Use of Intravascular Lithotripsy in a Staged Repair of Severe Bilateral Common Femoral Artery Disease

Vascular Surgeon
UT Southwestern Medical Center
Dallas, Texas
Vascular Disease Management speaks with Michael Siah, MD, from UT Southwestern Medical Center in Dallas, Texas, about treating CFA disease with the Shockwave M5+ catheter. Dr. Siah’s case report follows the interview.
How do you decide to use an endovascular vs a surgical approach for common femoral artery (CFA) treatment?
It ultimately depends on the indication. Most of my interventions are performed for patients with either rest pain or tissue loss. Once that indication is satiated, usually these patients will have either cross-sectional imaging or on-table angiography, depending on the anatomic location of where their disease exists.
In the relatively uncommon situation where the disease is purely isolated to the CFA, or maybe the distal external iliac artery and the CFA, those patients are good candidates for endovascular interventions. But I feel if their disease extends into the profunda femoris, or there is extensive disease at the origins of the superficial femoral artery, or the superficial femoral artery and the profunda femoris, I worry about plaque shifting; those patients are better served by an open intervention.
Other considerations I have are patient characteristics. For certain patients, some physicians talk about doing common femoral endarterectomies under local or regional anesthesia; however, I’ve never done this. That’s more of an academic conversation. Because most of these patients need general anesthesia to undergo these procedures, obviously, patient comorbidities can play hand in hand with that.
I don’t think that patients with bad ejection fractions, or those on home oxygen in addition to their underlying peripheral vascular disease, are best served by open surgical interventions. If patients are morbidly obese, or if I’m worried about wound complications or this is a redo intervention for a previously endarterectomized CFA, endovascular treatment jumps straight to the forefront of my thought process.
As a vascular surgeon, what percentage of your peripheral procedures are surgical vs endovascular? Do you think this is shifting, and why?
The last 2½ years have had a huge impact on my practice, skewing it to 80% endovascular and 20% open. A big reason for that is the availability and access to ICU beds postoperatively.
When it comes to the management of CFA disease, it’s probably 50% surgical and 50% endovascular. It’s tough to sell somebody on an operation that’s going to have them in the hospital for 3 days. Then when you talk about complications such as heart attack, growing complications, hematomas, and lymphoceles, those open interventions are a little bit less attractive. When you offer patients an endovascular solution, even though it may not have the same durability as an open intervention, they pick what is easiest for them. They don’t need to have an incision, they get to go home the same day, and they don’t need to spend time in the hospital. It becomes an increasingly attractive option for them.
What are the biggest challenges you face when performing endovascular procedures? And how has intravascular lithotripsy (IVL) impacted these challenges?
When it comes to chronic atherosclerotic lesions associated with peripheral arterial disease, calcium is a huge problem whether you’re doing open surgery or endovascular surgery. IVL has provided us with a new technology to treat calcium beneath the surface of these lesions, thereby allowing us to treat more challenging lesions with lower balloon pressures without the need to stent.
IVL has opened new doors regarding areas that we have historically treated with balloons, atherectomy, and stents. It’s also provided us a new way to treat heavily calcified lesions in areas that historically haven’t been best served by endovascular solutions. Physicians are addressing the CFA and talking about intervening without putting in stents because of IVL. Furthermore, we don’t necessarily have to put in iliac stents. IVL has added a tool to our toolbox for treating challenging lesions that historically weren’t best served with the devices we had available.
What has been your experience with the Shockwave M5+ and IVL? Does M5+ enable you to perform procedures that you could not with the previous Shockwave M5 catheter?
It’s been wonderful—the M5+ is like Shockwave fast-forward. When I was in training, we were one of the trial sites for the Shockwave balloon, and I remember being flabbergasted at how long it felt that these balloon inflations and energy delivery cycles would take. The Shockwave M5+ catheter has increased our ability to treat more types of blood vessels faster, and that is really exciting.
