

New Stroke VTE Safety Recommendations: Four Key Steps to Better Health Outcomes
New Stroke VTE Safety Recommendations provide 4 key steps to help prevent deep vein thrombosis (DVT) and pulmonary embolism (PE) in stroke patients. Deep vein thrombosis (DVT) and pulmonary embolism (PE) are common peristroke complications. DVTs are found in 40% to 80% of stroke patients, and PEs are present in 10% to 15% of all stroke patients, with PEs accounting for 13% to 25% of early deaths after a stroke.1 Below we discuss these 4 steps from the new Stroke VTE Safety Recommendations and encourage all clinicians to assess and treat stroke patients for venous thromboembolism (VTE).
Step 1: Assess Patients With Stroke or Rule Out Stroke Diagnosis
Assess all admitted patients with a stroke or rule out stroke diagnosis for risk of VTE. As Leizorovicz and Mismetti stated, “There is a need for systematic assessment of risk in patients hospitalized for acute medical conditions. Quantifying a patient’s risk permits selection of those for whom the benefits of prophylaxis exceed its dangers. This assessment should be based on predisposing risk factors, inherited or acquired, as well as the transient risk associated with hospitalization.”2 Doing so determines who may be at risk of VTE and who may not be, allowing for the application of appropriate pharmacological and mechanical prophylaxis.
Step 2: Prescribe Recommended Prophylaxis
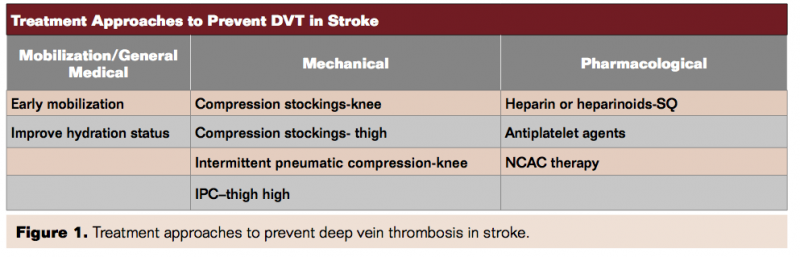
Provide the recommended prophylaxis regimen, which includes the use of mechanical prophylaxis and anticoagulant therapy, unless contraindicated. The different approaches to preventing DVT in stroke patients are summarized in Figure 1.
Much has already been written about the use of anticoagulants. Current AHA stroke guidelines recommend the following:
- The use of subcutaneous anticoagulation for DVT prevention is a class I, level A recommendation.
- The use of aspirin is a class IIa, level A recommendation.
- The use of external compression devices is a class IIa, level B recommendation (written before CLOTS 3 study, discussed below).
Although not a specific guideline recommendation, the PREVAIL study showed that enoxaparin 40 mg subcutaneously 4 times a day was more effective than unfractionated heparin 5,000 U subcutaneously 2 times a day.3
Given results of the recent CLOTS 3 study,4 which involved nearly 3,000 stroke patients at over 100 hospitals across the United Kingdom, particular emphasis needs to be placed on the use of thigh-length intermittent pneumatic compression (IPC). The CLOTS 3 study was a multicenter parallel-group randomized trial. Patients were enrolled from day 0 to day 3 of admission and allocated via a central randomization system (ratio 1:1) to receive either IPC or no IPC. The CLOTS 3 study showed a 29% reduction in life-threatening DVT and a 14% reduction in overall mortality for patients receiving thigh-length IPC therapy.
Intermittent pneumatic compression can be used in all types of stroke patients, particularly in cases where anticoagulant use is contraindicated. As stated by Jauch et al, “The use of intermittent external compression devices is reasonable for treatment of patients who cannot receive anticoagulants” (Class IIa; Level of Evidence B; revised from the previous guideline).5
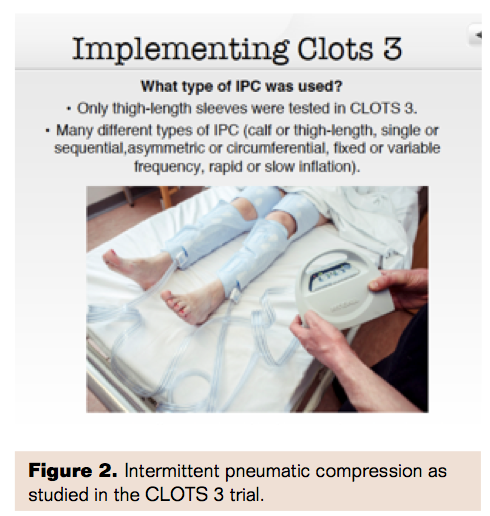 Although compression stockings are commonly used on stroke patients, overall there has been no evidenced benefit from their use.1 Intermittent pneumatic compression applies pressure on the tissues in the limb, thereby forcing fluids, such as blood and lymph, out of the pressurized area, followed by a pressure reduction, allowing increased blood flow back into the limb. Moreover, although there are many different types of IPC (calf or thigh length, single or sequential, asymmetric or circumferential, fixed or variable frequency, rapid or slow inflation), only thigh-length sleeves were tested in CLOTS 3 (Figure 2).
