


How to Prepare For, and Treat, Potential Complications in the Outpatient Endovascular Center
Working in an outpatient endovascular center, also known as an office-based lab (OBL), prompts certain considerations that do not exist in a hospital setting. The most important consideration is that there is no immediate availability of an operating room, anesthesiology team, blood bank, code team, or any other subspecialists that may be needed in an emergency such as a procedural complication or patient decompensation. It is therefore incumbent upon those of us operating in an outpatient center to take additional precautions to both try to avoid complications and to promptly treat complications when they do occur. Failure to rapidly resolve complications may mean an unsatisfactory patient outcome or even death. If the problem cannot be managed on site, then an inter-institutional transfer may become necessary. A transfer requires that the patient is stable enough for transport and that a relationship exists between the outpatient center and a hospital and/or accepting physician(s) with the necessary skills to treat the problem. If the physician working in the OBL also maintains privileges at the receiving hospital, the transfer process may be smoother. In other cases, the local hospital may not have the expertise to resolve the problem and may only be able to stabilize the patient, with subsequent transfer to a more remote institution for definitive treatment. This latter situation describes my OBL, and I have consequently worked to put procedures and practices into place to try to prevent or mitigate patient complications.
Safety of OBLs
There are a number of well-described benefits to patients treated in an OBL compared to hospital-based procedures.1-3 When I conceived my OBL, which is called Flint Hills Heart, Vascular and Vein Clinic, in Manhattan, Kansas, one of my chief goals was to provide advanced vascular services to a population that had to otherwise travel many miles, hours in many cases, to a hospital in order to obtain these services. We specialize in treating patients with critical limb ischemia (CLI), and these patients comprise about 60% of our case load in the endovascular suite. Patients with CLI tend to be sicker and less able to tolerate procedural complications. With the nearest hospital with the capability to treat these patients at least an hour away, it is of paramount importance to try to prevent, and treat, complications on site if necessary. Patient safety must be the overriding consideration. It is better to have an unsuccessful but uncomplicated procedure than to persist beyond the point of likely success and risk a complication. The success of the clinic is predicated on both the success of the procedures and the lack of complications. Some patients are already concerned about having what they perceive to be a complex procedure in an outpatient center. A solid reputation can go a long way toward allaying these trepidations, and that reputation must be grounded in patient safety.
Requirements
Physicians operating in an outpatient clinic must possess the skillset and sufficient experience required to safely perform procedures. Aptitude, case volume, and complexity of procedures all play significant roles, so it is not possible to define “experience” numerically. The key point is that physicians must work within their comfort level, which may mean deferring some complex cases to the hospital or to a more experienced colleague in the outpatient center. There are published “appropriate use criteria” that may be helpful in guiding decisions,4 but I personally consider these criteria to be too conservative. Nonetheless, the published criteria can provide a baseline so that if one “colors outside the lines,” the heightened importance of safety can be appreciated.
The requirements to operate an OBL are extensive, so this article will focus on certain considerations for making the procedures safe and successful. When we opened our center six years ago, the biggest concern was what would happen if a patient had a hemodynamic collapse during a procedure. To address this issue, we required that everyone working in a patient care position at the clinic be advanced cardiovascular life support (ACLS) certified. We periodically run drills to prepare for procedural complications that could lead to patient compromise. These drills ensure that the two nurses and the technologist in the room with the operator each know their roles. All the intravenous agents necessary to treat such emergencies are available, as is the ability to intubate if necessary. If the operator says to start dopamine, start compressions, administer oxygen by mask, or any other of a number of possibilities, each person knows ahead of time which staff member is responsible for that action without the need for making assignments in the moment. This approach saves critical time. The emergency must be resolved quickly, because there will not be time for transfer to a hospital. It takes very little time to run the drills with the staff on a regular basis and ensure that all the necessary drugs are in the crash cart.
The most common causes of complications are related to the access site. To that end, it is imperative to have quality duplex ultrasound studies prior to the intervention. Many patients will be referred for intervention with unsatisfactory studies, so we need to repeat the study, if necessary, to determine the status of all the vessels that are potentially needed for accessing, traversing, and treating the patient. In patients with CLI, the status of all the tibial vessels must be known. I have found that tibial artery duplex scanning is the most deficient of outside examinations and one of the more common reasons to repeat the study.
