

Managing Thrombosis and Lower Limb Ischemia Using Directional Atherectomy and Balloon Angioplasty
Abstract
A 71-year-old male underwent bilateral renal artery stenting via the right femoral artery and received an Angio-Seal vascular closure device (St. Jude Medical) for access site hemostasis upon completion of the case. Two weeks later, he presented with critical limb ischemia and thrombosis at the site of Angio-Seal deployment. Directional atherectomy and adjunctive balloon angioplasty were used to eliminate the remnant Angio-Seal anchor and restore patency to the common femoral artery.
VASCULAR DISEASE MANAGEMENT 2012:9(10):E172-E174
Case Report
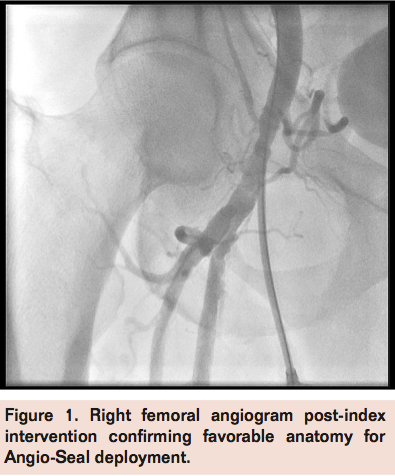 A 71-year-old male with history of coronary artery disease and 2 previous coronary artery bypass surgeries, hypertension, dyslipidemia, diabetes mellitus, and chronic kidney disease underwent successful bilateral renal artery stenting via the right femoral approach through an 8 Fr sheath in the setting of refractory hypertension and renal insufficiency. Following the procedure, an 8 Fr Angio-Seal (St. Jude Medical) vascular closure device was deployed without complications, after limited femoral angiogram confirmed favorable anatomy (Figure 1). He was discharged on dual antiplatelet therapy with aspirin 325 mg and clopidogrel 75 mg daily. One week following the procedure, the patient stated that he began having significant right lower extremity pain with minimal exertion, followed by intermittent right foot numbness despite compliance with all medications. However, the patient delayed any further evaluation until 2 weeks post-procedure, when the patient presented with right lower limb ischemia demonstrated by pallor and rest pain. Right groin ultrasound was suggestive of occlusive disease within the right common femoral artery. Ankle-brachial index was 0.3 on the right posterior tibial and 0.35 on the right dorsalis pedis. Due to the patient’s symptoms and abnormal non-invasive testing, right lower extremity angiography was offered.
A 71-year-old male with history of coronary artery disease and 2 previous coronary artery bypass surgeries, hypertension, dyslipidemia, diabetes mellitus, and chronic kidney disease underwent successful bilateral renal artery stenting via the right femoral approach through an 8 Fr sheath in the setting of refractory hypertension and renal insufficiency. Following the procedure, an 8 Fr Angio-Seal (St. Jude Medical) vascular closure device was deployed without complications, after limited femoral angiogram confirmed favorable anatomy (Figure 1). He was discharged on dual antiplatelet therapy with aspirin 325 mg and clopidogrel 75 mg daily. One week following the procedure, the patient stated that he began having significant right lower extremity pain with minimal exertion, followed by intermittent right foot numbness despite compliance with all medications. However, the patient delayed any further evaluation until 2 weeks post-procedure, when the patient presented with right lower limb ischemia demonstrated by pallor and rest pain. Right groin ultrasound was suggestive of occlusive disease within the right common femoral artery. Ankle-brachial index was 0.3 on the right posterior tibial and 0.35 on the right dorsalis pedis. Due to the patient’s symptoms and abnormal non-invasive testing, right lower extremity angiography was offered.