Recently, I had a case with one of our vascular residents and on one side we had an M5 and on the contralateral side we had an M5+. I used the M5 first and the results were wonderful. However, the resident was blown away by how quick it felt like these interventions were with the M5+. In addition to the speed with which patients can be treated, the new sizes have been wonderful because you can appropriately treat blood vessels that, with the M5 alone, we weren’t able to treat. Historically, physicians were using 6-mm balloons in the CFA, but not many CFAs are 6 mm in diameter; they’re often much larger. The M5+ 8.0mm size allows us to take care of patients less invasively and more effectively.
Case Report
Use of Intravascular Lithotripsy in a Staged Repair of Severe Bilateral Common Femoral Artery Disease
Khalil Chamseddin, MD; Michael Siah, MD
NUT Southwestern Medical Center, Dallas, Texas
Introduction
The standard treatment for common femoral artery (CFA) occlusive disease has been open endarterectomy with patch angioplasty. While this approach yields long-term patency of more than 90% at 5 years, it carries risk of hematoma, lymph leak, and wound infection >10%.1-4 Endovascular treatment of CFA disease provides an alternative solution with lower procedure-related morbidity and mortality. Angioplasty, atherectomy, and stenting have been shown to be safe and effective for CFA disease; however, due to inferior long-term patency, they remain controversial.5,6 Intravascular lithotripsy (IVL) has been used in calcified femoropopliteal and tibial segments with an acceptable safety profile. We present the case of a 54-year-old man with significant CFA disease treated with IVL.
Case Report
A 54-year-old man with a history of hypertension, hyperlipidemia, and chronic smoking presented to clinic with bilateral lower extremity rest pain. Due