

Four-Year Data Show Long-Term Durability for EndoSuture Aneurysm Repair in Hostile Necks
 Vascular Disease Management talks with William Jordan Jr., MD, Professor of Surgery and Chief, Division of Vascular Surgery and Endovascular Therapy at Emory University School of Medicine, in Atlanta, Georgia.
Vascular Disease Management talks with William Jordan Jr., MD, Professor of Surgery and Chief, Division of Vascular Surgery and Endovascular Therapy at Emory University School of Medicine, in Atlanta, Georgia.
Four-year follow-up data from the ANCHOR registry, which captures long-term outcomes of ESAR (EndoSuture Aneurysm Repair) with the Heli-FX EndoAnchor System (Medtronic) and commercially available grafts, was presented by William Jordan Jr., MD, Professor of Surgery and Chief, Division of Vascular Surgery and Endovascular Therapy at Emory University School of Medicine and Jean-Paul de Vries, MD, currently Chair of the Department of Surgery at University Medical Center Groningen, in Groningen, the Netherlands.
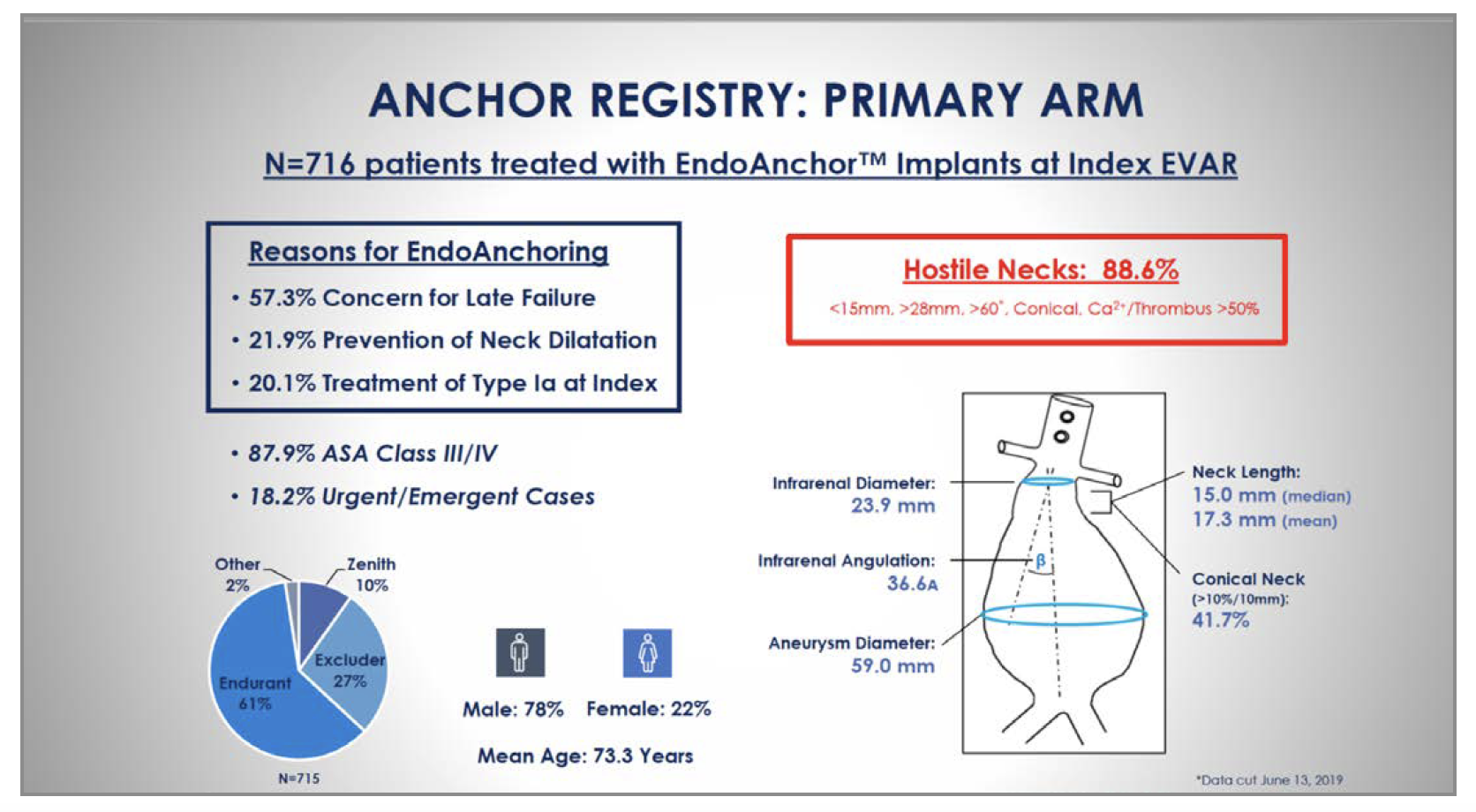
To date, more than 900 patients with abdominal aortic aneurysms (AAA) have been enrolled in the primary and revision arms of the ANCHOR registry. The data presented includes AAA patients treated with ESAR in the primary and revision cohorts of the study who were eligible for clinical and imaging follow-up through 4 years. Both groups included a high percentage (>88%) of patients who met the Society of Vascular Surgery (SVS) definition of hostile aortic necks. A high percentage of EndoAnchors penetrated the aortic wall in both the primary cohort (95.9%) and the revision cohort (93.1%) — a group which consisted of 100% failed endovascular aneurysm repairs (EVARs). The data also demonstrated:
- Freedom from secondary procedures to treat Type Ia endoleak based on Kaplan-Meier estimate:
- Through 4 years: primary= 97.2%; revision= 82.4%
- Positive sac regression despite the hostile anatomy characteristics:
- At 4 years: primary= 62.1%; revision= 32.4%
- Freedom from aneurysm-related mortality (ARM) based on the Kaplan-Meier estimate, which is notable given the hostile neck anatomies of patients in both study arms:
- Through 4 years: primary= 97.7%; revision= 89.7%
