


Acoustic Pulse Thrombolysis Treatment Strategies for Acute Limb Ischemia: An Observational Single-Center Study
Abstract
Objective: The optimal treatment strategy for acute limb ischemia (ALI) from thrombotic occlusion remains controversial. Surgical thrombectomy, catheter-directed thrombolysis, and acoustic pulse thrombolysis (APT) have shown benefits, yet are associated with significant amputations and bleeding complications. APT delivers low-intensity, high-frequency ultrasonic waves accompanied by low-dose thrombolytics. We report our single-center observational experience in patients presenting with ALI and undergoing APT. Methods: A retrospective review was conducted of patients treated with APT for ALI from February 2016 to August 2017 at our facility. We assessed the technical success of APT in the treatment of ALI. We also evaluated the safety and efficacy of two treatment strategies: primary APT with secondary endovascular intervention, and primary endovascular intervention with secondary APT. Results: A total of 19 patients with a mean age of 66 ± 12.4 years were retrospectively studied. Eleven (58%) of the patients were male. There were 10 patients in the primary APT group and 9 in the secondary APT group. A preexisting diagnosis of peripheral arterial disease was present in 14 (74%) patients. The average duration of symptoms at presentation was 3.45 ± 3.26 days, and the mean treatment time with APT was 20.78 ± 3.75 hours in all subjects. Overall technical success was achieved in 17 (89%) patients, with primary APT treatment success of 80% and secondary APT treatment success of 100% (P=.474). In all subjects, 2 (11%) had major complications and 2 (11%) had major amputations with no in-hospital mortality. Conclusions: APT is a safe and effective treatment strategy for ALI, and has a low rate of complications and amputations. Large, randomized, controlled trials are needed to evaluate the timing and duration of APT with optimal timing of endovascular interventions.
VASCULAR DISEASE MANAGEMENT 2019;16(11):E149-E156
Key words: acute limb ischemia, acoustic-pulse thrombolysis, thrombolysis, peripheral artery disease, endovascular intervention
Acute limb ischemia (ALI) occurs when the arterial lumen becomes acutely occluded and disrupts blood perfusion to the distal vessels and tissues, which can lead to ischemia and necrosis if not treated emergently. There are up to 14 million cases of ALI per year, with an in-hospital mortality rate of up to 15% and 1-year mortality rate of 40%.1,2 Emergent diagnosis and rapid intervention are paramount to achieve better outcomes, decrease complications, and preserve limbs.
Surgical thrombectomy and catheter-directed thrombolysis have been the mainstays of therapy and guideline recommendations during the past few decades.3 Surgical thrombectomy is an effective treatment; however, although the clinical relevance of surgical thrombectomy may be disputed, 36% of patients are still found to have residual thrombus after treatment.4 Endovascular treatment is a viable alternative to surgery and is often the preferred treatment modality. The role of catheter-directed thrombolysis has long been validated by trials such as STILE, TOPAS, and Rochester.5-7
Acoustic pulse thrombolysis (APT) has emerged as a contemporary endovascular treatment for arterial and venous thrombosis. APT treatment delivers low-intensity, high-frequency ultrasonic waves, while infusing thrombolytic medication directly into the thrombus.8 The combination of ultrasonic waves with thrombolytic medication causes greater lytic permeation and fibrin dissolution. When compared to catheter-directed thrombolysis in studies, APT has demonstrated non-inferiority in ALI treatment.9,10 The benefits of APT are significantly reduced infusion times (21.29 hours APT vs 56.53 hours catheter-directed thrombolysis, P=.0001) and adverse bleeding events (4.7% APT vs 23.8% catheter-directed thrombolysis, P<.01), which have been the biggest drawbacks to treatment with catheter-directed thrombolysis.11
Failure rates and adverse bleeding events are still high with thrombolytic therapies (catheter-directed thrombolysis or APT), even though they are considered mainstream treatments. Major gaps in research still remain regarding optimal treatment strategies to increase positive outcomes and decrease complications. Contemporary studies have shown that 89% of patients still require adjunct revascularization despite high technical success rates with thrombolytics and that poor distal run-off is a direct predictor of amputation.12
In this observational study, we report the outcomes of a small cohort of ALI patients who were treated with APT therapy. We also report the procedural success of APT, and the safety and efficacy of two treatment strategies: 1) primary APT with secondary endovascular intervention, or 2) primary endovascular intervention with secondary APT.
Methods
A retrospective chart review of patients who received APT treatment for ALI with the EkoSonic (Ekos) Endovascular System (Boston Scientific) was conducted at a community hospital from February 2016 to August 2017. Internal review board approval was obtained from the Western Internal Review Board, and informed consent was waived. Patients were identified by the procedural code for percutaneous arterial thrombolysis, International Classification of Diseases- Clinical Modification 37211. Inclusion criteria included ALI patients with Rutherford class I-IIb who received APT treatment with Ekos, with a follow-up angiogram after the completion of treatment.13 Rutherford class III patients or those who did not have a follow-up angiogram were excluded. Patient demographics, procedural data, complications, and in-hospital outcomes were collected.
Patient Demographics and Presentation
The patient demographics included age, gender, and medical history. Medical history included hypertension, hyperlipidemia, coronary artery disease, diabetes mellitus, smoking status (current or former), peripheral artery disease (PAD), critical limb ischemia, and surgical bypass. Data regarding patient presentation collected included duration of symptoms (days), pulse upon presentation, and Rutherford class.
Procedure and Treatment Strategies
All procedures were performed by interventional cardiologists in the cardiac catheterization laboratory. Collected procedural data included occluded vessel (native or bypass graft), APT duration (hours), amount of lysis achieved, procedural success, and interventions pre and post APT. Endovascular interventional techniques included aspiration thrombectomy, angioplasty, and/or stenting. Based upon initial angiography, the physician chose to treat with either 1) primary APT with secondary endovascular intervention, or 2) primary endovascular intervention with secondary APT. These two treatment strategies progressed as follows.
1) Ekos was placed and APT was infused for a duration that was decided by the interventional cardiologist. The patient was brought back to the cardiac catheterization laboratory after completing treatment and was reevaluated with angiography. Subsequent endovascular intervention was performed as decided by the interventional cardiologist.
2) Initial endovascular intervention was performed as decided by the interventional cardiologist, and Ekos was placed for APT. After APT treatment, the patient was reevaluated with angiography, and based on angiographic results, subsequent endovascular intervention was performed as decided by the interventional cardiologist.
For APT, recombinant tissue plasminogen activator (r-tPA) was used in all patients, with a 1-2 mg initial bolus and an infusion rate of 0.5-2 mg per hour. Adjunctive anticoagulation was given with either enoxaparin or heparin. The duration of APT therapy was up to the discretion of the treating interventional cardiologist. All patients were monitored in the intensive care unit for the duration of APT.
