old woman with Fitzpatrick II skin phototype presented with a 7-month history of a widespread, pruritic rash unchanged by levocetirizine 5 mg twice daily and hydroxyzine 25 mg every night at bedtime. The patient denied any alleviating or exacerbating factors or recent change in medications. She also reported several years of weakness, arthralgias, and joint stiffness. Physical examination revealed 2- to 3-mm, waxy, dermal papules on the face, trunk, and extremities (Figure 1). A biopsy was obtained.
What Is The Diagnosis?
Check your answer below!
Diagnosis
Generalized Eruptive Histiocytosis (GEH)
Our patient was presented at the Morphology Conference at the University of Oklahoma where the consensus diagnosis of GEH was given based on characteristic presentation, including age of onset, lesional distribution, and pathology showing dermal histiocytic infiltrate, as well as a lack of joint deformity or concerning findings on workup for systemic malignancy to support a diagnosis of multicentric reticulohistiocytosis (MRH).
GEH is a rare subtype of non-Langerhans cell histiocytosis (non-LCH) characterized by recurrent eruptions of red-brown papules in a widespread axial distribution. The pathologic cells driving GEH derive from the mononuclear-macrophage system, as is the case with all histiocytoses. More specifically, GEH is thought to belong to a subset of non-LCH disorders related specifically to abnormalities in dermal dendritic cells. This family of disorders also includes juvenile xanthogranuloma (JXG), benign cephalic histiocytosis (BCH), and xanthoma disseminatum (XD).1 Although the typical disease course is spontaneous resolution within several months, GEH may persist for years or, rarely, progress to more serious forms of non-LCH such as XD.2-5
Differential Diagnosis
JXG presents as solitary or multiple, dome-shaped, reddish to tan papules favoring the head and neck. Onset is typically at birth or within the first year of life, although presentation during adulthood may be seen in about 10% of cases.6
BCH presents as multiple, asymptomatic, reddish to tan papules favoring initial cephalic involvement with subsequent caudal progression to involve the trunk and extremities. Onset is typically between ages 2 and 34 months, with rare cases presenting as late as age 5 years.7
XD also appears as multiple, reddish to tan, grouped papules, primarily favoring flexor and intertriginous surfaces.8
MRH is another important diagnosis to consider in patients with multiple, round, reddish to tan papules or nodules and a biopsy showing dermal histiocytic infiltrate. Lesions in MRH classically erupt in a symmetric distribution favoring acral surfaces, particularly overlying joints. Typical age of onset is middle age, with a predilection for women. In addition to cutaneous eruption, MRH is usually associated with erosive polyarthritis, which often leads to joint deformity, and 25% of cases are associated with underlying malignancy.9
Treatment
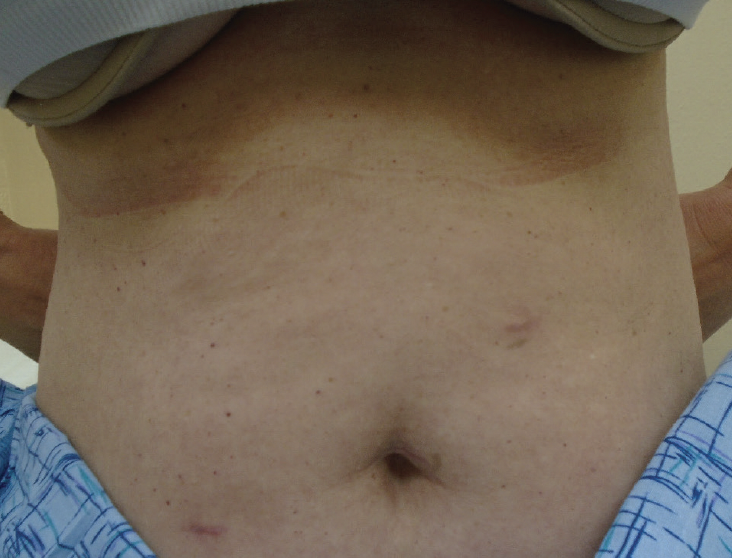
Currently, no standard treatment exists for cases of GEH that fail to resolve spontaneously, and treatment recommendations are largely based on case reports. Previous reports have described selective clearing of GEH lesions in sun-exposed areas, as well as successful treatment with psoralen plus ultraviolet A (PUVA).3,4 However, PUVA is costly and poorly tolerated by many patients.10 Our patient was treated with UVA in the absence of psoralen and achieved complete clearance of lesions within 3 months after failing to improve with multiple other treatment modalities (Figure 2).
Our Patient
After experiencing no improvement with narrowband UVB therapy, isotretinoin, intramuscular steroid injections, and 1064 nm Nd:YAG laser therapy, referral was placed for initiation of full-body PUVA therapy. However, due to cost, the patient opted to forgo the psoralen and attempted broadband UVA therapy alone. She received a total of 64 treatments over a 9-month period. Treatment was initiated 3 times weekly then gradually tapered to once weekly due to scheduling conflicts. Initial fluence was set to 0.5 mJ/cm2 and gradually up titrated to 21.0 mJ/cm2 by the fifty-ninth treatment, then reduced to 16.5 mJ/cm2. Within 3 months of initiating treatment, the patient’s skin eruption resolved with residual hyperpigmented macules, which themselves resolved by the eighth month. She maintained complete clearance without relapse at the most recent follow up, 33 months after finishing treatment.