to diminished femoral pulses bilaterally, a CT angiography was performed, which showed severe bilateral CFA disease. The patient then underwent a staged repair. First, he underwent a right common femoral endarterectomy with patch angioplasty and right external iliac artery stenting with an 8-mm x 7.5-cm Viabahn stent (Gore). Given the persistence of symptoms in his left leg, and after a lengthy discussion about his options, it was decided to treat his left CFA disease with IVL.
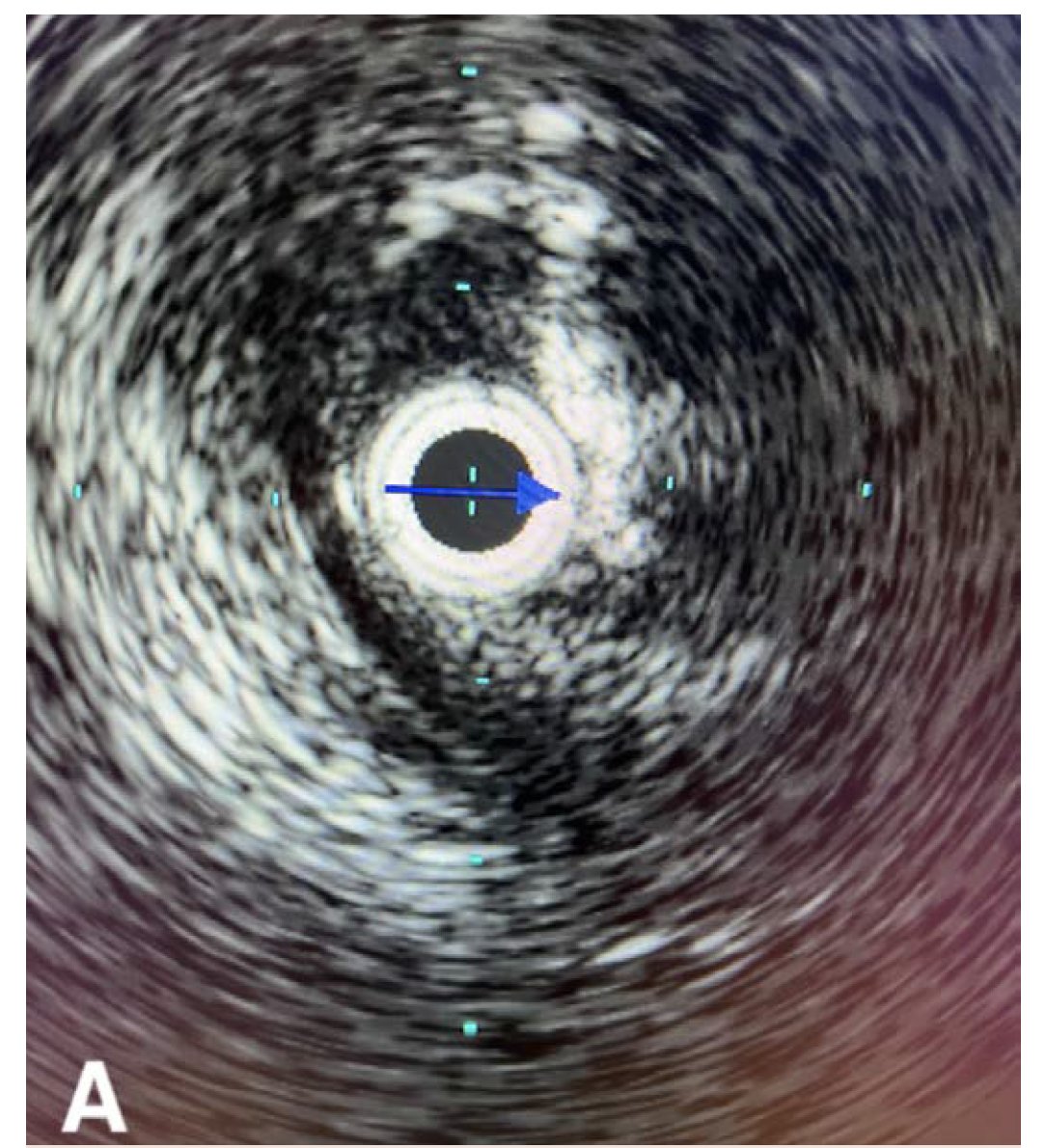
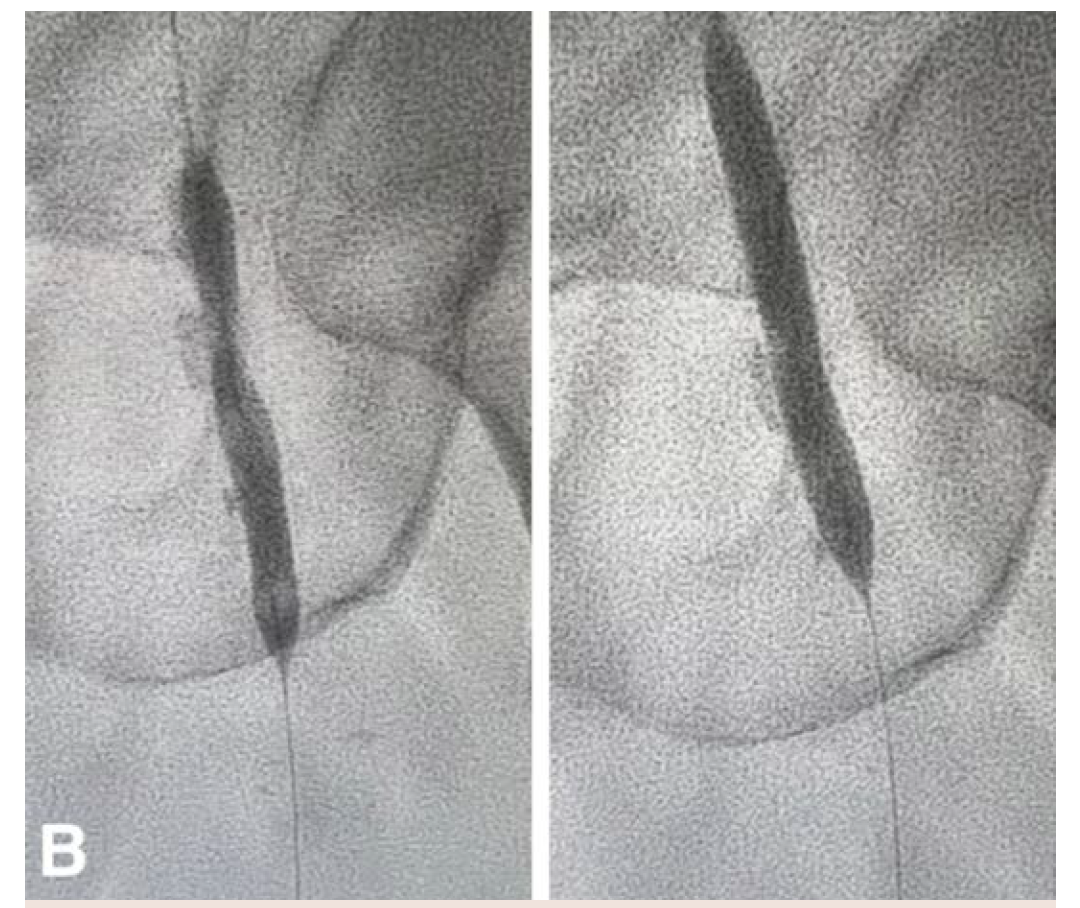
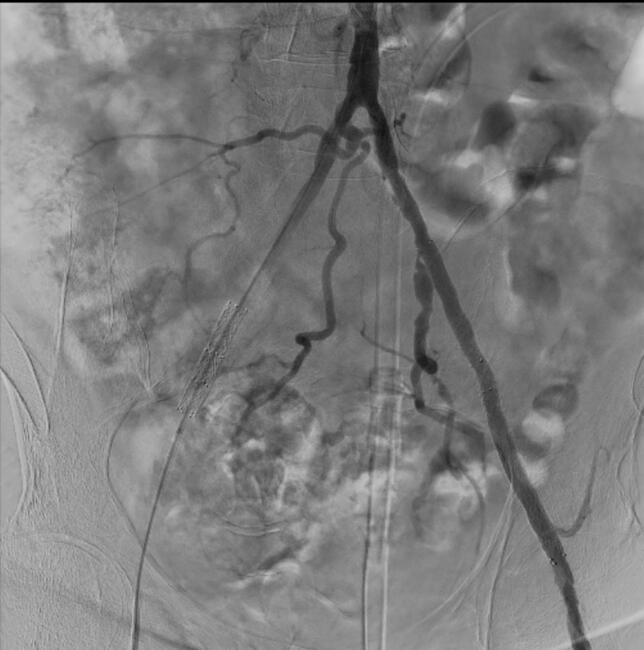
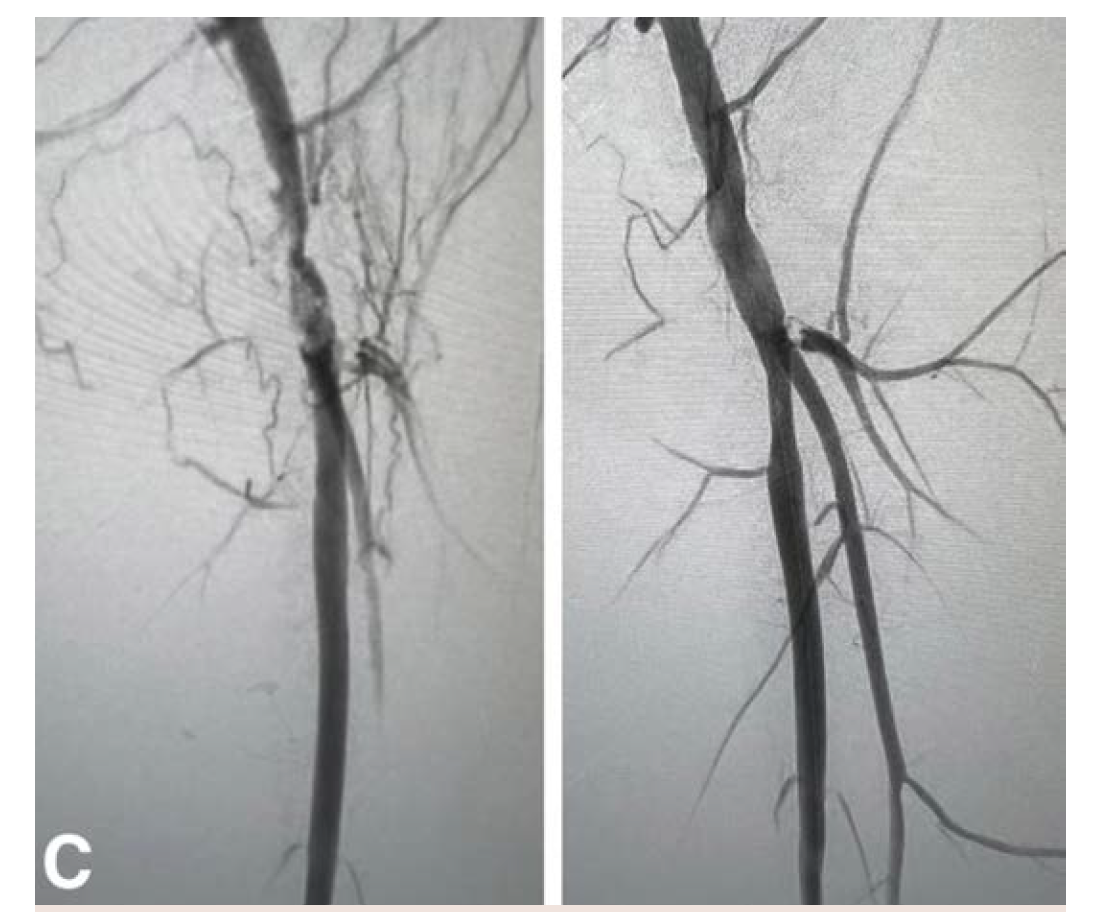
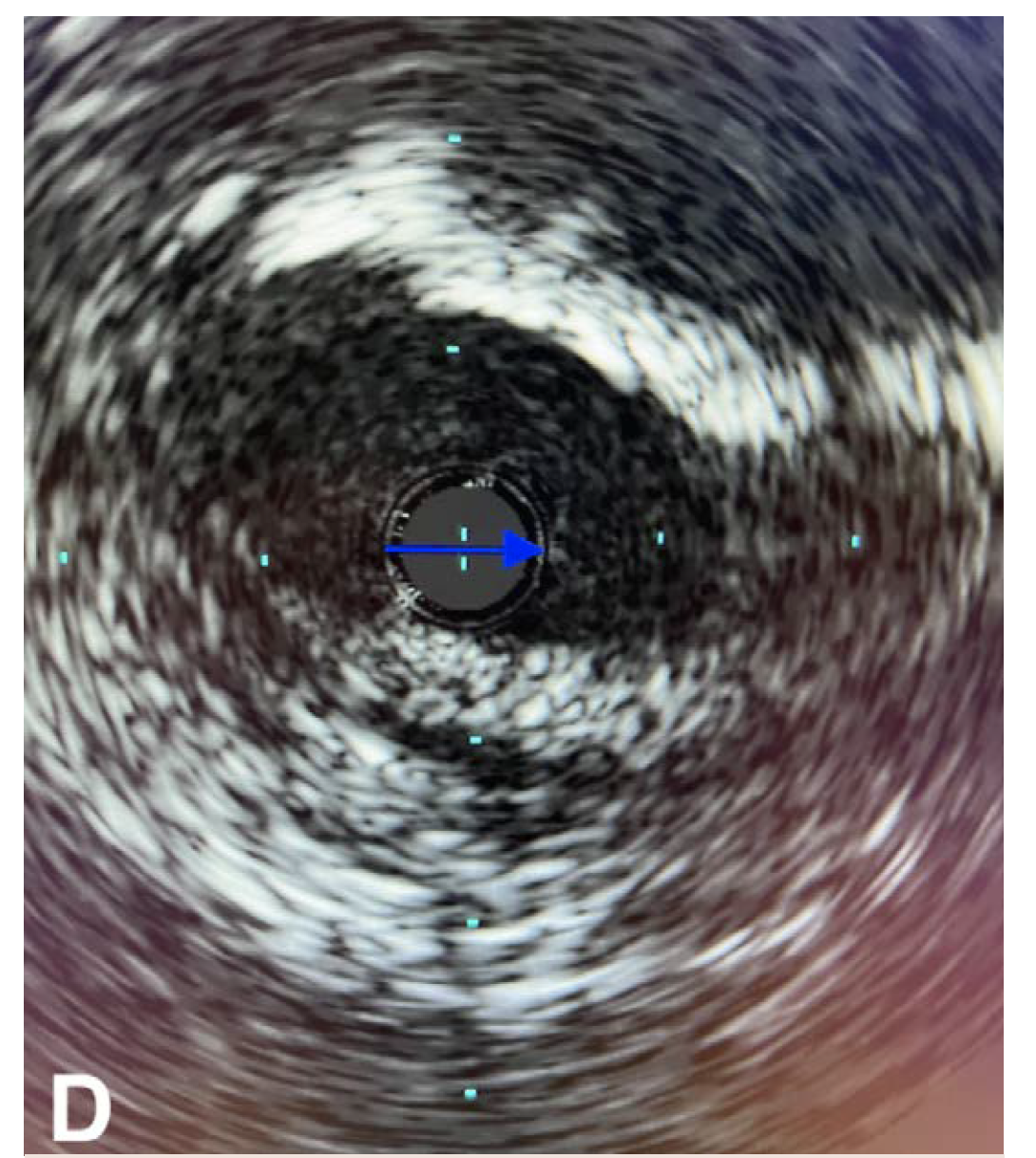
The patient underwent an initial catheter-directed diagnostic angiogram that revealed a 99% stenosis of the left CFA. The lesion was successfully transversed, and a 7 Fr 45-cm sheath was placed in the left external iliac artery. Intravascular