Tell us about the ANCHOR registry.
The ANCHOR Registry began in 2012 and was related to the partial success of the STAPLE-1 and STAPLE-2 trials, which were aortic endograft trials that were initiated many years ago. In those trials, a new endograft incorporated the anchors into the primary treatment system. Overall, the graft did not work as intended, but the anchors did work and were approved by the FDA in 2011. The ANCHOR registry was initiated in 2012 and was specifically designed as a prospective, observational study. The objective of the ANCHOR registry was to capture the utilization of the Heli-FX EndoAnchor System in various commercially available endografts and try to understand their application post approval. Our registry gathered patients and was supported as part of small company that was eventually acquired by Medtronic. Medtronic has continued the registry and has grown it to more than 1,000 patients.
Can you describe ESAR (EndoSuture Aneurysm Repair) with the Heli-FX EndoAnchor System?
The ESAR system recreates the surgical anastomosis by placing anchors, or staples, through the aortic endograft into the wall of the aorta. ESAR has a similar, and in some cases greater, strength to that of a stitch made in an open procedure.
ESAR is distinctly different from other available endograft options. Most other endograft options have radial fixation, which involves a spring that helps push against the aortic wall to enable the wall to seal. These endografts then rely on biologic mechanisms to heal in place and provide long-term fixation.
Over the past few decades, grafts have had subtle modifications and include various forms of what is termed “active fixation.” Active fixation typically means that there is a sharp edge or some anchor or barb with which we try to improve the fixation in the aortic wall. The EndoAnchor is 4.4 mm in length and has farther penetration through the graft into the wall, which differentiates it from other current options. Other grafts use seal mechanisms, and some use suprarenal fixation with a more active anchor or some sharp point that will penetrate partially into the aortic wall, but those grafts will not penetrate with the strength or depth of the EndoAnchor.