A Novel Therapeutic Option For GEH
UV phototherapy acts primarily via immunomodulation, inducing cytokine profile shifting, inhibition of antigen presenting cells, and induction of apoptosis through cytochrome C or the Fas signaling pathway.5 UV radiation is part of the electromagnetic spectrum that ranges from 100 nm to 400 nm. UVC (100 nm–280 nm) is the shortest wavelength and not utilized clinically. UVB therapy is divided into broadband UVB (280 nm–320 nm) and narrowband UVB (311 nm–320 nm). UVA therapy is divided into broadband UVA (320 nm–400 nm), UVA-2 (320 nm–340 nm), and UVA-1 (340 nm–400 nm).10
Wavelength is directly related to penetrance and inversely related to energy transmission. Thus, the relatively shorter wavelength light with UVB phototherapy has primarily been utilized for treatment of epidermal processes, such as vitiligo and psoriasis, which do not require deeper penetration. Similarly, UVA-1 has the longest wavelength and is primarily utilized in the treatment of processes wherein the pathology lies in the deep dermal and subcutaneous tissues such as morphea. Broadband UVA therapy covers a comparatively large range of wavelengths and is utilized in the treatment of a wide variety of dermatologic disorders, including atopic dermatitis, psoriasis, and cutaneous mastocytosis.11
Because of the decreased energy transmission associated with UVA phototherapy, UVA spectrum therapies are often paired with a photosensitizer such as psoralen to increase efficacy. The most common oral photo sensitizer is 8-methoxypsoralen, which works by covalently binding to nucleic acids in DNA, rendering them less stable and more easily damaged via irradiation, thus enhancing the apoptotic effect of UV phototherapy.12
Association between exposure to UVA radiation and improvement in GEH is supported by previous reports describing improvement following exposure to natural sunlight, as well as following treatment with PUVA.3,4 To our knowledge, this is the first report of successful treatment of GEH with UVA phototherapy in the absence of psoralen. The strong temporal correlation between UVA exposure and lesional resolution seen in our report in combination with the previous reports showing improvement with natural sunlight may suggest that the dermal histiocytic infiltrate of GEH may respond to lower doses of UVA radiation than those seen with psoralen photosensitization. However, for any isolated report of GEH, it cannot be excluded that time, itself, played a role in lesional resolution, as the condition eventually resolves spontaneously in most cases.
Conclusion
This case of GEH successfully treated with UVA therapy without the use of psoralen may represent a safe, cost-effective, and well-tolerated initial treatment option for patients with GEH requiring therapeutic intervention.
References
1. Weitzman S, Jaffe R. Uncommon histiocytic disorders: the non-Langerhans cell histiocytoses. Pediatr Blood Cancer. 2005;45(3):256-264. doi:10.1002/pbc.20246. PMID: 15547923
2. Kobayashi K, Kurihara Y, Yamagami J, et al. Generalized eruptive histiocytoma developing into xanthoma disseminatum with central diabetes insipidus. J Dermatol. 2019;46(8):e281-e283. doi:10.1111/1346-8138.14845
3. Misery L, Kanitakis J, Hermier C, Cambazard F. Generalized eruptive histiocytoma in an infant with healing in summer: long-term follow-up. Br J Dermatol. 2001;144(2):435-437.
4. Lan Ma H, Metze D, Luger TA, Steinhoff M. Successful treatment of generalized eruptive histiocytoma with PUVA. J Dtsch Dermatol Ges. 2007;5(2):131-134. doi:10.1111/j.1610-0387.2007.06178.x
5. Tang X, Shen H, Xu A, et al. Spontaneous regression of generalized eruptive histiocytosis: possible involvement of apoptosis? Int J Dermatol. 2007;46(10):1073- 1075. doi:10.1111/j.1365-4632.2006.03045.x
6. Hernández-San Martín MJ, Vargas-Mora P, Aranibar L. Juvenile xanthogranuloma: an entity with a wide clinical spectrum. Actas Dermosifiliogr (Engl Ed). 2020;111(9):725-733. doi:10.1016/j.ad.2020.07.004
7. Lange M, Iżycka-Świeszewska E, Michajłowski I, Barańska-Rybak W. Benign cephalic histiocytosis. Cutis. 2015;95(6):E15-E17.
8. Rupec RA, Schaller M. Xanthoma disseminatum. Int J Dermatol. 2002;41(12): 911-913. doi:10.1046/j.1365-4362.2002.01680_1.x
9. Tajirian AL, Malik MK, Robinson-Bostom L, Lally EV. Multicentric reticulohistiocytosis. Clin Dermatol. 2006;24(6):486-492. doi:10.1016/j.clindermatol.2006.07.010
10. Rathod DG, Muneer H, Masood S. Phototherapy. In: StatPearls [Internet]. StatPearls Publishing; 2022.
11. Lotti TM, Gianfaldoni S. Ultraviolet A-1 in dermatological diseases. Adv Exp Med Biol. 2017;996:105-110. doi:10.1007/978-3-319-56017-5_9
12. Guitart J. Psoralen plus UV-A therapy in the 21st century: use it or lose it. JAMA Dermatol. 2019;155(5):529-531. doi:10.1001/jamadermatol.2018.5844