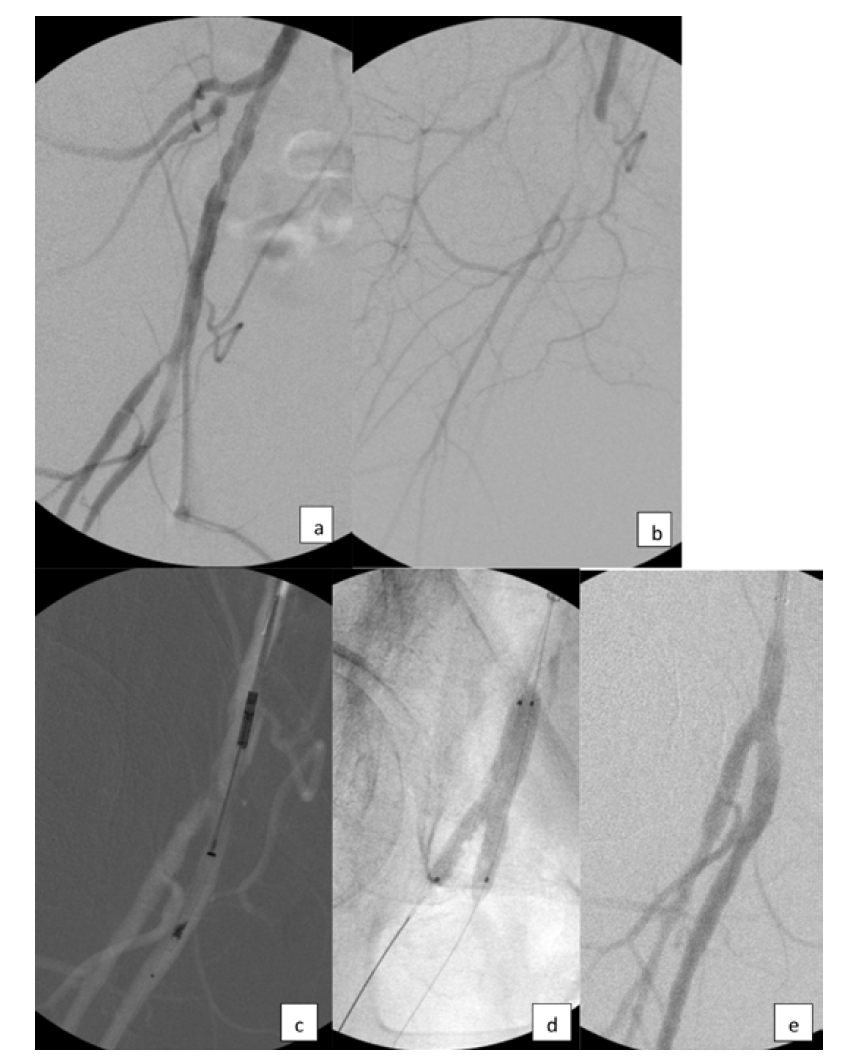
Like many operators these days, we use ultrasound-guided access in almost every case. Starting with a micropuncture needle and sheath is safest, if not necessary, in all cases. Our first angiogram is usually of the access site in order to determine that we are in the optimal location and, in the case of femoral artery access, whether a closure device may be used at the end of the case. We use closure devices in 97% of our femoral artery access cases,5 which results in faster time to ambulation. Additionally, some patients travel great distances to home after the procedure,6 and using a closure device helps to prevent a late bleed at an inopportune time. I predominantly use a suture-based device, but also have collagen-plug type devices when the former is not applicable, as in heavily calcified access vessels. It is important to be familiar with the complications that can occur if a closure device is not properly deployed, or if the device malfunctions, and know how to resolve the situation. Becoming well acquainted with a couple of closure devices rather than many devices may help to build operator skills and minimize the risk of unsuccessful deployment. In my own experience, I have rarely caused acute access site closure from improper closure device deployment, which usually occurs when a closure device is used in a diseased vessel (Figure 1). All operators must know how to respond to this scenario. Follow activated clotting time (ACT) throughout the case, usually after the initial heparin bolus, and at least every 30 minutes thereafter, to minimize the risk of thrombus generation, particularly when there is diminished flow and in tibial interventions. The variability in the response to standard weight-based administration can be striking between individuals. The presence of thrombus will usually require additional heparin as well. Only the ACT will determine the proper dosing of heparin during the case. The range should be 200 – 300 seconds, depending upon circumstances.
