Endovascular Management of Splanchnic Aneurysms
Abstract
Background. Splanchnic aneurysms are an important cause of gastrointestinal bleeds with different endovascular treatment options. Method. This retrospective study included all aneurysms involving the splanchnic arteries that were referred to our department for endovascular treatment over a period of more than 10 years (June 2002 through December 2012). Results. 63 patients were included in the study. A high success rate of 92% was seen overall. Two patients underwent successful embolization but died due to causes unrelated to the bleeding. Rebleeding occurred in four patients (8%). Two patients underwent repeat embolization and one underwent surgery with good results. A repeat angiogram did not reveal a source of bleed in the fourth patient and he continued to bleed and died despite blood transfusions and inotroic supports. Few complications were seen. Conclusion. Excellent results for treatment of splanchic aneurysms can be achieved with proper planning and choice of technique.
VASCULAR DISEASE MANAGEMENT 2013:10(1):E5-E10
Key words: interventional radiology, mesenteric artery interventions, pseudoaneurysm, vascular intervention
_____________________________________________
Excellent success rates have been achieved with different endovascular techniques in the treatment of splanchnic aneurysms. This pictorial essay describes the endovascular management of different splanchnic aneurysms.
Method
This was a retrospective study that included all aneurysms involving the splanchnic arteries that were referred to our department for endovascular treatment over a period of more than 10 years (from June 2002 to December 2012).
Results
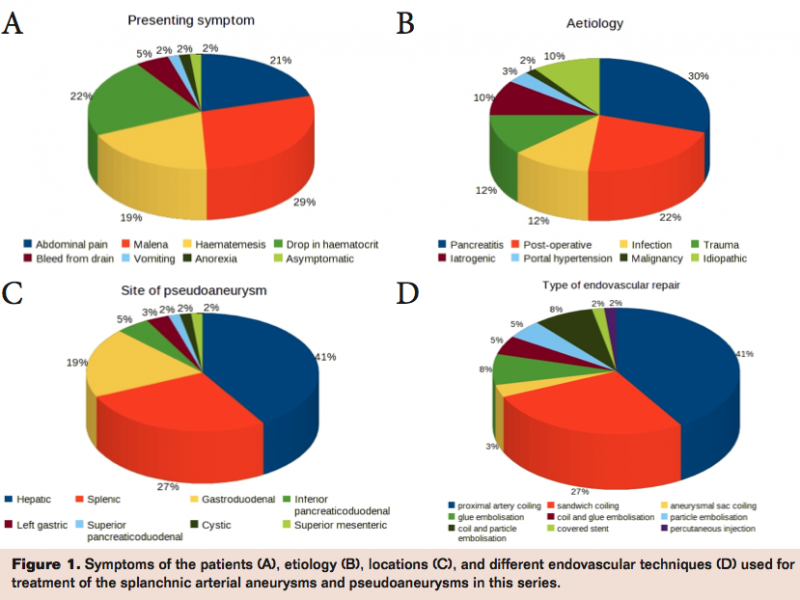
63 patients were included in this study. Males were more common than females (4.7:1) and more than half of the patients were in the 30 to 60 year age group. The most common symptoms were abdominal pain, melena, and hematemesis (Figure 1A). Pancreatitis (30%), surgery (22%), infection (12%), and trauma (12%) were the most common causes (Figure 1B). The most common locations were the hepatic artery (41%) and the splenic artery (27%; Figure 1C). The most common endovascular techniques used were proximal coil embolization (41%) and the sandwich technique of coil embolization (27%; Figure 1D). A high success rate of 92% was seen overall. Two patients underwent successful embolization but died due to causes unrelated to the bleeding. Rebleeding occurred in four patients (8%). Two patients underwent repeat embolization and one underwent surgery with good results. A repeat angiogram did not reveal a source of bleed in the fourth patient and he continued to bleed and died despite blood transfusions and inotropic supports. A few complications were seen. Inadvertent dislodgement of an embolization coil into the parent hepatic artery was seen in one patient. A pseudoaneurysm of the hepatic artery ruptured during the coil embolization and was treated with hepatic artery embolization. Subintimal dissection of a gastroduodenal artery occurred and was treated by balloon angioplasty. Cystic necrosis of the spleen was seen on a follow-up CT scan, which was a result of embolization of a splenic pseudoaneurysm with Histacryl n-butyl cyanoacrylate glue (B. Braun).