ultrasound (IVUS) was performed over a 0.014" wire (Figure 1A), which demonstrated near occlusion of the CFA with heavy calcium burden. An 8-mm x 60-mm Shockwave balloon was then inflated to 4 atm, and 10 cycles were used to treat the CFA and proximal superficial femoral artery (Figure 1B). Completion angiogram showed an excellent result, with complete resolution of the calcific disease and no residual stenosis (Figure 1C). IVUS was performed at the end, which showed more than 80% luminal expansion after IVL treatment (Figure 1D). The patient was awakened from monitored anesthesia care and discharged from the postanesthesia care unit to home the same day.
Discussion
Endovascular treatment of peripheral arterial disease (PAD) at the iliac, femoropopliteal, and tibial levels represents first-line therapy in patients ranging from claudication to critical limb ischemia due to its low perioperative morbidity and mortality and shorter length of stay compared with open surgical revascularization. This treatment modality is particularly attractive in this patient population due to the prevalence of significant comorbidities. CFA occlusive disease remains a difficult entity to treat through percutaneous interventions. Criticisms of endovascular therapy highlight that angioplasty exerts high pressure that can risk dissection, which may require stenting in the CFA. Additionally, mobility and flexion of the CFA at the inguinal ligament may predispose it to stent fracture or occlusion. Risk of profunda femoris dissection, plaque shift, or embolization may compromise essential collateral flow to the lower extremity. Furthermore, CFA disease particularly has a high calcium burden. Intra-arterial calcium is associated with increased risk for dissection, distal embolization, perforation, and vessel recoil, predisposing the CFA to complications.
