Confronting Issues and Challenges Beneath the Surface: Emerging Eczema Therapies
Emerging Eczema Therapies, featuring April Armstrong, MD, MPH
Topical Therapies
The landscape for topical therapies for patients with atopic dermatitis (AD) looks very exciting. We are currently looking at three different mechanisms of actions: a topical phosphodiesterase (PDE)-4 inhibitor, a Janus kinase (JAK) inhibitor, and an aryl hydrocarbon receptor (AHR) modulator (Table). These options are quite promising for our patients with AD, as they all are additional nonsteroidal treatments. While we have good nonsteroidal options, such as our topical calcineurin inhibitors or crisaborole, the advent of these emerging therapies will add to our toolbox of what we can offer to our patients.
First, when we look at the topical PDE-4, we are talking about topical roflumilast. A phase 2 study showed that the 0.15% cream formulation had an approximately 72% improvement in Eczema Area and Severity Index, with greater than 50% of
patients achieving clear or almost clear at 4 weeks.
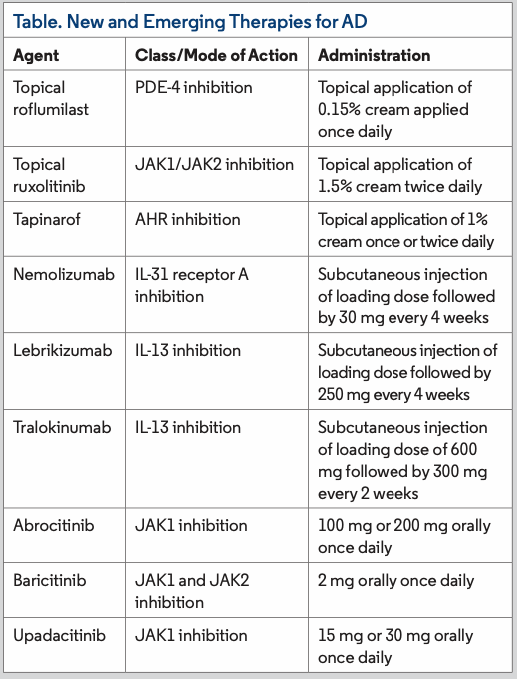
Another class of topical therapies is the topical JAK inhibitors, including topical ruxolitinib. Topical ruxolitinib is a JAK1 and JAK2 inhibitor that was recently approved by the FDA. The phase 3 studies looked at two formulations, 0.75% cream and 1.5% cream. With the 0.75% formulation, 45% of patients achieved clear or almost clear, and with the 1.5% formulation, 53% of patients achieved clear or almost clear. These percentages are important, because we saw very good efficacy with topical ruxolitinib in patients aged 12 years and older with mild to moderate AD. Overall, topical ruxolitinib was very well tolerated, with rates of application site reaction being lower than that of the placebo group.
The last class of innovative topical therapy for AD is the topical AHR agonists, which includes tapinarof. It has a role in limiting the dysregulated T helper (TH) 2 pathway that we see in patients with AD. Specifically, it can inhibit the IL-4 and signal transducers and activators of transcription 6 pathway. In addition, AHR inhibition can increase the level of filaggrin, which as we know is typically impaired in patients with AD.
In the dose ranging study, 55% of patients who applied tapinarof 1% twice daily achieved clear or almost clear by week 12. When they looked at another dose of once-daily application, 45% achieved clear or almost clear. Comparatively, approximately 25% of patients in the vehicle group had that level of response by week 12. Overall, tapinarof was well tolerated. About 5% to 7% of patients experienced folliculitis; however, this was generally mild and resolved with or without treatment.