Managing Complications
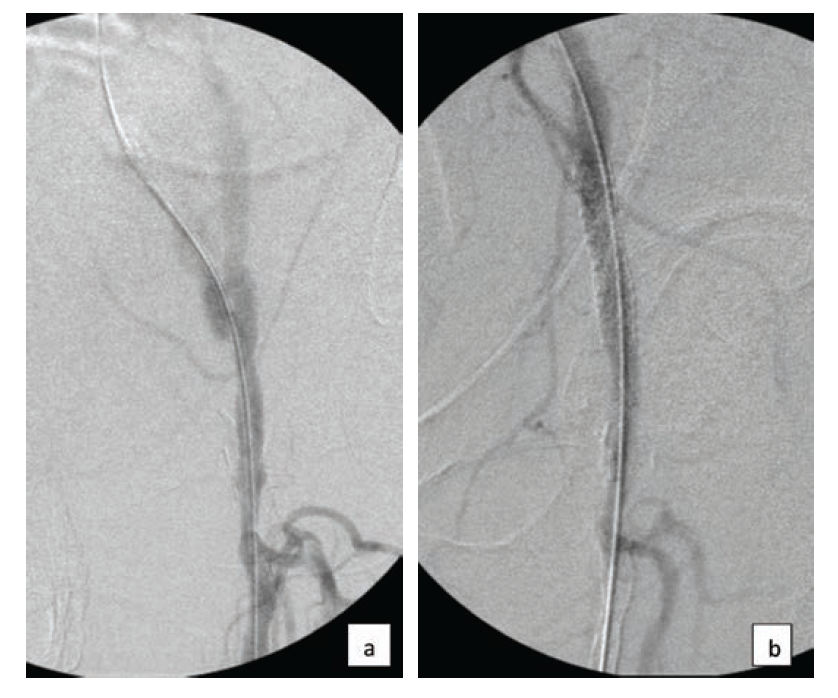
While access sites constitute the most common type of procedural complication, vessel rupture is the most feared complication and can occur at any vascular level. Rupture of an iliac artery can result in precipitous and catastrophic hemodynamic compromise if not immediately treated (Figure 2). I keep a number of covered stents on the shelf to mitigate this complication, should it occur. These stents include both balloon-expandable and self-expanding varieties of varying sizes. Many of these stents will outdate on the shelf, and I will replace them. I also keep embolization coils in inventory, as these coils can be helpful for small vessel perforation or vessel “leaks.” Stocking devices is a form of insurance that will hopefully not need to be used.
The rare occasions of iliac rupture are typically cases of chronic total occlusion (CTO) recanalization with subintimal wire passage. Therefore, in cases of iliac artery CTO recanalization, upsize the sheath prior to balloon dilatation so that precious time is not wasted performing this maneuver if a rupture occurs. Intravascular ultrasound can also be used prior to aggressive balloon dilatation or stenting. In all cases, it is important to recognize the potential complications for each case and to be appropriately prepared. For some of us, this knowledge unfortunately comes from personal experience, but much can be gleaned from presentations at the “Worst Complications” session at most conferences. Everyone can benefit from attending these types of sessions.