Study Outcomes and Definitions
The amount of lysis achieved was graded as complete, partial, or none. Complete lysis was considered >95% lysis of thrombus with a restoration of in-line flow of the occluded vessel. Partial lysis was defined as <95% lysis of thrombus burden with the restoration of in-line flow of the occluded vessel. No lysis was considered to be no angiographic change in thrombus burden without restoration of in-line flow of the occluded vessel. Procedural success was defined as the achievement of either complete or partial lysis upon angiographic evaluation. If no lysis was achieved, then APT was considered unsuccessful. Pulses after APT were assessed and documented.
Major amputations were documented, and the complications included in the study were in-hospital death, compartment syndrome, retroperitoneal bleed, blood transfusion, major hematoma, and intracranial hemorrhage.
Statistical Analysis
Statistical analyses were performed using SPSS software (version 25.0; IBM Corporation). Continuous variables were displayed as mean ± standard deviation and percentages for categorical data. Comparisons between primary APT and secondary APT strategy were analyzed using Chi-square or Fisher exact test.
Results
Patients
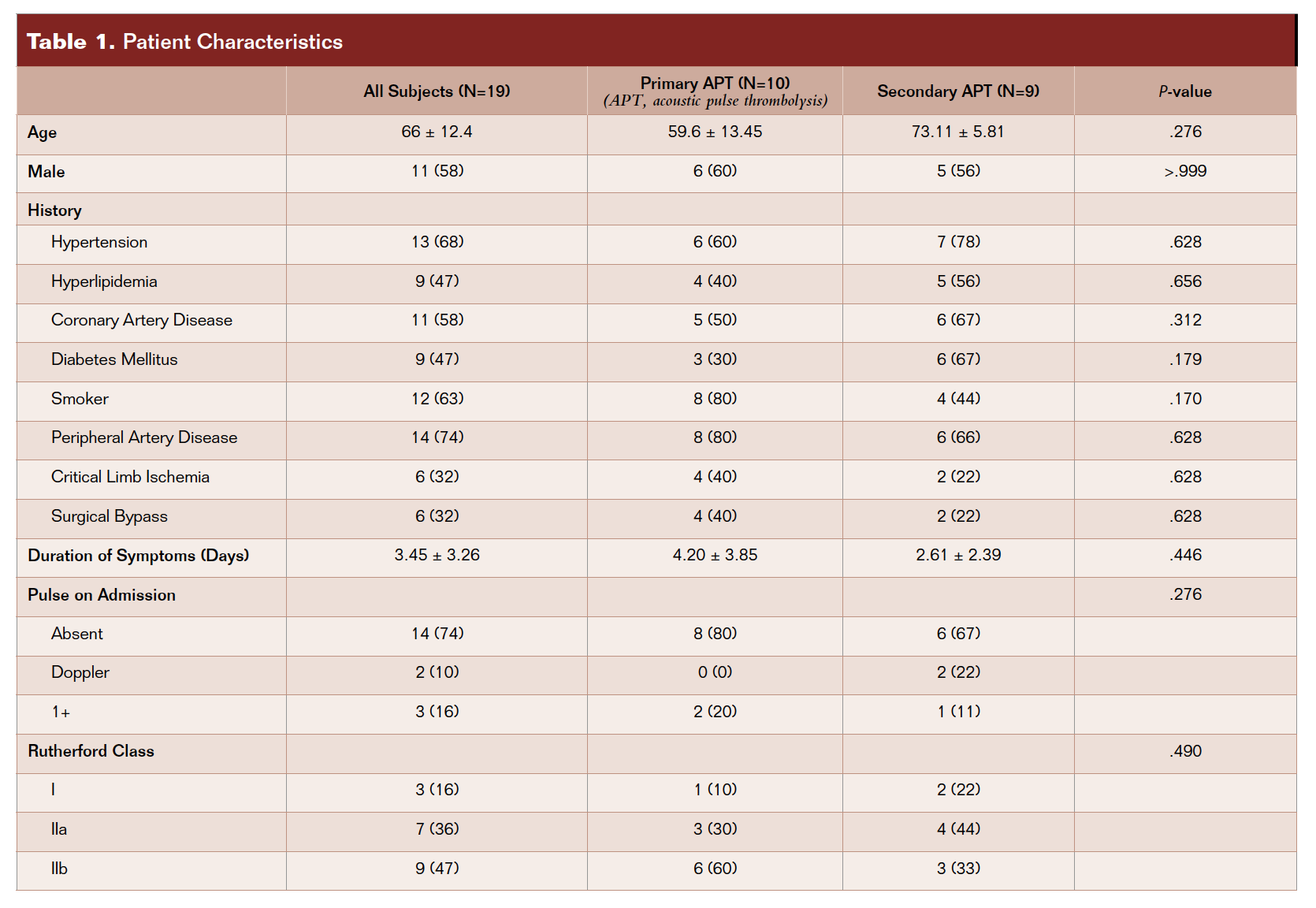 A total of 19 patients were included in the study. There were 10 patients in the primary APT group with secondary endovascular intervention and there were 9 patients in the secondary APT with primary endovascular intervention group. Patient characteristics are included in Table 1 for all subjects and the two treatment groups. In all subjects, 11 (58%) were male, the mean age was 66 ± 12.4 years, and the mean symptom duration was 3.45 ± 3.26 days. There was a high prevalence of history of PAD (74%). Seven (36%) patients were Rutherford class IIa upon presentation, and 9 (47%) were Rutherford class IIb. Fourteen (74%) patients presented with an absent pulse in the affected limb. Demographics in both treatment groups were similar.
A total of 19 patients were included in the study. There were 10 patients in the primary APT group with secondary endovascular intervention and there were 9 patients in the secondary APT with primary endovascular intervention group. Patient characteristics are included in Table 1 for all subjects and the two treatment groups. In all subjects, 11 (58%) were male, the mean age was 66 ± 12.4 years, and the mean symptom duration was 3.45 ± 3.26 days. There was a high prevalence of history of PAD (74%). Seven (36%) patients were Rutherford class IIa upon presentation, and 9 (47%) were Rutherford class IIb. Fourteen (74%) patients presented with an absent pulse in the affected limb. Demographics in both treatment groups were similar.
