

Complex Endovascular Repair of Concurrent Ruptured Arch and Descending Thoracic Aortic Aneurysms in a Patient with a Previously Replaced Abdominal Aorta
Abstract
Objective. To present a challenging case of a patient with contained ruptured aneurysm of her aortic arch as well as a saccular aneurysm of the descending thoracic aorta with a history of previously repaired abdominal aortic aneurysm. Methods. Technical considerations for the placement of the endograft required us to perform extra anatomic reconstruction in the form of a right carotid to left carotid artery bypass, and a left carotid to left subclavian artery bypass. This provided the 2 cm proximal landing zone required for endovascular repair of the arch aneurysm. A 34 x 34 x 115 mm Talent (Medtronic EndoVascular, Minneapolis, Minnesota) thoracic graft was used to exclude the arch aneurysm. In addition, a separate 32 x 32 x 48 mm Talent cuff graft was used to exclude the saccular aneurysm located in the descending thoracic aorta. The intervening native aorta was left untouched. Results. The patient recovered well with no evidence of paralysis. Conclusion. When planning the repair of an aortic aneurysm, consideration must be given not only to the ability to cover the aneurysm, but to the consequences of doing so. We feel that precautions should be taken to cover as little of the native aorta as possible to decrease the associated risk of paraplegia in patients whose abdominal aorta has been replaced.
VASCULAR DISEASE MANAGEMENT 2011;8(6):E113–E115
Clinical History
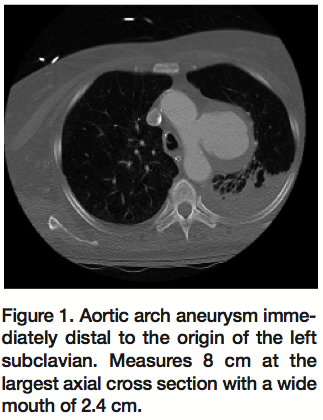
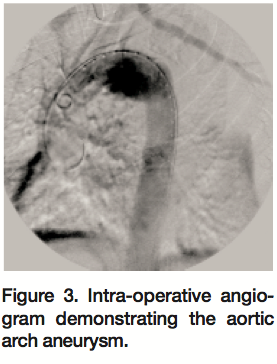
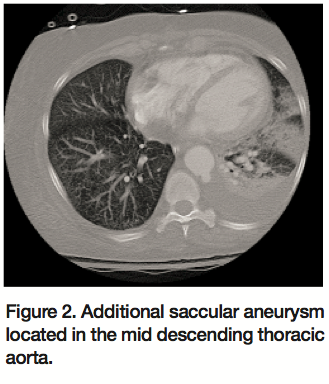 The patient is a 67-year-old African American female with a past medical history significant for chronic obstructing pulmonary disease, hypertension, and deep vein thrombosis with pulmonary embolism who was transferred to our institution for evaluation of repair of an aneurysm of the ascending aorta and transverse arch of the aorta. She had undergone an open repair of an acutely symptomatic abdominal aortic aneurysm 3 months prior. The patient was admitted to an outside facility due to severe flank pain; imaging at that time showed an acute increase in the size of her aortic arch to 7.4 x 6.7 cm. Repeat imaging at our institution showed the aneurysm to have further increased in size to 8 cm with surrounding hematoma; therefore, a diagnosis of contained rupture of the aneurysm was made (Figures 1 and 2). Preoperative angiogram demonstrated the 8 cm aortic arch aneurysm (Figure 3) as well as a second saccular aneurysm located in the mid thoracic aorta. Owing to the patient’s multiple comorbidities, the decision was made to repair the aneurysms endovascularly to prevent exsanguination and death.