Although compression stockings are commonly used on stroke patients, overall there has been no evidenced benefit from their use.1 Intermittent pneumatic compression applies pressure on the tissues in the limb, thereby forcing fluids, such as blood and lymph, out of the pressurized area, followed by a pressure reduction, allowing increased blood flow back into the limb. Moreover, although there are many different types of IPC (calf or thigh length, single or sequential, asymmetric or circumferential, fixed or variable frequency, rapid or slow inflation), only thigh-length sleeves were tested in CLOTS 3 (Figure 2).
Step 3: Reassess Patients for Venous Thromboembolism Risk
A risk factors reassessment should be conducted and documented as follows:
- Prior to any surgical or procedural intervention;
- With change in the patient’s condition;
- At minimum once every 24 hours.
- Step 4: Ensure Appropriate Discharge
Approximately 1 in every 4 of the nearly 800,000 strokes that occur each year is recurrent.6 Ensure that the patient is provided appropriate VTE instructions and information upon hospital discharge or transition to rehabilitation.
Four Key Steps to Better Health Outcomes
Assessing and treating stroke should be done in as short a period of time as possible. Successful health outcomes in stroke patients often depend on having as short a door to treatment time as possible. Delays in evaluation and initiation of therapy should be avoided, because the opportunity for improvement is greater with earlier treatment. This means not only having a collaborative team effort, but also looking at anything that might shorten door-to-treatment times, including designated parking for stroke patients. Unfortunately, the provision of needed prophylaxis has been suboptimal.7-9
The new Stroke VTE Safety Recommendations, developed by a group of leading neurologica health and patient safety experts brought together by the Physician-Patient Alliance for Health & Safety, provide a concise and standardized application of the latest research and best practices. We encourage clinicians to avail themselves of this free resource.
Editor’s note: Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no disclosures related to the content herein.
Address for correspondence: Michael Wong can be reached by email at mwong@ppahs.org.
References
- Kappelle LJ. Preventing DVT after stroke. Curr Treat Options Neurol. 2011; 3(6):629-635.
- Leizorovicz A, Mismetti P. Preventing venous thromboembolism in medical patients. Circulation. 2004;110(24 Suppl 1):IV13-IV19.
- Holmes DR Jr, Kar S, Price MJ et al. Prospective randomized evaluation of the Watchman Left Atrial Appendage Closure device in patients with atrial fibrillation versus long-term warfarin therapy: the PREVAIL trial. J Am Coll Cardiol. 2014;64(1):1-12.
- CLOTS (Clots in Legs Or sTockings after Stroke) Trials Collaboration, Dennis M, Sandercock P, et al. Effectiveness of intermittent pneumatic compression in reduction of risk of deep vein thrombosis in patients who have had a stroke (CLOTS 3): a multicentre randomised controlled trial. Lancet. 2013;382(9891):516-524.
- Jauch EC, Saver JL, Adams HP Jr, et al. Guidelines for the early management of patients with acute ischemic stroke. Stroke. 2013;44(3):870-947.
- Furie KL et al, “Guidelines for the Prevention of Stroke in Patients With Stroke or Transient Ischemic Attack” Stroke. 2011;42:227-276.
- Gaspar L, Stvrtina S, Ocadlik I, et al. Autopsy-proven pulmonary embolism: a major cause of death in hospitalized patients. Adv Orthop. 2010;2:8-14.
- Caprini JA, Tapson VF, Hyers TM, et al; for the NABOR Steering Committee. Treatment of venous thromboembolism: adherence to guidelines and impact of physician knowledge, attitudes, and beliefs. J Vasc Surg. 2005;42(4):726-733.
- Yu HT, Dylan ML, Lin J, Dubois RW. Hospitals’ compliance with prophylaxis guidelines for venous thromboembolism. Am J Health Syst Pharm. 2007;64(1):69-76.