Procedure and Treatment Outcomes
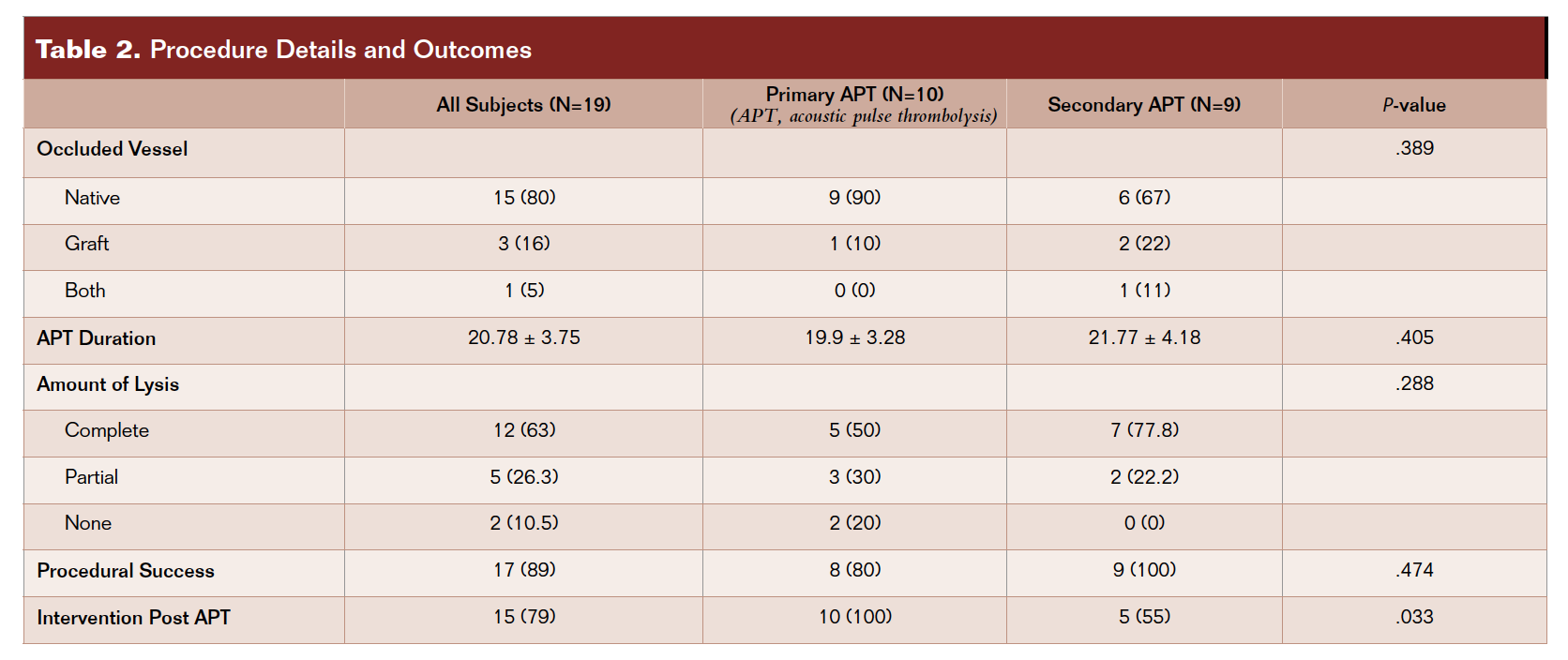 Table 2 includes the procedural data and treatment outcomes for all subjects and both treatment groups. Procedural success in all subjects was achieved in 17 (89%) patients. The mean APT duration was 20.78 ± 3.75 hours. Intervention post APT was performed in 15 (79%) patients. Procedural success was achieved in 8 (80%) patients in the primary APT group and 9 (100%) patients in the secondary APT group (P=.474). Intervention post APT was performed in 10 (100%) patients in the primary APT group and 5 (55%) patients in the secondary APT group (P=.033), which was statistically significant.
Table 2 includes the procedural data and treatment outcomes for all subjects and both treatment groups. Procedural success in all subjects was achieved in 17 (89%) patients. The mean APT duration was 20.78 ± 3.75 hours. Intervention post APT was performed in 15 (79%) patients. Procedural success was achieved in 8 (80%) patients in the primary APT group and 9 (100%) patients in the secondary APT group (P=.474). Intervention post APT was performed in 10 (100%) patients in the primary APT group and 5 (55%) patients in the secondary APT group (P=.033), which was statistically significant.
In-Hospital Outcomes
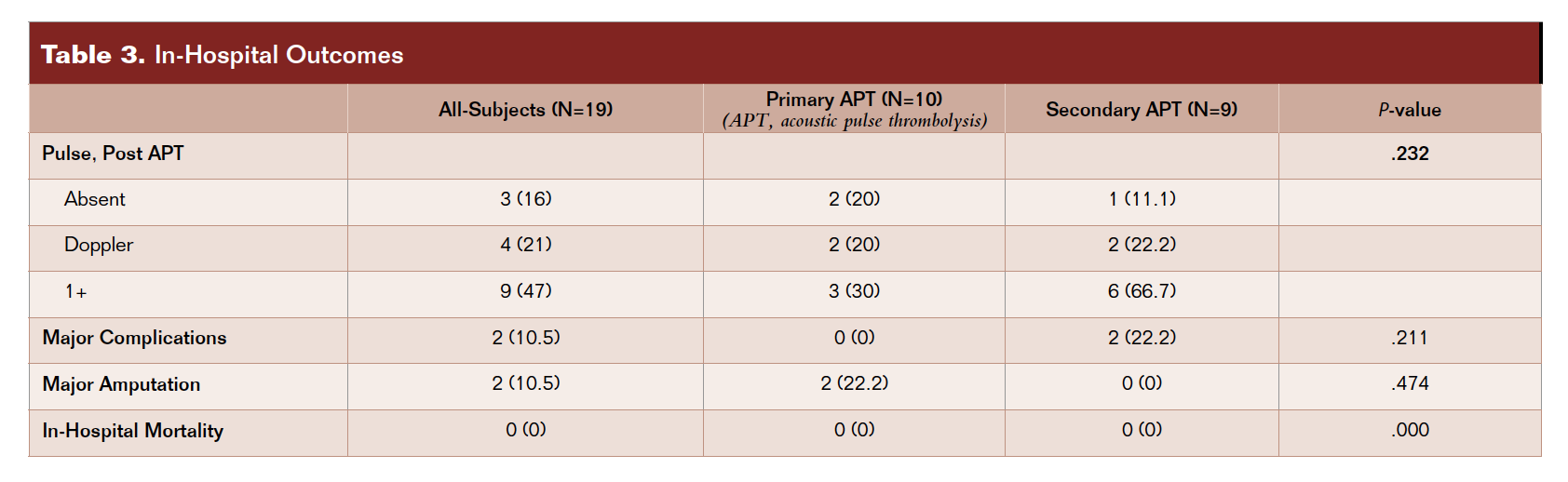 Table 3 includes the in-hospital outcomes. There were 2 (10.5%) amputations that occurred in the primary APT group and 2 (10.5%) complications that occurred in the secondary APT group. The two complications were compartment syndrome that required fasciotomy and a major hematoma at the access site. Three (16%) patients still had absent pulses upon completion of APT. There was no in-hospital mortality, and there was no statistical difference between the two groups.
Table 3 includes the in-hospital outcomes. There were 2 (10.5%) amputations that occurred in the primary APT group and 2 (10.5%) complications that occurred in the secondary APT group. The two complications were compartment syndrome that required fasciotomy and a major hematoma at the access site. Three (16%) patients still had absent pulses upon completion of APT. There was no in-hospital mortality, and there was no statistical difference between the two groups.