The patient is a 67-year-old African American female with a past medical history significant for chronic obstructing pulmonary disease, hypertension, and deep vein thrombosis with pulmonary embolism who was transferred to our institution for evaluation of repair of an aneurysm of the ascending aorta and transverse arch of the aorta. She had undergone an open repair of an acutely symptomatic abdominal aortic aneurysm 3 months prior. The patient was admitted to an outside facility due to severe flank pain; imaging at that time showed an acute increase in the size of her aortic arch to 7.4 x 6.7 cm. Repeat imaging at our institution showed the aneurysm to have further increased in size to 8 cm with surrounding hematoma; therefore, a diagnosis of contained rupture of the aneurysm was made (Figures 1 and 2). Preoperative angiogram demonstrated the 8 cm aortic arch aneurysm (Figure 3) as well as a second saccular aneurysm located in the mid thoracic aorta. Owing to the patient’s multiple comorbidities, the decision was made to repair the aneurysms endovascularly to prevent exsanguination and death.
Procedure
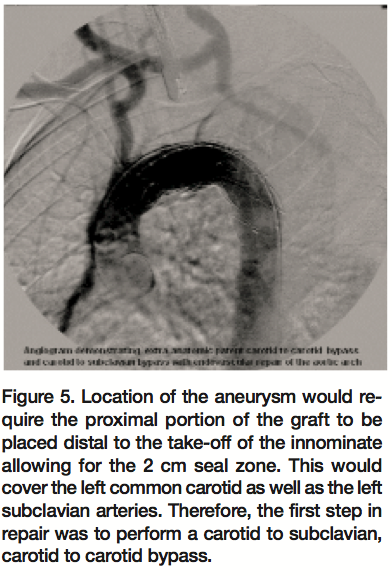
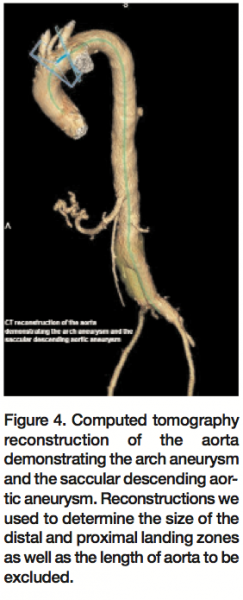 The proximal location of the arch aneurysm would require the proximal landing zone to be at the distal border of the innominate artery. This would provide the 2 cm of normal aorta as the fixation area for the endograph (Figure 4). This would cover the left common carotid artery as well as the subclavian artery; therefore, the first step in the repair of this aneurysm was a left carotid artery to left subclavian artery, left carotid artery to left carotid artery bypass (Figure 5). This was performed using a 10 mm Hemashield graft (Boston Scientific, Natick, Massachusetts). The proximal left carotid artery was ligated and the proximal left subclavian artery was occluded using Nester coils (Cook Medical, Bloomington, Indiana). Due to the patient’s multiple comorbidities, it was felt that a debranching procedure with median sternotomy would not be well tolerated.
The proximal location of the arch aneurysm would require the proximal landing zone to be at the distal border of the innominate artery. This would provide the 2 cm of normal aorta as the fixation area for the endograph (Figure 4). This would cover the left common carotid artery as well as the subclavian artery; therefore, the first step in the repair of this aneurysm was a left carotid artery to left subclavian artery, left carotid artery to left carotid artery bypass (Figure 5). This was performed using a 10 mm Hemashield graft (Boston Scientific, Natick, Massachusetts). The proximal left carotid artery was ligated and the proximal left subclavian artery was occluded using Nester coils (Cook Medical, Bloomington, Indiana). Due to the patient’s multiple comorbidities, it was felt that a debranching procedure with median sternotomy would not be well tolerated.
 Due to the small size of the external iliac artery, a 10 mm Hemashield graft was sewn into the distal right external iliac artery in order to allow for the graft device to be introduced into the aorta.
Due to the small size of the external iliac artery, a 10 mm Hemashield graft was sewn into the distal right external iliac artery in order to allow for the graft device to be introduced into the aorta.
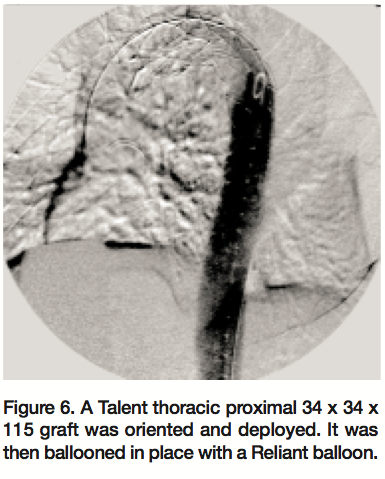
After a series of intra-operative measurements were done to confirm the preoperative planning, a 34 x 34 x 115 mm Talent thoracic proximal main graft (Medtronic EndoVascular) was appropriately oriented and deployed (Figures 5 and 6). It was then ballooned in place with a Reliant balloon (Cook Medical, Bloomington, Indiana).