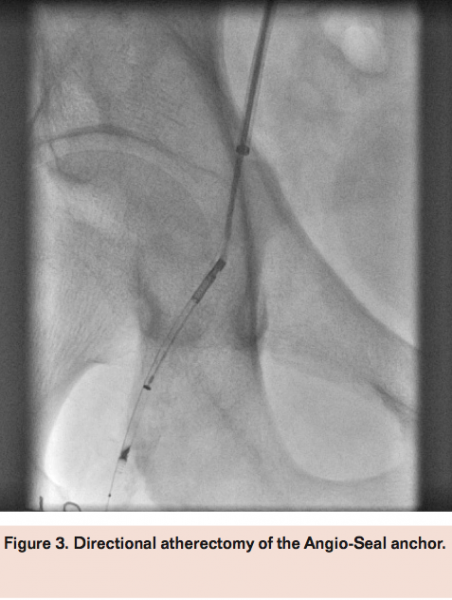
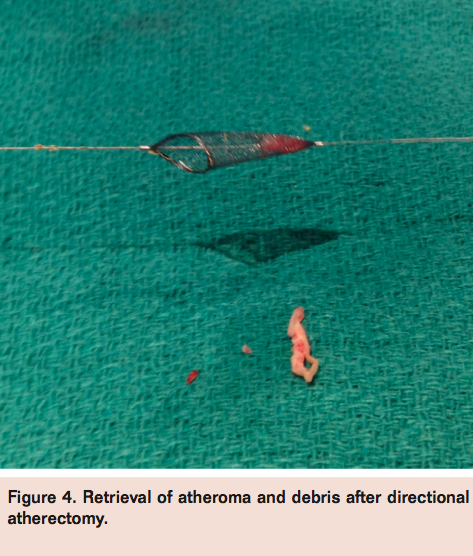
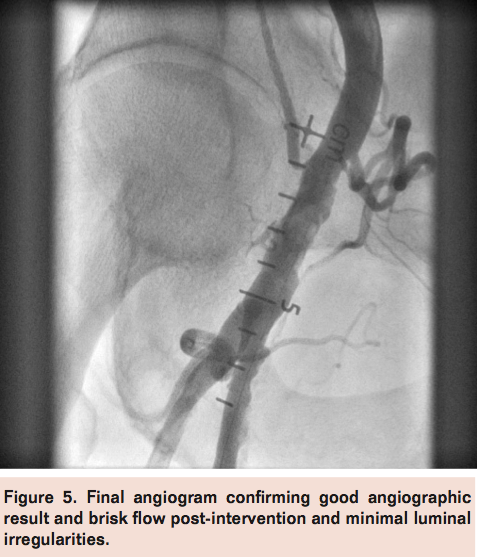
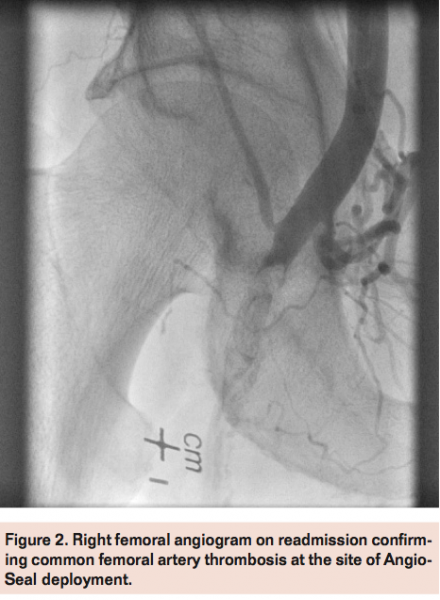 Access was obtained in the left femoral artery with a 7 Fr sheath. Angiography of the right external iliac artery with runoff demonstrated a hazy thrombotic 20 mm subtotal occlusion of the right common femoral artery at the site of previous Angio-Seal device deployment with filling of the distal common femoral artery via microchannels (Figure 2). A Grand Slam wire (Abbott Vascular) was advanced across the lesion into the distal popliteal artery and a Spider 6.0 mm distal embolic protection device (Covidien) was deployed in the popliteal artery. Directional atherectomy with a TurboHawk LSM device (Covidien) was performed (Figure 3) with multiple cuts to eliminate the residual Angio-Seal anchor and collecting some atheroma (Figure 4). The filter was retrieved successfully, which also revealed a moderate amount of macro debris (Figure 4). Final angiogram after adjunctive balloon angioplasty demonstrated good angiographic result with brisk flow through the common femoral artery and minimal residual luminal irregularities (Figure 5).
Access was obtained in the left femoral artery with a 7 Fr sheath. Angiography of the right external iliac artery with runoff demonstrated a hazy thrombotic 20 mm subtotal occlusion of the right common femoral artery at the site of previous Angio-Seal device deployment with filling of the distal common femoral artery via microchannels (Figure 2). A Grand Slam wire (Abbott Vascular) was advanced across the lesion into the distal popliteal artery and a Spider 6.0 mm distal embolic protection device (Covidien) was deployed in the popliteal artery. Directional atherectomy with a TurboHawk LSM device (Covidien) was performed (Figure 3) with multiple cuts to eliminate the residual Angio-Seal anchor and collecting some atheroma (Figure 4). The filter was retrieved successfully, which also revealed a moderate amount of macro debris (Figure 4). Final angiogram after adjunctive balloon angioplasty demonstrated good angiographic result with brisk flow through the common femoral artery and minimal residual luminal irregularities (Figure 5).
 The patient was discharged home the following day without any complications. At follow-up in clinic 1 month later, there were no recurrent symptoms and palpable pedal pulses.
The patient was discharged home the following day without any complications. At follow-up in clinic 1 month later, there were no recurrent symptoms and palpable pedal pulses.