 HIGHLIGHTED CASES
HIGHLIGHTED CASES
Case #1
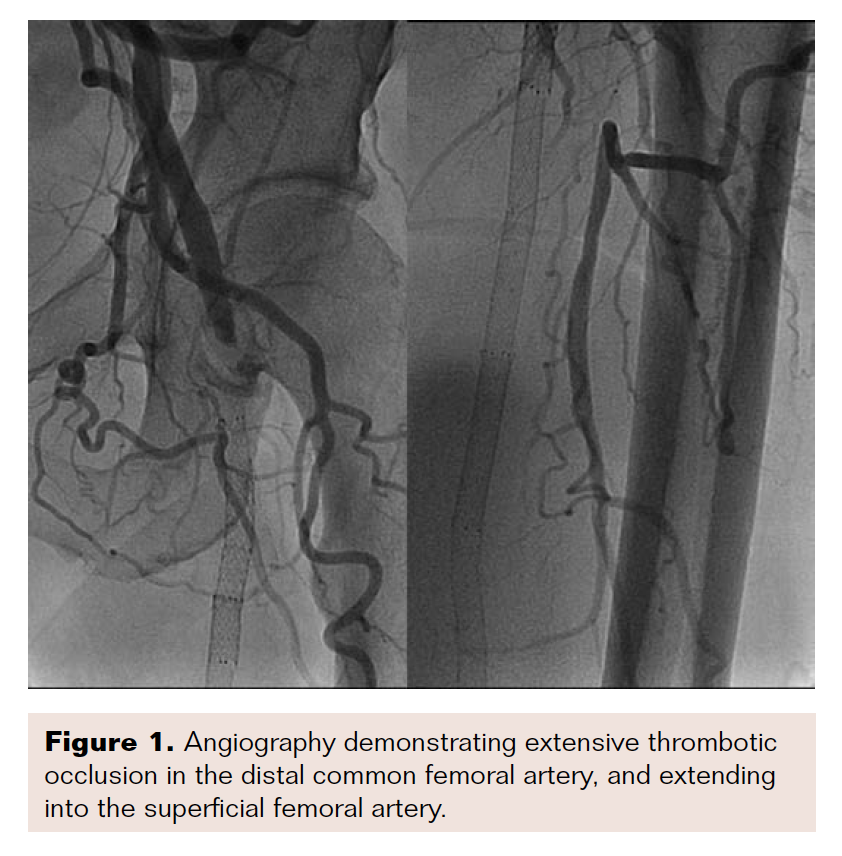
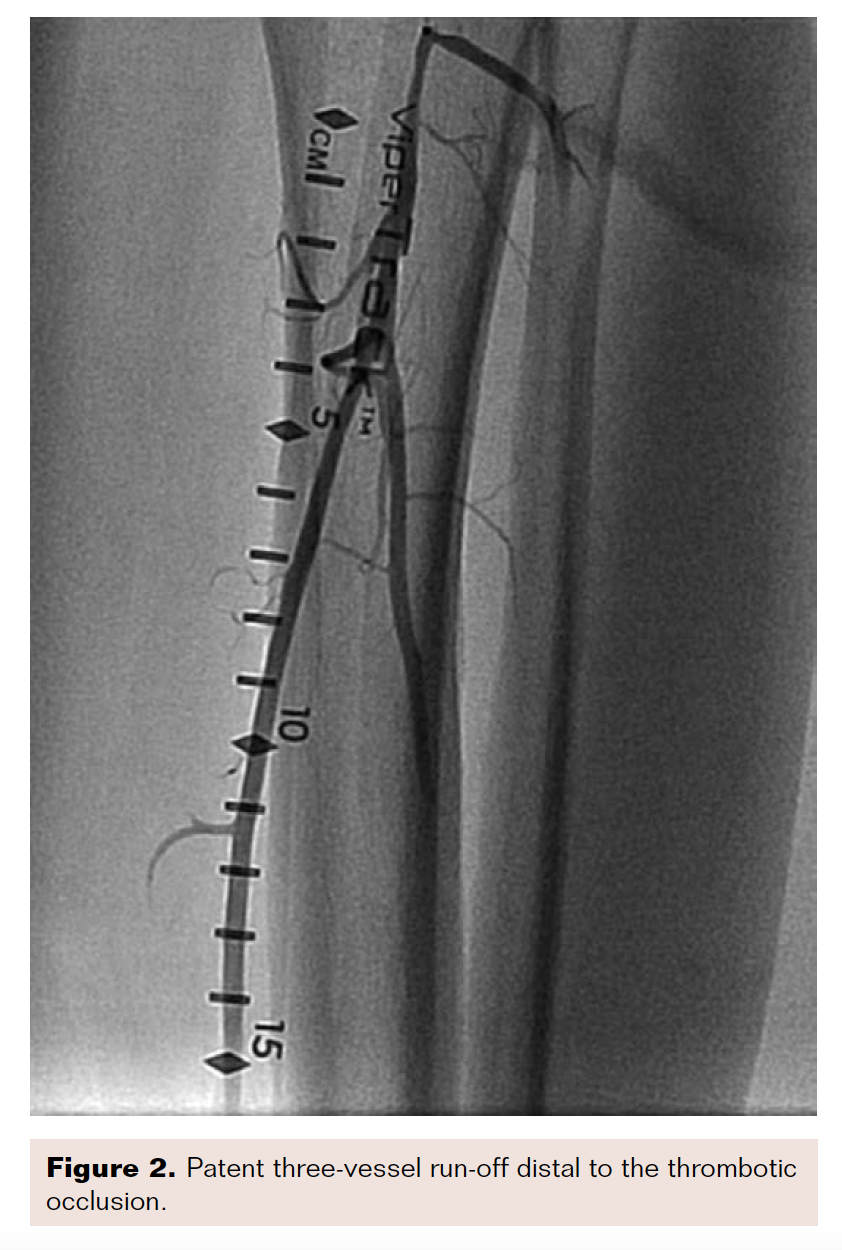
A 50-year-old man with a history of PAD, failed femoral-popliteal bypass grafting, and prior superficial femoral artery (SFA) intervention presented to the emergency department with Rutherford class IIa symptoms that had persisted for one week. Doppler ultrasound showed a possible clot in the left common femoral artery, with poor run-off.
Angiogram revealed acute thrombotic occlusion of the left distal common femoral artery and SFA, with reconstitution at the tibioperoneal trunk (Figures 1-2). Initial balloon angioplasty was performed at the distal common femoral artery and proximal SFA. A 50 cm Ekos catheter was placed from the common femoral artery to the popliteal artery on the left side.