Biologics
When we think about the different mechanisms that are implicated in AD, we typically think about the TH2 pathway. The TH2 targets under investigation in drug development have mostly been in IL-13, IL-4, and IL-31. Among those, IL-13 is thought to be important in mediating the inflammatory response seen clinically on the skin as well as the debilitating itch associated with AD. Similarly, IL-31 is important in itch mediation, not only just in AD but also in a number of different disease states. One last pathway that we are trying to understand is IL-33. When at excess levels, IL-33 is thought to be responsible for disruptions in the skin barrier as well as mediating itch. Thus, with all these pathways, we are at a very exciting time for AD treatment development. There are several different biologic therapies in the pipeline, including nemolizumab, lebrikizumab, and tralokinumab, which is in the latest phase development and currently under FDA review (Table).
Tralokinumab, an IL-13 antagonist, is dosed every 2 weeks, but phase 3 trials have shown some possibility of a 4-week dosing regimen. In its pivotal trials, approximately 22% of patients achieved clear or almost clear at week 16. These results show that tralokinumab could be another first-line biologic option. In addition, for patients who do not tolerate dupilumab, the biologic that revolutionized AD treatment, tralokinumab could be an effective treatment. The trials have found that tralokinumab does have a slightly slower onset of action. Its mechanism of action may be partially responsible for the long lasting effects seen thus far, with an increase in response rate even after week 24 in a subset of patients. Additionally, when tralokinumab was used in combination with topical steroids—a combination that mimics real-world use—approximately 39% of patients achieved clear or almost clear response by week 16.
Based on this evidence, there is no reason that tralokinumab cannot be used as a first-line systemic agent for patients who have not responded on dupilumab or who have experienced side effects.
Oral JAK Inhibitors
Oral JAK inhibitors are an expanding area of AD treatment. This class seems to improve itch rapidly, with a response sometimes within days of initiating therapy. It also important to note that not all JAK inhibitors are the same; the efficacy, tolerability, and safety profile depend on both the molecule and its dose (Table). Across the class, there are some safety and tolerability outcomes that we may want to think about, including herpes zoster and herpes simplex virus (HSV), but most can be treated and the JAK inhibitor can be continued.
Of the three options in current FDA review, baricitinib is the lowest-dosed JAK inhibitor. The overall efficacy seems to be more modest as well, but there is good efficacy for
patients with more moderate disease with less than 50% body surface area affected. Baricitinib is likely the best tolerated JAK inhibitor among the three that we’re talking about today. There’s low rates of nausea, vomiting, or acne with baricitinib. Again, as with all three JAK inhibitors, we see increased rates of HSV—less than 4%—and herpes zoster was also seen but at low frequency—less than 1%. Additionally, serious infections were not increased with baricitinib, and malignancy rates were lower than placebo. No venous thrombosis (VTE) at the 2-mg dose were observed.
Abrocitinib, at two different doses, is the second JAK inhibitor being evaluated for the treatment of AD. The lower dose, 100 mg, has shown similar efficacy to dupilumab, and the
200 mg dose may even have higher efficacy than dupilumab. As for tolerability and safety, nausea was noted in up to almost 15% of patients, but this adverse effect tended to be transient. Herpes zoster and HSV were observed but in most cases resolved with treatment. Notably, there was some rare (≤5%) transient platelet reduction at week 4 in some of the trials, and VTE was quite rare at 0.3 per 100 patient-years, which is similar to the background AD VTE rates regardless of therapy.
The last JAK inhibitor to mention is upadacitinib, which shows the highest efficacy of JAK inhibitor class at its 30-mg dose. In studies, this dose showed superiority to dupilumab. What about the safety profile? Overall, upadacitinib was well tolerated. Acne is something that we have seen that seems to be a bit unique and can occur in up to 17% of patients receiving the 30-mg dose. Again, herpes zoster was seen as with the other JAK inhibitors. Serious infections occurred in less than 1% of the treated population.
With upadacitinib, neutropenia and lymphopenia were observed in up to 5% of patients. Therefore, whether looking to start upadacitinib or another JAK inhibitor, it is important to perform a baseline laboratory workup and ongoing monitoring. These tests include complete blood count, comprehensive metabolic panel, lipid profile, tuberculosis, and viral hepatitis. The recommended follow-up interval is 12 weeks minimum.