Discussion
Approximately 49% of patients who undergo a percutaneous coronary intervention receive a vascular closure device.1 Several meta-analyses have found that vascular closure devices had a shorter time to hemostasis than manual compression corresponding to shorter duration of bed rest and shorter hospital stay.2 However, this convenience comes at a cost of possible increased risk of groin hematoma and bleeding, pseudoaneurysms, and device infection,2 although these findings are not universal across all studies.3
The Angio-Seal closure device consists of 3 bioresorbable components that include an anchor, a plug, and positioning suture.4 The 3 components are contained within a delivery system with a tamper tube. Hemostasis is maintained by tension between the anchor, which is positioned flat against the arterial wall, and the plug, which is exterior to the artery via the suture line. Pulling the suture line causes the anchor and plug to approximate on the arterial wall. All the components are fully absorbed by the body in 60 to 90 days.4
 The Angio-Seal investigators found a 9% complication rate, including need for vascular repair, pseudoaneurysm, blood transfusion, hematoma, and late bleeding compared with 6% for manual pressure.4 Other reported complications include infection, retroperitoneal bleed, and arteriovenous fistulas.4,5 There are rare case reports of femoral thrombosis of the Angio-Seal device not attributable to known vascular disease.6,7 The majority of these cases were treated surgically with endarterectomy,7 although recently other endovascular treatment strategies including balloon angioplasty and laser atherectomy have been described.6
The Angio-Seal investigators found a 9% complication rate, including need for vascular repair, pseudoaneurysm, blood transfusion, hematoma, and late bleeding compared with 6% for manual pressure.4 Other reported complications include infection, retroperitoneal bleed, and arteriovenous fistulas.4,5 There are rare case reports of femoral thrombosis of the Angio-Seal device not attributable to known vascular disease.6,7 The majority of these cases were treated surgically with endarterectomy,7 although recently other endovascular treatment strategies including balloon angioplasty and laser atherectomy have been described.6
 The etiology of Angio-Seal thrombosis is unclear. While polylactic and polyglycolic acids, which are components of the anchor, have been shown to cause inflammation in animal models,8 other studies demonstrated no evidence of thrombosis.9 Alternative extravascular closure devices without intravascular anchors are currently available to avoid this risk of thrombosis.10 This report is the first documented use of directional atherectomy with distal protection to remove the thrombogenic material in the setting of device-related thrombosis.
The etiology of Angio-Seal thrombosis is unclear. While polylactic and polyglycolic acids, which are components of the anchor, have been shown to cause inflammation in animal models,8 other studies demonstrated no evidence of thrombosis.9 Alternative extravascular closure devices without intravascular anchors are currently available to avoid this risk of thrombosis.10 This report is the first documented use of directional atherectomy with distal protection to remove the thrombogenic material in the setting of device-related thrombosis.
References
- Subherwal S, Peterson ED, Dai D, et al. Temporal trends in and factors associated with bleeding complications among patients undergoing percutaneous coronary intervention: a report from the National Cardiovascular Data CathPCI Registry. J Am Coll Cardiol. 2012;59(21):1861-1869.
- Biancari F, D’Andrea V, Di Marco C, Savino G, Tiozzo V, Catania A. Meta-anaylsis of randomized trials on the efficacy of vascular closure devices after diagnostic angiography and angioplasty. Am Heart J. 2010;159(4):518-531.
- Arora N, Matheny ME, Sepke C, Resnic FS. A propensity analysis of the risk of vascular complications after cardiac catheterization procedures with the use of vascular closure devices. Am Heart J. 2007;153(4):606-611.
- Henry M, Amor M, Allaoui M, Tricoche O. A new access site management tool: the Angio-Seal hemostatic puncture closure device. J Endovasc Surg. 1995;2(3):289-296.
- Nikolsky E, Mehran R, Halkin A, et al. Vascular complications associated with arteriotomy closure devices in patients undergoing percutaneous coronary procedures: a meta-analysis. J Am Coll Cardiol. 2004;44(6):1200-1209.
- Trayer T, George JC. Successful endovascular treatment of common femoral artery thrombosis occurring 2 months after catheterization and Angio-Seal closure. Vascular Disease Management. 2012;9(2):E27-E29.
- Cikirikcioglu M, Cherian S, Keil V, el al. Surgical treatment of complications associated with the Angio-Seal vascular closure device. Ann Vasc Surg. 2011;25(4):557.e1-e4.
- van der Giessen WJ, Lincoff AM, Schwartz RS, et al. Marked inflammatory sequelae to implantation of biodegradable and nonbiodegradable polymers in porcine coronary arteries. Circulation. 1996;94(7):1690-1697.
- Iwai S, Sawa Y, Ichikawa H, et al. Biodegradable polymer with collagen microsponge serves as a new bioengineered cardiovascular prosthesis. J Thorac Cardiovasc Surg. 2004;128(3):472-479.
- Scheinert D, Sievert H, Turco MA, et al. The safety and efficacy of an extravascular, water-soluble sealant for vascular closure: initial clinical results for Mynx. Catheter Cardiovasc Interv. 2007;70(5):627-633.
__________________________________________________________________
From the Deborah Heart and Lung Center, Browns Mills, New Jersey.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. Dr. George reports consultancy for Covidien. Dr. Groben reports no conflicts regarding the content herein.
Manuscript submitted August 15, 2012, provisional acceptance given August 27, 2012, final version accepted September 11, 2012.
Address for correspondence: Jon C. George, MD, Director of Clinical Research, Division of Cardiovascular Medicine, Deborah Heart and Lung Center, 200 Trenton Road, Browns Mills, NJ, 08015, USA. Email: georgej@deborah.org