 The patient underwent APT for a duration of three hours. At this time, he reported feeling significantly less pain, and a pulse was palpable in the dorsalis pedis. The Ekos catheter was removed and angiography revealed complete resolution of thrombus, with brisk inflow and outflow (Figure 3). Intravascular ultrasound demonstrated a large area of plaque burden at the distal common femoral and superficial artery junction.
The patient underwent APT for a duration of three hours. At this time, he reported feeling significantly less pain, and a pulse was palpable in the dorsalis pedis. The Ekos catheter was removed and angiography revealed complete resolution of thrombus, with brisk inflow and outflow (Figure 3). Intravascular ultrasound demonstrated a large area of plaque burden at the distal common femoral and superficial artery junction. 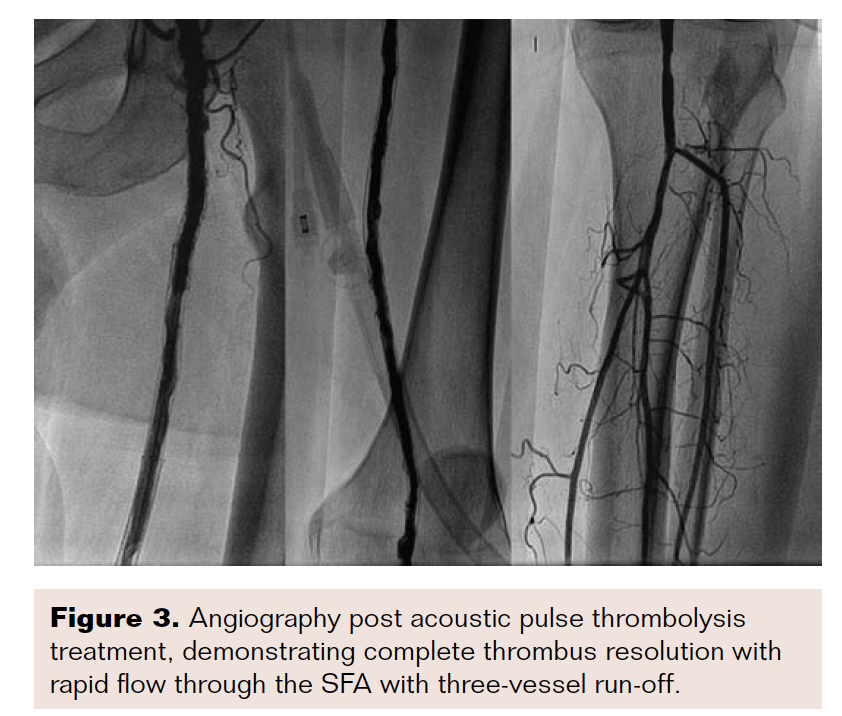 The area of plaque burden was treated with angioplasty and stent placement.
The area of plaque burden was treated with angioplasty and stent placement.
Case #2
A 70-year-old man with a history of left above-knee amputation and recent right femoropopliteal bypass presented to the emergency department with Rutherford class IIb symptoms. Computed tomography angiography demonstrated occlusion of the bypass graft with poor distal flow.
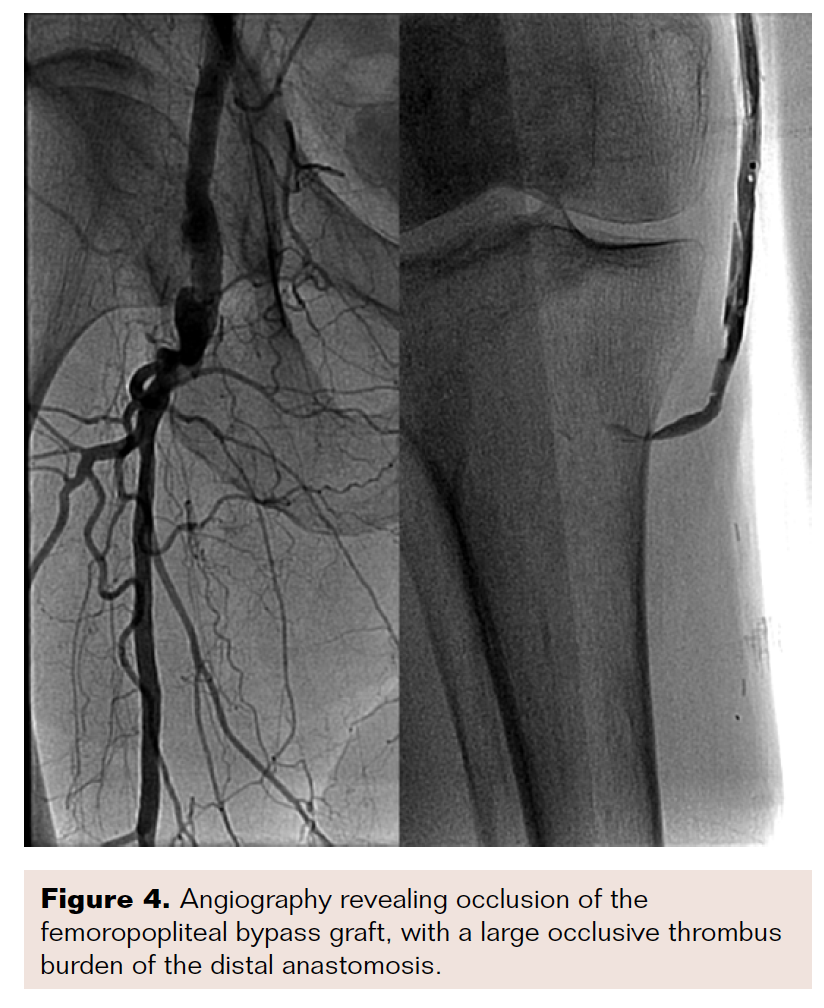 Angiography showed complete occlusion of the graft and very poor run-off past the distal anastomotic site (Figure 4). With some difficulty, a wire and support catheter were passed down into the native tibioperoneal trunk. Angioplasty was performed at the proximal and distal anastomotic sites to increase inflow and outflow. After multiple inflations, a 30 cm Ekos catheter was placed and acoustic pulse thrombolysis was initiated.
Angiography showed complete occlusion of the graft and very poor run-off past the distal anastomotic site (Figure 4). With some difficulty, a wire and support catheter were passed down into the native tibioperoneal trunk. Angioplasty was performed at the proximal and distal anastomotic sites to increase inflow and outflow. After multiple inflations, a 30 cm Ekos catheter was placed and acoustic pulse thrombolysis was initiated.