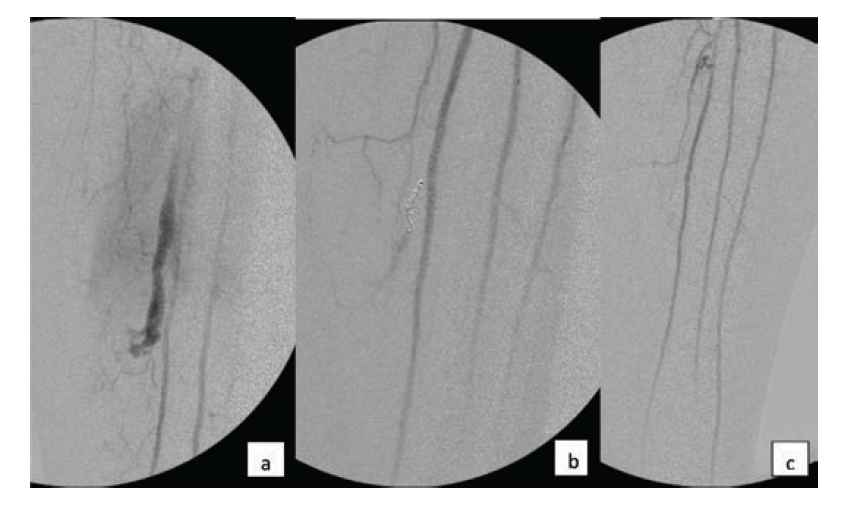
Atherectomy is commonly used in lower extremity endovascular procedures, both in the femoropopliteal and tibial vascular territories. There are many devices available with different mechanisms of action, but they all have the goal of plaque removal in common, which comes with an increased risk of vessel perforation, particularly when treating a CTO. Contained perforation can often be successfully treated with reversal of anticoagulation and prolonged balloon inflation. Development of an arteriovenous fistula is generally well tolerated. In the femoropopliteal segment, a covered stent may be utilized if there is a free perforation. In the tibial arteries, covered stent placement is not an available option. A free perforation in a tibial artery can quickly result in compartment syndrome if it is not expeditiously treated. The complication demonstrated in Figure 3 did not resolve despite reversal of anticoagulation and prolonged balloon inflation. It was successfully resolved with stent-supported coil embolization. Drug-eluting stent deployment was able to maintain vessel patency, while the coils provided good resolution of the extravasation.
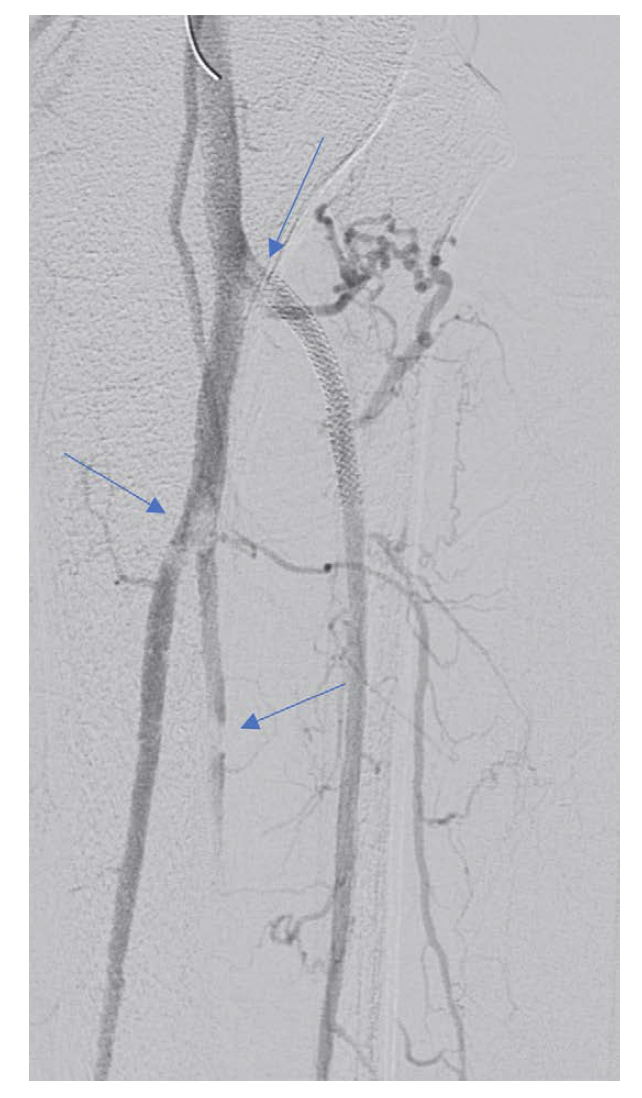
The risk of distal embolization is also increased with atherectomy compared to balloon angioplasty and stenting, where embolization is clinically less common. There are several filters available to protect against distal embolization, and it is important to understand these filters, be comfortable with their use, and have filters on hand that are compatible with the devices used. Treating distal embolization will add a great deal of time, stress, and risk to any procedure (Figure 4). It is also important to be familiar with the causes and treatment of slow-flow or no-flow phenomena. Was the phenomenon caused by proximal dissection or microembolization? Microembolization is more common with the use of rotational or orbital atherectomy. Proximal dissection is usually corrected with stent placement while microembolization is often treated with vasodilators, particularly those that act on the arterioles, such as adenosine.