Discussion
Splanchnic aneurysms are a small but important cause of gastrointestinal bleeds.1 The management of a patient with a splanchnic aneurysm or pseudoaneurysm includes surgical, endovascular, and percutaneous options.2 Surgical approaches include aneurysmorrhaphy, aneurysm excision, and ligation of the parent artery.3 Endovascular options have emerged as the preferred approach especially if the aneurysm has ruptured due to the decreased morbidity and mortality.4
Direct percutaneous puncture of the aneurysm with a 22G needle can be done under ultrasound or CT guidance to inject a thrombogenic agent such as thrombin or n-butyl cyanoacrylate glue into the aneurysmal sac. A patient with abdominal pain and hematemesis due to chronic pancreatitis was detected on CT scan to have a pseudoaneurysm of the gastroduodenal artery. Digital subtraction angiography could not demonstrate either the pseudoaneurysm or the gastroduodenal artery. Since the pseudoaneurysm was well visualised on transabdominal ultrasonography, ultrasound-guided direct percutaneous injection of n-butyl cyanoacrylate glue into the pseudoaneurysm was done. Subsequent doppler studies revealed that the pseudoaneurysm had thrombosed and the patient showed improvement. However, someaneurysms may not be accessible. The injected material could reflux into the main artery and cause thrombosis. The safety of the injection could be increased with temporary balloon occlusion of the parent artery.
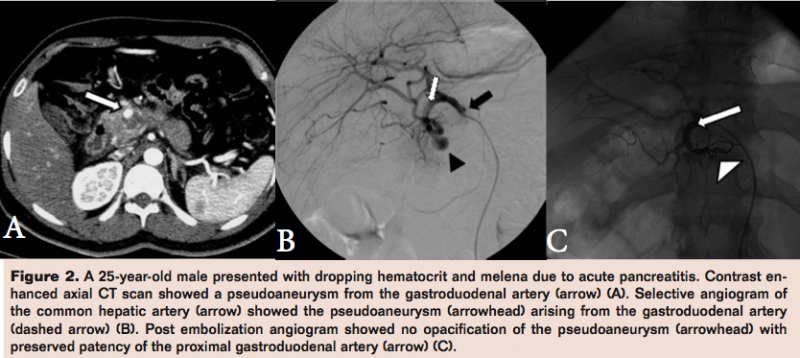
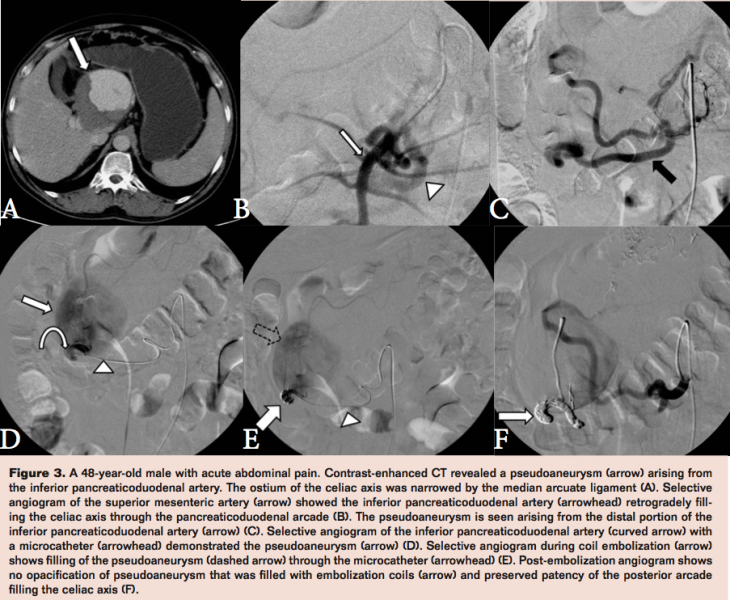
Endovascular treatment options include occlusion of the artery supplying the aneurysm with embolization coils (Figures 2 and 3) or n-butyl cyanoacrylate glue, filling the aneurysm sac with coils and deploying a covered stent in the parent artery acrossthe neck of the pseudoaneurysm.5
Proximal occlusion of the parent artery supplying the pseudoaneurysm is effective. A patient with acute pancreatitis and dropping hematocrit had a pseudoaneurysm of the left gastric artery, which was treated with proximal coil embolization of the left gastric artery (Figure 4).
However, there is a possibilityof retrograde filling of the pseudoaneurysm from a distal artery.
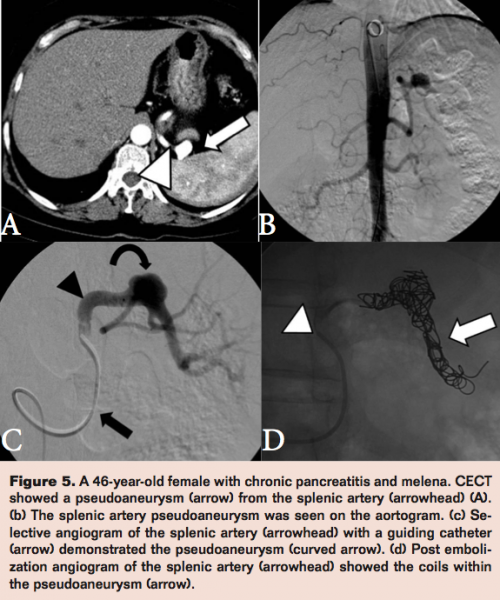
In order to avoid this, the sandwich technique embolizes the parent artery both distally and proximally in relation to the aneurysmal neck. A patient with a splenic artery pseudoaneurysm due to chronic pancreatitis was treated in this way using embolization coils (Figure 5).