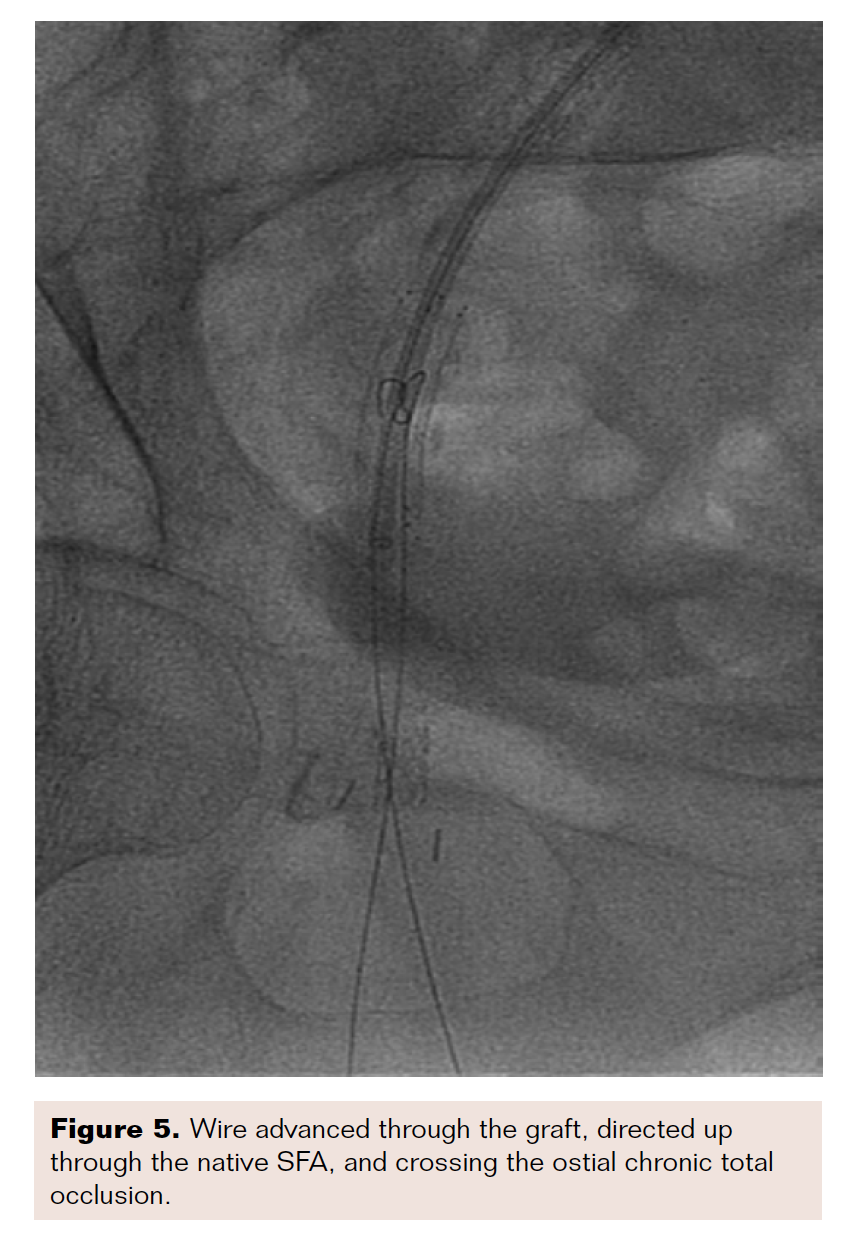
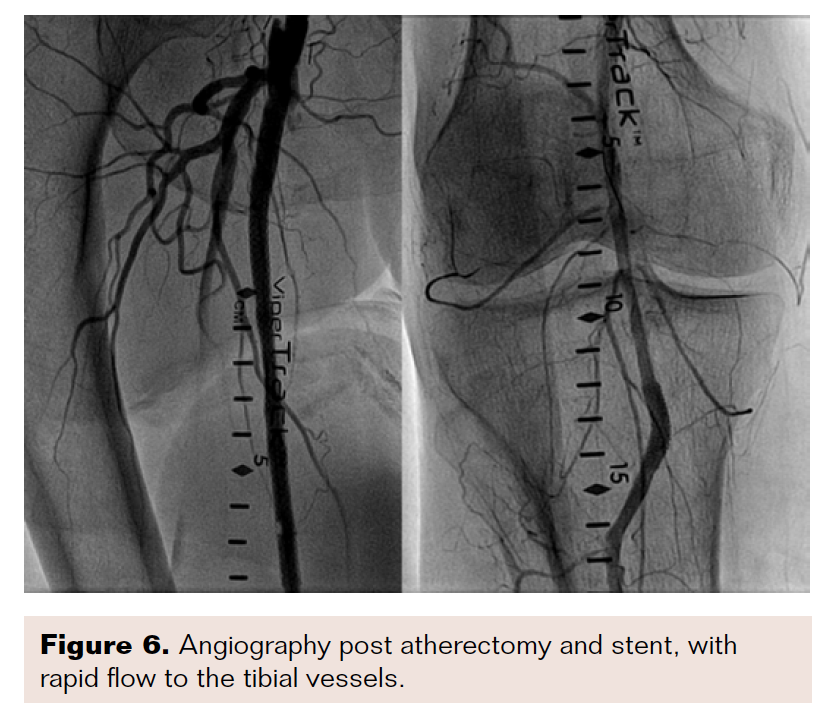
After approximately three hours of acoustic pulse thrombolysis therapy, the patient’s ischemic pain had worsened, and no signs of revascularization were seen. The decision was made to bring the patient back for a repeat angiogram. Subsequent angiography demonstrated no improvement in the thrombus burden and it was decided to proceed with intervention at the native right SFA chronic total occlusion. We used a Quick-Cross catheter (Philips) and V-18 wire (Boston Scientific) and unsuccessfully tried to cross the chronic total occlusion antegrade. We subsequently went through the graft and came retrograde through the distal anastomotic site. We crossed into the common femoral artery and the wire was externalized through the sheath. Atherectomy and stent placement were performed to establish brisk flow to the foot (Figures 5-6).
 DISCUSSION
DISCUSSION
This small, observational study demonstrated that 1) APT is a safe and effective treatment option for patients presenting with ALI, and 2) there were no major differences between two treatment strategies: primary APT with secondary endovascular intervention, or primary endovascular intervention with secondary APT.
The goal of ALI treatment is prompt evaluation, diagnosis, and intervention with a strategy that will provide the most complete revascularization with the lowest procedural risk. Unfortunately, all available treatment modalities (surgical thrombectomy, catheter-directed thrombolysis, and APT) still carry high amputation and subsequent mortality risk.5-7,11,12,14 Even less invasive endovascular procedures such as catheter-directed thrombolysis and APT have been limited by long duration of thrombolytic infusion and subsequent bleeding complications. We believe this small, single-center study is hypothesis-generating and has brought about some interesting observations.