However, several studies have shown favorable safety profiles for endovascular treatment of the CFA.7,8 Mehta et al analyzed 167 patients undergoing percutaneous transluminal angioplasty (PTA) only, atherectomy with PTA, and provisional stenting. In a mean follow-up of 42 months, 20.4% of patients developed CFA restenosis; 10.8% required repeat percutaneous intervention; and 10.2% required open surgical revascularization. Provisional CFA stenting had 100% patency during the study follow-up. They found a complication rate of 1.8%, including 1 pseudoaneurysm, 1 thrombosis, and 1 distal embolization.5 Atherectomy has also been employed for treatment of CFA to improve restenosis rates and is often used in addition to drug-coated balloon angioplasty; however, it can be associated with 2% to 10% embolic complications.9,10
IVL has been introduced as an alternative and adjunct to treatment of highly calcified occlusive disease. It produces pulsatile sonic pressure waves that travel throughout the arterial layers to fracture calcium deposits within the intima and media. This results in increased vessel compliance, reduced vessel recoil, and expansion of intraluminal diameter.11 The DISRUPT PAD II trial was a nonrandomized multicenter study that treated 60 patients with IVL. Researchers found a residual stenosis of 24.2%, with an average 3-mm luminal gain after treatment. Only 1 dissection was observed, which required stent placement. Additionally, they noted a 12-month primary patency of 62.9% with optimal IVL technique.12 The DISRUPT PAD III trial was a randomized trial between IVL and plain balloon angioplasty in 306 patients that demonstrated plain balloon angioplasty was associated with more flow-limiting dissections (6.8% vs 1.4%; P=.02) and high rate of stent placement (18.3% vs 4.6%; P<.001), while IVL achieved more lesions with residual stenosis ≤30% (66.4% vs. 51.9%; P=.02).13 The 1-year patency rates for the PAD III RCT are expected later this year.
Similar results can be seen in the PAD III Observational Study, CFA cohort. The PAD III OS is a prospective, multicenter, single-blind observational study with the data currently released for 752 patients. The CFA cohort included 97 lesions and demonstrated effective treatment complex, calcified CFA lesions with pre-diameter stenosis percentages dropping over 40% after IVL treatment (77% v. 34%). The study also showed 0% perforation and distal embolization, as well as low Grade D-F dissection rates (1.3%).14
Conclusion
Our patient had significant calcific disease in the CFA, which was successfully treated with IVL without any evidence of dissection, perforation, or distal embolization. There was no access site complication, and the profunda femoris was preserved free of complication.
This interview was supported by Shockwave Medical.
Dr. Siah is a paid consultant for Shockwave Medical and opinions expressed are those of the speaker and not necessarily those of Shockwave Medical.
In the United States: Rx only.
Indications for Use. The Shockwave Medical Intravascular Lithotripsy (IVL) System is intended for lithotripsy-enhanced balloon dilatation of lesions, including calcified lesions, in the peripheral vasculature, including the iliac, femoral, ilio-femoral, popliteal, infra-popliteal, and renal arteries. Not for use in the coronary or cerebral vasculature.
Contraindications. Do not use if unable to pass 0.014 guidewire across the lesion. Not intended for treatment of in-stent restenosis or in coronary, carotid, or cerebrovascular arteries.
Warnings. Only to be used by physicians who are familiar with interventional vascular procedures. Physicians must be trained prior to use of the device. Use the generator in accordance with recommended settings as stated in the Operator’s Manual.
Precautions. Use only the recommended balloon inflation medium. Appropriate anticoagulant therapy should be administered by the physician. Decision regarding use of distal protection should be made based on physician assessment of treatment lesion morphology.
Adverse effects. Possible adverse effects consistent with standard angioplasty include access site complications; allergy to contrast or blood thinner; arterial bypass surgery; bleeding complications; death; fracture of guidewire or device; hypertension/hypotension; infection/sepsis; placement of a stent; renal failure; shock/pulmonary edema; target vessel stenosis or occlusion; vascular complications. Risks unique to the device and its use: allergy to catheter material(s); device malfunction or failure; excess heat at target site.