Another important action is to always check pedal pulses immediately following the procedure, while the patient is still on the table, both in the treated limb and the access limb. Correction of a problem is much more efficient, and more likely to be successful, if done while the patient is still draped and on the table. However, the patient may have good pulses at the termination of the procedure only to lose those pulses in the recovery period. In our clinic, outpatient treatment offers the advantage of frequent visits to the bedside of the patient, as the operator is usually on site and not at a remote office that is far from the hospital where the procedure was performed. Additionally, the nurses in our clinic are all well trained in how to assess various pulses. In many cases, a simple bedside duplex scan can be performed to identify the problem, and the patient can be rapidly returned to the angiographic suite if needed. On multiple occasions, we have sent the patient home the same day after additional intervention.
Following the procedure, we want to avoid a phone call the next day from the patient indicating that the patient has a cold, painful foot. Our clinic is extremely attentive about proactively managing this aspect of patient recovery, and yet, even with our efforts, a cold and painful foot will still occur, though rarely. We recommend having a nurse call the patient the next day to assess recovery. Despite instructions alerting the patient and family members to the possible development of significant discomfort and edema in the limb post procedure, there will often be concern by the patient if discomfort and edema develop. A phone call can readily allay these fears and potentially avert an emergency department visit. Simply asking the patient if the foot is warm or cool can often quickly settle any question about the status of blood flow to the limb.
Conclusion
The best way to obtain successful outcomes in an OBL is to know the types of complications that may occur as a result of a given procedure, and to avoid those complications through meticulous planning. If complications do occur, prompt treatment is paramount. Successful planning to avoid complications, and treatment when complications do occur, requires an extensive knowledge base arising from the experience of performing many cases. Thus, operators must only perform cases in the outpatient setting with a complexity that is commensurate with their experience. Performing procedures safely is as important as performing them successfully.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest and report no conflicts of interest regarding the content therein.
Manuscript submitted October 20, 2019; manuscript accepted October 24, 2019.
Address for correspondence: Address for correspondence: Raymond Dattilo, MD, FACC, Flint Hills Heart, Vascular and Vein Clinic; Manhattan, Kansas, United States. Email: icardmd@aol.com
REFERENCES
1. Jain K. Why outpatient centers and office-based labs (OBLs) are the best place to do which endovascular procedures: best for patients and best for operators: when can atherectomies be performed safely there; when not. Presented at: VEITHsymposium 2019. November 20, 2019. New York, NY.
2. Mukherjee D. Real world results of lower extremity atherectomy (mostly in outpatient centers) from Medicare billing data is much worse than favorable registry data: where lies the truth. Presented at: VEITHsymposium 2019. November 20, 2019. New York, NY.
3. Lin PH, Yang KH, Kolllmeyer KR, et al. Treatment outcomes and lessons learned from 5134 cases of outpatient office-based endovascular procedures in a vascular surgical practice. Vascular. 2017;25(2):115-122.
4. Bailey SR, Beckman JA, Dao TD, et al. ACC/AHA/SCAI/SIR/SVM 2018 appropriate use criteria for peripheral artery intervention: a report of the american college of cardiology appropriate use criteria task force, american heart association, society for cardiovascular angiography and interventions, society of interventional radiology, and society for vascular medicine. J Am Coll Cardiol. 2019;73(2):214-237.
5. Dattilo R, Dattilo A, Colby S. Outcomes of patients treated for critical limb ischemia in an outpatient endovascular center. Vascular Disease Management. 2018;15(6):E49-E52.
6. Dattilo R. OBL spotlight: Flint Hills Heart, Vascular and Vein Clinic. Cath Lab Digest 2019 Aug;(27)8:40-41.