Can you describe the registry data presented at VEITH?
One of the primary points of the presentation at VEITH was to discuss durability and how the EndoAnchor has continued to work over the longer term. In the last 20 years of endovascular aneurysm repair, we seem to encounter failures between year 2 and year 5, so results from years 4 and 5 have become very important. For example, the implication of the EVAR 1 study was that EVAR works great initially, but may not be adequately durable. In contrast, the 4-year results of the ANCHOR registry are showing that we have good durability with our group of patients. The ANCHOR registry has been in existence since 2012, and it takes some time to gather a larger volume of patients and show durable results at 4 years, backed by statistical validity.
Our endpoints demonstrate that we did not have to go back and revise endografts at the proximal area, which was a primary point of concern. The endografts were durable, and they did not have type 1 endoleaks or proximal type 1 endoleaks. The endografts usually required a revision distally, but such a revision is more often related to the progression of the disease.
Tell us more about the results of the primary and revision cohorts.
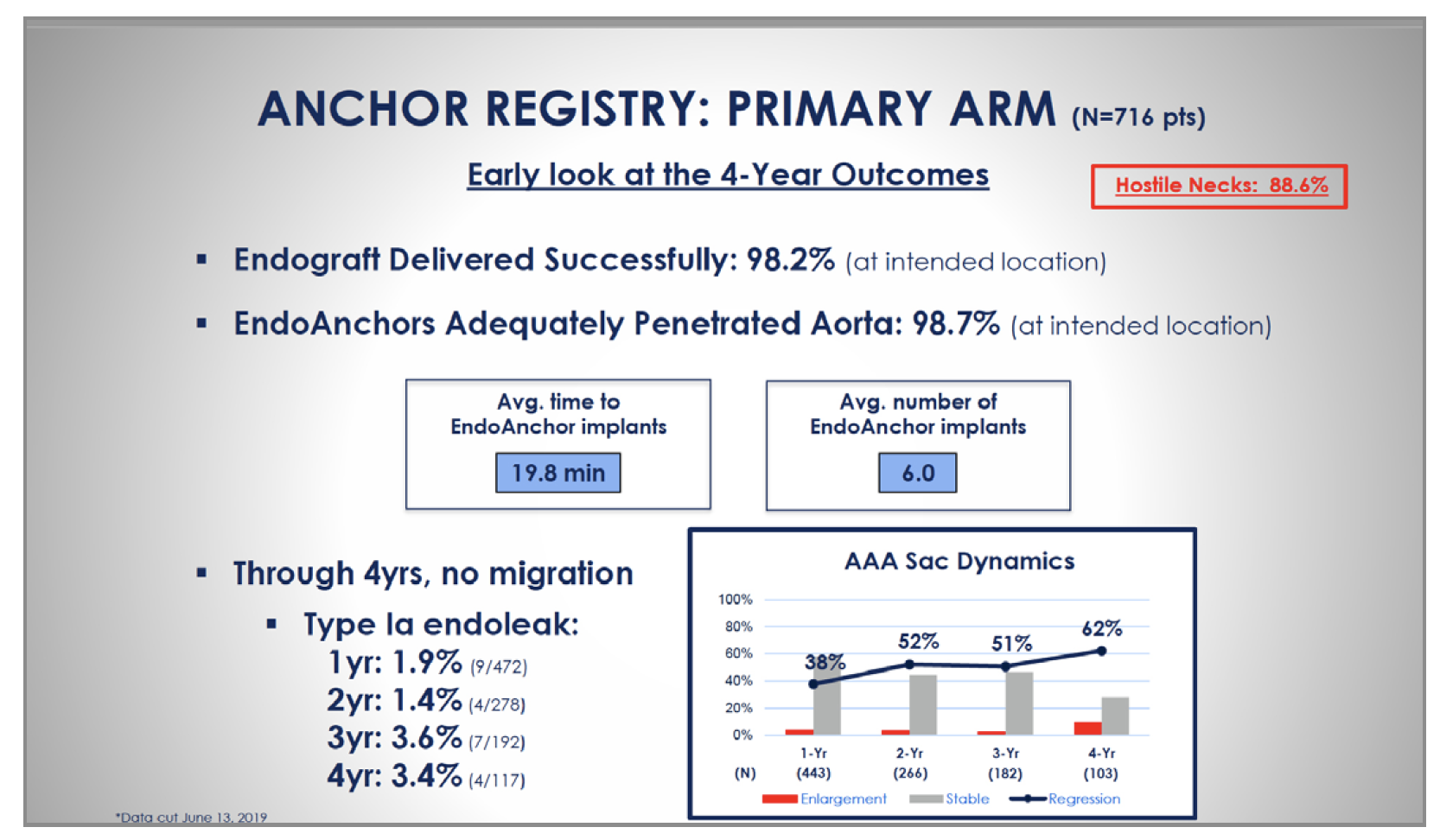
The primary arm (Figure 1) shows that there is greater success when the physician recognizes the potential for a bad aortic proximal fixation and uses the anchors in the first repair of the aneurysm. There is a better success rate when the anchors are used in the primary repair arm versus the revision arm. At 4 years, freedom from type 1A endoleaks was 97% in the primary repair arm and freedom from rupture (shown with Kaplan-Meier plots) was 98%. Freedom from secondary revisions was 87%, but most of those revisions were related to distal revisions rather than type 1A endoleaks. It is important to remember that the revision arm was already pre-selected for patients who have failed the initial repair. This means that there is some reason that the grafts failed, which sets the patients up for another failure later. The overall implication is that there is better long-term success if the aneurysm is fixed optimally the first time.
Many of the patients had met the Society for Vascular Medicine definition of hostile aortic necks. What process was used to define and classify hostile necks?