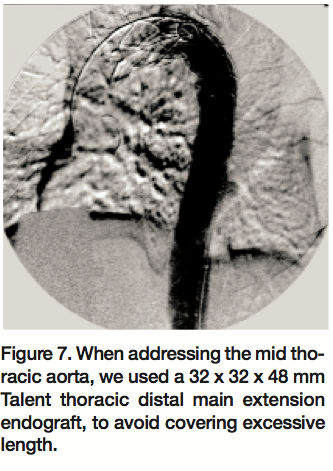
 Attention was then turned to a second saccular aneurysm located in the mid thoracic aorta. The native aorta measured about 28 mm at this site. In order to avoid covering excessive length of the descending thoracic aorta, a 32 x 32 x 48 mm Talent thoracic distal main extension endograft was used (Figure 7).
Attention was then turned to a second saccular aneurysm located in the mid thoracic aorta. The native aorta measured about 28 mm at this site. In order to avoid covering excessive length of the descending thoracic aorta, a 32 x 32 x 48 mm Talent thoracic distal main extension endograft was used (Figure 7).
At the conclusion of the procedure, the decision was made to place a spinal drain based on the patient’s decreased level of alertness and inability to cooperate with physical exam evaluations of her extremities.
Results
 The completion angiogram demonstrated excellent results with the exclusion of the ruptured arch aneurysm and no endoleak. The innominate artery was widely patent and the extra anatomic carotid-carotid bypass graft, as well as the carotid-subclavian bypass graft, were all clearly visualized with excellent flow (Figures 5 and 6). After deployment of the graft over the second saccular aneurysm, angiogram demonstrated complete exclusion of this aneurysm as well (Figure 7).
The completion angiogram demonstrated excellent results with the exclusion of the ruptured arch aneurysm and no endoleak. The innominate artery was widely patent and the extra anatomic carotid-carotid bypass graft, as well as the carotid-subclavian bypass graft, were all clearly visualized with excellent flow (Figures 5 and 6). After deployment of the graft over the second saccular aneurysm, angiogram demonstrated complete exclusion of this aneurysm as well (Figure 7).
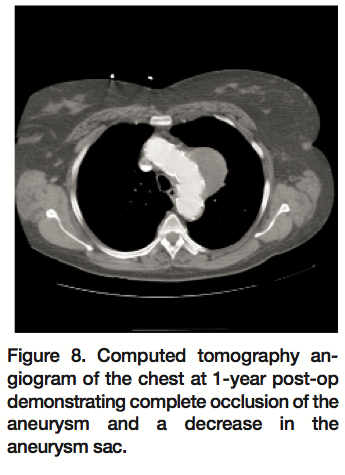 The patient is currently 1 year out from her surgery and is alive and well with no reported musculoskeletal weakness. She had a 1-year follow-up computed tomography angiogram of her chest, which showed the aortic arch aneurysm sac to still be completely excluded by the graft and a decrease in size of the aortic arch aneurysm from 7.4 x 6.7 cm to 6.4 x 5.6 cm (Figure 8). The second saccular aneurysm that was in the mid thoracic aorta is no longer seen.
The patient is currently 1 year out from her surgery and is alive and well with no reported musculoskeletal weakness. She had a 1-year follow-up computed tomography angiogram of her chest, which showed the aortic arch aneurysm sac to still be completely excluded by the graft and a decrease in size of the aortic arch aneurysm from 7.4 x 6.7 cm to 6.4 x 5.6 cm (Figure 8). The second saccular aneurysm that was in the mid thoracic aorta is no longer seen.