Prior to use, please reference the Instructions for Use for more information on indications, contraindications, warnings, precautions, and adverse events. www.shockwavemedical.com
Please contact your local Shockwave representative for specific country availability and refer to the Shockwave S4, Shockwave M5, and Shockwave M5+ instructions for use containing important safety information.
REFERENCES
1. Ballotta E, Gruppo M, Mazzalai F, Da Giau G. Common femoral artery endarterectomy for occlusive disease: an 8-year single-center prospective study. Surgery. 2010;147(2):268-74. doi:10.1016/j.surg.2009.08.004
2. Mukherjee D, Inahara T. Endarterectomy as the procedure of choice for atherosclerotic occlusive lesions of the common femoral artery. Am J Surg. 1989;157(5):498-500. doi:10.1016/0002-9610(89)90644-2
3. Kang JL, Patel VI, Conrad MF, Lamuraglia GM, Chung TK, Cambria RP. Common femoral artery occlusive disease: contemporary results following surgical endarterectomy. J Vasc Surg. 2008;48(4):872-7. doi:10.1016/j.jvs.2008.05.025
4. Imran HM, Hyder ON, Soukas PA. Efficacy and safety of adjunctive drug-coated balloon therapy in endovascular treatment of common femoral artery disease. Cardiovasc Revasc Med. 2019;20(3):210-214. doi:10.1016/j.carrev.2018.06.018
5. Mehta M, Zhou Y, Paty PS, et al. Percutaneous common femoral artery interventions using angioplasty, atherectomy, and stenting.
J Vasc Surg. 2016;64(2):369-379. doi:10.1016/j.jvs.2016.03.418
6. Shammas NW, Shammas GA, Karia R, Khalafallah R, Jones-Miller S, Shammas AN. Two-year outcomes of endovascular interventions of the common femoral artery: a retrospective analysis from two medical centers. Cardiovasc Revasc Med. 2021;24:72-76. doi:10.1016/j.carrev.2020.09.006
7. Siracuse JJ, Van Orden K, Kalish JA, et al. Endovascular treatment of the common femoral artery in the Vascular Quality Initiative. J Vasc Surg. 2017;65(4):1039-1046. doi:10.1016/j.jvs.2016.10.078
8. Cantu D, Jawaid O, Kokkinidis D, et al. Outcomes of drug-coated balloon angioplasty vs. conventional balloon angioplasty for endovascular treatment of common femoral artery atherosclerotic disease. Cardiovasc Revasc Med. 2020;21(7):867-874. doi:10.1016/j.carrev.2019.11.008
9. Kronlage M, Erbel C, Lichtenberg M, et al. Safety and effectiveness of Phoenix atherectomy for endovascular treatment in calcified common femoral artery lesions. Vasa. 2021;50(5):378-386. doi:10.1024/0301-1526/a000960
10. Böhme T, Romano L, Macharzina RR, et al. Outcomes of directional atherectomy for common femoral artery disease. EuroIntervention. 2021;17(3):260-266. doi:10.4244/eij-d-19-00693
11. Brodmann M, Schwindt A, Argyriou A, Gammon R. Safety and feasibility of intravascular lithotripsy for treatment of common femoral artery stenoses. J Endovasc Ther. 2019;26(3):283-287. doi:10.1177/1526602819844998
12. Brodmann M, Werner M, Holden A, et al. Primary outcomes and mechanism of action of intravascular lithotripsy in calcified, femoropopliteal lesions: Results of Disrupt PAD II. Catheter Cardiovasc Interv. 2019;93(2):335-342. doi:10.1002/ccd.27943
13. Adams G, Shammas N, Mangalmurti S, et al. Intravascular lithotripsy for treatment of calcified lower extremity arterial stenosis: initial analysis of the Disrupt PAD III study. J Endovasc Ther. 2020;27(3):473-480. doi:10.1177/1526602820914598
14. CFA PAD OS (3) Shammas, N.W., CRT 2021.