Determining what constitutes a hostile neck is important, and a distinct advantage of the ANCHOR registry is that a separate core laboratory objectively examined each CT scan to help define a bad neck. The neck length and conicity are mainly what contributed to the hostile neck anatomy, which comprised 88% of patients in the primary cohort (Figure 2).
Which patients are the best candidates for EndoAnchors?
Patients with large diameter necks or cases in which there is a concern that the necks are beginning to dilate before treatment begins are the best candidates for EndoAnchors. If there is a short neck and a concern about the fixation zone, the EnchoAnchor can add to the security of the fixation zone. If there is a type 1 endoleak after the implantation at the primary procedure, the endoleak should be fixed right away, because that is where you will have some of the highest success rates.
Practicing physicians who are new to this therapy should consider using the EndoAnchor on larger diameter necks because our data show that those necks are more likely to have late failure. By gaining familiarity with the technology, physicians will have improved skillsets when in tough anastomotic situations.
What are the future plans for the ANCHOR Registry?
The ANCHOR Registry closed to enrollment after it reached 1,000 patients. We are now at the point of processing the outcomes and determining whether there are additional data that we need to gather. If we can follow as many patients as possible to the five-year mark, we will have a better sense about durability. We would also like to know that the EndoAnchor improves long-term survival, so we need to continue following patients with that goal in mind.
What are the main takeaways from your presentation for practicing clinicians?
There is clearly a clinical benefit to using EndoAnchors, particularly when the goal is long-term, durable results. The biggest concern is figuring out how to justify the cost. The benefits of the EndoAnchor are great, but cost reasons prevent us from adding the EndoAnchor as a supplemental adjunct to every case. One good strategy is to determine which patients are higher risk and use the anchors in the primary repair. This approach can prevent a secondary revision down the road and recover the cost of the anchors.
Disclosures: The registry was funded by Medtronic. Dr. Jordan reports he received institutional research grants from Cook Medical, Endologix, Medtronic, Terumo and W.L. Gore and Associates and consultant fees paid to his institution from Medtronic and W.L. Gore and Associates.