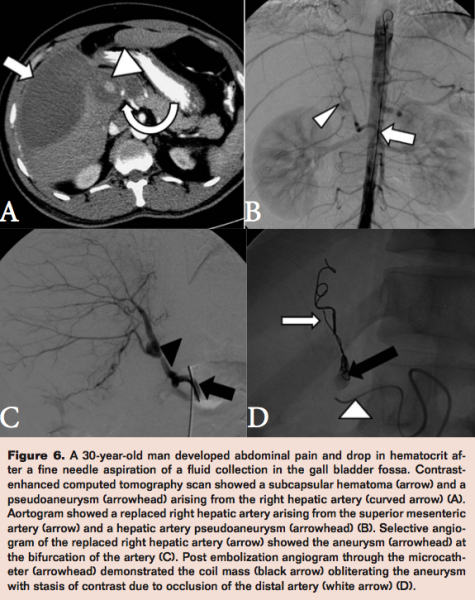
Filling the aneurysmal sac with coils is feasible in smaller aneurysms and preserves the patency of the parent artery. A patient with post-cholecystectomy bleeding underwent coil embolization of a branch of the right hepatic artery but continued to have intermittent hematemesis. Angiogram revealed a pseudoaneurysm at the cystic artery stump.
While filling the aneurysm sac with coils, a loop prolapsed into the right hepatic artery, occluding it (Figure 6). The patient improved gradually.
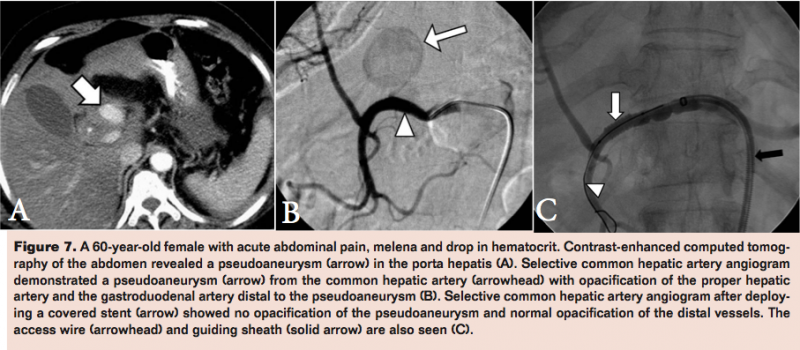
A covered stent has the advantage of preserving the patency of the parent artery while excluding the aneurysm. However, this is a difficult option if the anatomy is tortuous. A patient with abdominal pain and dropping hematocrit due to a large pseudoaneurysm in the common hepatic artery was treated using a covered stent (Figure 7).
Some situations call for a combination of endovascular techniques. A patient with a significant bleed after a liver biopsy underwent angiography, which showed multiple punctate bleeds arising from the replaced right hepatic artery and a focal bleed from a branch of the left hepatic artery.
Both arteries were selectively embolized with polyvinyl alcohol particles. The patient continued to bleed and a repeat angiography showed a small pseudoaneurysm from the right hepatic artery, which was embolized with coils using the sandwich technique followed by a small amount of n-butyl cyanoacrylate glue with successful results.
Conclusion
Splanchnic aneurysms are an important cause of gastrointestinal bleeds with different endovascular treatment options. The choice for treatment depends on the situation, anatomy, and the experience of the interventional radiologist. Excellent results can be achieved with good planning and technique.
References
- Pasha SF, Gloviczki P, Stanson AW, Kamath PS. Splanchnic artery aneurysms. Mayo Clin Proc. 2007;82(4):472-479.
- Sachdev-Ost U. Visceral artery aneurysms: review of current management options. Mt Sinai J Med. 2010;77(3):296-303.
- Sachdev U, Baril DT, Ellozy SH, et al. Management of aneurysms involving branches of the celiac and superior mesenteric arteries: a comparison of surgical and endovascular therapy. J Vasc Surg. 2006;44(4):718-724.
- Tulsyan N, Kashyap VS, Greenberg RK, et al. The endovascular management of visceral artery aneurysms and pseudoaneurysms. J Vasc Surg. 2007;45(2):276-283.
- JL, Chung J, Brevetti LS, Graham AM, Siegel RL. Visceral and renal artery aneurysms: a pictorial essay on endovascular therapy. Radiographics. 2006;26(6):1687-1704.
_________________________________
Editor’s Note: Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript received July 16, 2012; final version accepted August 13, 2012.
Address for correspondence: George Koshy Chiramel, MD, Christian Medical College Vellore, Tamil Nadu, India. Email: gkchiramel@gmail.com