Discussion
The risk of paraplegia is significantly decreased with endovascular repair; however, a finite risk is still present.3,4 There is a reported approximate 1.7% risk of paraplegia with TEVAR alone, which increases to approximately 12.5% with a history of previous or concomitant abdominal aortic aneurysm repair.1 Contributing to the risk of spinal cord ischemia are increased length of aortic coverage as well as increased length of time between repair of abdominal aorta and thoracic aorta.4,6,7
Thoracic aortic aneurysms can be extremely devastating, with a high mortality rate associated with rupture.2 Therefore, it is imperative that the aorta is repaired in this patient population. Our patient not only had a large aneurysm in the arch of her aorta, but also rapid expansion and surrounding hematoma, leading to the diagnosis of a contained rupture of the arch aneurysm. In addition, a saccular aneurysm was located in the descending thoracic aorta. Using one contiguous graft to repair the multiple aneurysms posed an unacceptably high risk of paralysis, but leaving the aneurysms to progress to free rupture was obviously not an option as well.
The technical considerations for this procedure were great. In order to achieve the appropriate 2 cm landing seal zone required by the endovascular device,5 it was clear that the origin of the left subclavian artery as well as the left common carotid artery would have to be covered by the device. Therefore, it was necessary to perform a carotid to subclavian, then a subclavian to subclavian bypass, to ensure perfusion to the brain and left upper extremity.5
Finally, there was consideration that needed to be given to the saccular aneurysm located in the descending thoracic aorta, which also required attention. To place a long graft to extend from the aneurysmal aortic arch down to the saccular aneurysm would directly increase the risk of spinal cord ischemia in light of her previous abdominal aortic aneurysm repair. However, not repairing this aneurysm would have exposed the patient to risk of rupture and death, versus the risk of paraplegia with repair. To minimize the risk of spinal cord ischemia, we placed a cuff, just covering the aneurysmal area and allowing for as much native healthy aorta to be left uncovered as possible.
This case highlights the importance of limited coverage of the thoracic aorta when the abdominal aorta has been replaced. To our knowledge, this is a unique report of a durable endovascular repair of a ruptured aneurysm in the arch of the aorta and a separate saccular aneurysm in the descending thoracic aorta treated with 2 separate stent grafts with intervening normal native aorta.
References
- Schlösser FJ, Verhagen HJ, Lin PH, et al. TEVAR following prior abdominal aortic aneurysm surgery: Increased risk of neurological deficit. J Vasc Surg 2009;49:308–314; discussion, p. 314; Epub 2008 Dec 20.
- Abraha I, Romagnoli C, Montedori A, Cirocchi R. Thoracic stent graft versus surgery for thoracic aneurysm. Cochrane Database Syst Rev 2009 Jan 21;(1):CD006796.
- Cheng D, Martin J, Shennib H, et al. Endovascular aortic repair versus open surgical repair for descending thoracic aortic disease: A systematic review and meta-analysis of comparative studies. J Am Coll Cardiol 2010;55:986–1001.
- Feezor RJ, Lee WA. Strategies for detection and prevention of spinal cord ischemia during TEVAR. Semin Vasc Surg 2009;22:187–192.
- Schoder M, Lammer J, Czerny M. Endovascular aortic arch repair: Hopes and certainties. Eur J Vasc Endovasc Surg 2009;38:255–261.
- Martin DJ, Martin TD, Hess PJ, et al. Spinal cord ischemia after TEVAR in patients with abdominal aortic aneurysms. J Vasc Surg 2009;49:302–306.
- Matsuda H, Fukuda T, Iritani O, et al. Spinal cord injury is not negligible after TEVAR for lower descending aorta. Eur J Vasc Endovasc Surg 2010;39:179–186.
_______________________________________
From the Department of Surgery, Inova Fairfax Hospital, Falls Church, Virginia.
The authors report no financial relationships or conflicts of interest regarding the content herein.
Manuscript submitted February 16, 2011, provisional acceptance given April 14, 2011, final version accepted April 18, 2011.
Address for correspondence: Vaishali T. Kent, MD, Inova Fairfax Hospital, Department of Surgery, 3300 Gallows Road, Falls Church, VA 22042. Email: vtrivedi21@hotmail.com