We noticed several cases, especially in the primary APT group, where there was no-reflow phenomenon or poor outflow before and after APT. These scenarios could be due to poor distal flow, significant disease in the distal vessels, stenosis, or plaque rupture blocking adequate forward flow. Furthermore, flow could be blocked by the placement of the Ekos catheter itself. We had hypothesized that performing initial endovascular intervention in a vascular bed that cannot be well visualized with angiography (due to significant thrombus burden) would increase flow to the distal vessels and allow for catheter placement without causing flow obstruction. The endovascular intervention was very promising in our subset of patients, as the technical success was 100%, and no major amputations occurred. Our approach also resulted in significantly lower subsequent endovascular intervention in the same group. After analyzing our results, we made changes to our practice to establish distal flow with primary endovascular intervention and secondary APT therapy. We need a larger patient population to test this hypothesis, with the intention of establishing flow to the distal vascular bed, as we believe that the best treatment for thrombosis is blood flow with concurrent thrombolytic and antithrombotic therapy.
We also observed that the mean duration of symptom onset to presentation/ischemic time in our study group was 3.64 days. This timeframe is longer than previously reported ischemic times of 24 to 29 hours, where the main cause of treatment delay was patient driven.16-19 Abbott and colleagues demonstrated that when ischemia persists for greater than 12 hours without revascularization, the limb salvage rate drops from 93% to 78%.15 Delay in seeking treatment could be contributing to the high rates of amputation in patients with ALI. Patients may confuse lower extremity symptoms for many other disease processes, such as musculoskeletal pain or muscle cramps, and this confusion can cause delays in seeking treatment. It will be interesting to determine whether lower extremity symptoms are more closley related to a delay in seeking medical attention, or to a delay in diagnosis by health care providers. There are well-established protocols and guidelines for ischemia-related conditions in myocardial infarction and stroke. As a result, we think that establishing protocols for early recognition of ALI may help in rapid diagnosis and subsequently better outcomes.20,21 Even though the ischemic time was longer in our study, only two patients with APT treatment had to undergo major amputations.
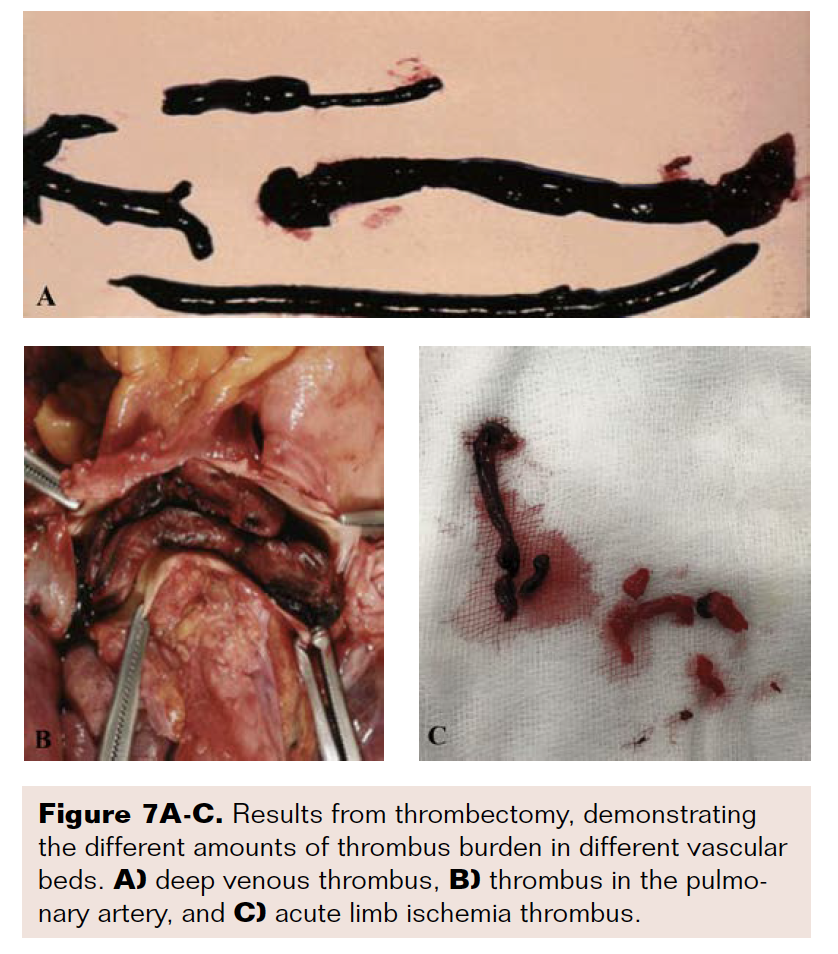 Additionally, a shorter duration of thrombolytic therapy may potentially decrease bleeding complications. The mean duration of treatment for APT in ALI patients in published literature is between 17.7 hours and 21.29 hours.11,12 APT has proven to be a successful treatment modality in patients with PE and DVT in large trials.22,23 The thrombus burden in PE and DVT is much higher than lower extremity arterial thrombosis, as proven by embolectomy (Figure 7). Yet a recent trial (OPTALYSE-PE) demonstrated that low-dose APT therapy can improve clinical symptoms and outcomes, with infusion times as low as 2 hours even in the high thrombus, low-pressure flow system of the lungs.23 Furthermore, Wissgott and colleagues demonstrated that a substantial number of patients with ALI achieved total thrombus dissolution within 6 hours of treatment with 6 mg r-tPA.24 Such evidence substantiates the hypothesis that forward flow is the best treatment for resolution of thrombus with assisted adjunctive pharmaco-mechanic therapy. With this approach in mind, we treated two patients (Cases 1 and 2), with shorter duration of thrombolytic therapy (3 hours). The successful outcomes in these patients could signify that long duration of thrombolytic therapy is not always needed for resolution of thrombus in ALI patients. Also, if flow is not established quickly, as in Case 2, it might be important to quickly convert to different revascularization strategies for establishing blood flow. Conversion to different strategies could potentially decrease ischemic times, lessen the utilization of resources, increase patient comfort, and decrease bleeding complications.
Additionally, a shorter duration of thrombolytic therapy may potentially decrease bleeding complications. The mean duration of treatment for APT in ALI patients in published literature is between 17.7 hours and 21.29 hours.11,12 APT has proven to be a successful treatment modality in patients with PE and DVT in large trials.22,23 The thrombus burden in PE and DVT is much higher than lower extremity arterial thrombosis, as proven by embolectomy (Figure 7). Yet a recent trial (OPTALYSE-PE) demonstrated that low-dose APT therapy can improve clinical symptoms and outcomes, with infusion times as low as 2 hours even in the high thrombus, low-pressure flow system of the lungs.23 Furthermore, Wissgott and colleagues demonstrated that a substantial number of patients with ALI achieved total thrombus dissolution within 6 hours of treatment with 6 mg r-tPA.24 Such evidence substantiates the hypothesis that forward flow is the best treatment for resolution of thrombus with assisted adjunctive pharmaco-mechanic therapy. With this approach in mind, we treated two patients (Cases 1 and 2), with shorter duration of thrombolytic therapy (3 hours). The successful outcomes in these patients could signify that long duration of thrombolytic therapy is not always needed for resolution of thrombus in ALI patients. Also, if flow is not established quickly, as in Case 2, it might be important to quickly convert to different revascularization strategies for establishing blood flow. Conversion to different strategies could potentially decrease ischemic times, lessen the utilization of resources, increase patient comfort, and decrease bleeding complications.
Limitations
There are significant of limitations to our study, given its retrospective nature. Our experience and subsequent analysis is based on a small cohort of patients. Since this is a small patient population, statistical analysis is not powered to compare efficacy or safety outcomes. We believe that there is sound scientific explanation for primary endovascular intervention to establish distal flow and shorten the duration of thrombolytic therapy. This approach could potentially benefit a large number of patients and decrease major amputations, complications, length of hospitalization, and resource utilization. Ideally, primary endovascular intervention to establish distal flow and shorten the duration of thrombolytic therapy should be tested in a large, randomized trial, which is inherently difficult in this patient population. Furthermore, our study did not examine ALI patients who received other forms of therapy, though we made every effort to include patients who underwent endovascular intervention during the study period.
Conclusion
Acoustic pulse thrombolysis is an effective endovascular treatment strategy for patients with ALI. We believe that initial endovascular intervention with the intention of establishing distal blood flow and subsequent shorter duration APT may decrease amputations and bleeding complications. Further research should include larger, randomized studies to prove the efficacy and safety of this treatment modality.
Disclosure: The authors report no financial relationships or conflicts of interest regarding the content herein.
Manuscript submitted, April 27, 2019; manuscript accepted, August 2, 2019.
Address for correspondence: Joji J. Varghese, MD, FACC, FSCAI; Hendrick Medical Center, 1900 Pine Street, Abilene, Texas, 79601. Email: jvarghese@hendrickhealth.org
REFERENCES
1. Peeters P, Verbist J, Keirse K, Deloose K, Bosiers M. Endovascular management of acute limb ischemia. J Cardiovasc Surg (Torino). 2010;51(3):329-336.
2. Gilliland C, Shah J, Martin JG, Miller MJ, Jr. Acute limb ischemia. Tech Vasc Interv Radiol. 2017;20(4):274-280.
3. Gerhard-Herman MD, Gornik HL, Barrett C, et al. 2016 AHA/ACC Guideline on the management of patients with lower extremity peripheral artery disease: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2017;135(12):e726-e779.
4. Plecha FR, Pories WJ: Intraoperative angiography in the immediate assessment of arterial reconstruction. Arch Surg. 1972;105(6):902-907.
5. Comerota AJ, Weaver FA, Hosking JD, et al. Results of a prospective randomized trial evaluating surgery versus thrombolysis for ischemia of the lower extremity. The STILE trial. Ann Surg.1994; 220(3):251-268.
6. Ouriel K, Shortell CK, DeWeese JA, et al. A comparison of thrombolytic therapy with operative revascularization in the initial treatment of acute peripheral arterial ischemia. J Vasc Surg. 1994; 19(6):1021-1030.
7. Ouriel K, Veith FJ, Sasahara AA. A comparison of recombinant urokinase with vascular surgery as initial treatment for acute arterial occlusion of the legs. Thrombolysis or Peripheral Arterial Surgery (TOPAS) Investigators. N Engl J Med. 1998; 338(16):1105-1111.
8. Soltani A, Volz KR, Hansmann DR. Effect of modulated ultrasound parameters on ultrasound-induced thrombolysis. Phys Med Biol. 2008;53(23):6837-6847.
9. Raabe RD. Ultrasound-accelerated thrombolysis in arterial and venous peripheral occlusions: fibrinogen level effects. J Vasc Interv Radiol. 2010;21(8):1165-1172.
10. Schrijver AM, van Leersum M, Fioole B, et al. Dutch randomized trial comparing standard catheter-directed thrombolysis and ultrasound-accelerated thrombolysis for arterial thromboembolic infrainguinal disease (DUET). J Endovasc Ther. 2015; 22(1):87-95.
11. Litzendorf M, Satiani B, Bline K, Starr J. Ultrasound-accelerated thrombolysis has higher success and limb salvage rages and similar costs compared to catheter-directed thrombolysis for acute limb ischemia. J Cardiol Curr Res. 2016;7(2):e1-e6.
12. Byrne RM, Taha AG, Avgerinos E, Marone LK, Makaroun MS, Chaer RA. Contemporary outcomes of endovascular interventions for acute limb ischemia. J Vasc Surg. 2014;59(4):988-995.
13. Rutherford RB, Baker JD, Ernst C, et al. Recommended standards for reports dealing with lower extremity ischemia: revised version. J Vasc Surg. 1997;26(3):517-538.
14. Eliason JL, Wainess RM, Proctor MC, et al. A national and single institutional experience in the contemporary treatment of acute lower extremity ischemia. Ann Surg. 2003;238(3):382-389.
15. Abbott WM, Maloney RD, McCabe CC, Lee CE, Wirthlin LS. Arterial embolism: a 44-year perspective. Am J Surg. 1982;143(4):460-464.
16. Londero LS, Nørgaard B, Houlind K. Patient delay is the main cause of treatment delay in acute limb ischemia: an investigation of pre- and in-hospital time delay. World J Emerg Surg. 2014;9(1):56.
17. Normahani P, Standfield NJ, Jaffer U: Sources of delay in the acute limb ischemia patient pathway. Ann Vasc Surg.2017;38:279-285.
18. Morris-Stiff G, D'Souza J, Raman S, Paulvannan S, Lewis MH. Update experience of surgery for acute limb ischaemia in a district general hospital - are we getting any better? Ann R Coll Surg Engl.2009; 91(8):637-640.
19. Burgess NA, Scriven MW, Lewis MH. An 11-year experience of arterial embolectomy in a district general hospital. J Roy Coll Surg Edinb. 1994; 39(2):93-96.
20. Powers WJ, Derdeyn CP, Biller J, et al. 2015 American Heart Association/American Stroke Association focused update of the 2013 guidelines for the early management of patients with acute ischemic stroke regarding endovascular treatment. Stroke. 2015;46(10):3020-3035.
21. O'Gara PT, Kushner FG, Ascheim DD, et al. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction. Circulation. 2013;127(4):e362-e425.
22. Kucher N, Boekstegers P, Müller OJ, et al. Randomized, controlled trial of ultrasound-assisted catheter-directed thrombolysis for acute intermediate-risk pulmonary embolism. Circulation. 2014;129(4):479-486.
23. Tapson VF, Sterling K, Jones N, et al. A randomized trial of the optimum duration of acoustic pulse thrombolysis procedure in acute intermediate-risk pulmonary embolism: the OPTALYSE PE trial. JACC Cardiovasc Interv. 2018;11(14):1401-1410.
24. Wissgott C, Richter A, Kamusella P, Steinkamp HJ. Treatment of critical limb ischemia using ultrasound-enhanced thrombolysis (PARES Trial): final results. J Endovasc Ther. 2007; 14(4):438-443.
