

Ocelot With Wildcat in a Complicated Superficial Femoral Artery Chronic Total Occlusion
Abstract
Of the population of patients with symptomatic peripheral vascular disease (PVD), 40% have lower-extremity peripheral arterial occlusive disease. Chronic total occlusions (CTOs) are a challenge to vascular specialists, particularly when the lesions are calcified, long, and associated with poor distal run-off. These challenges often contribute to failure of percutaneous revascularization, and they often require surgical interventions, which are risky in high-risk operable candidates. A host of new devices is available on the market aimed at increasing the ability of operators to successfully open the chronic occlusions percutaneously and reduce the need for surgical interventions in very high-risk patient populations. All devices have their advantages, disadvantages, and limitations. We present a case of long left SFA chronic occlusion in a very high-risk operable candidate that was successfully recanalized utilizing the Ocelot and Wildcat CTO crossing devices (Avinger).
VASCULAR DISEASE MANAGEMENT 2014;11(8):E166-E171
Key words: chronic total occlusion, peripheral vascular disease, percutaneous revascularization
___________________________
Lower-extremity peripheral arterial occlusive disease is present in 40% of patients presenting with symptomatic peripheral vascular disease (PVD). Chronic total occlusions (CTOs) continue to be most challenging, particularly when the lesions are calcified, long, and associated with poor distal run-off. These challenges often contribute to failure of percutaneous revascularization, and often require surgical interventions, which are risky in high-risk operable candidates.
The Ocelot is designed for crossing CTOs in the lower extremities while simultaneously using optical coherence tomography (OCT) to navigate the catheter inside the lumen of the arteries and avoid subintimal dissections and perforations. It utilizes near-infrared light to optimize intravascular visualization. It has a 110 cm shaft length, and it is compatible with 6 Fr sheaths but more easily used with 7 Fr sheaths over 0.014 wires. The distal tip is preshaped and malleable. It has spiral flutes and optical fiber to help progression through the CTO. The presence of the directional markers allows the operator to adjust the orientation of the catheter continuously and redirect it to keep the catheter intraluminal. The CTO crossing segment of the catheter has 2 speeds.
Case Presentation
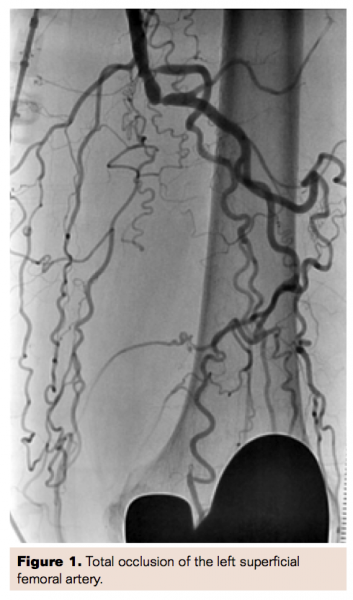 A 71-year-old male presented with multiple risk factors for cardiovascular disease and PVD, including a 60-pack-year history of smoking, hypertension, hyperlipidemia, diabetes mellitus, history of myocardial infarction, and ischemic cardiomyopathy (EF 35%). The patient presented with intermittent claudication for several years and rest pain over the last 6 months, Rutherford Class IV, with no critical limb ischemia and with ABI of 0.5 on the left leg. Angiogram of the lower extremity showed complete occlusion of the left superficial femoral artery (SFA) (Figure 1), with complete occlusion of the infrapopliteal vessels.
A 71-year-old male presented with multiple risk factors for cardiovascular disease and PVD, including a 60-pack-year history of smoking, hypertension, hyperlipidemia, diabetes mellitus, history of myocardial infarction, and ischemic cardiomyopathy (EF 35%). The patient presented with intermittent claudication for several years and rest pain over the last 6 months, Rutherford Class IV, with no critical limb ischemia and with ABI of 0.5 on the left leg. Angiogram of the lower extremity showed complete occlusion of the left superficial femoral artery (SFA) (Figure 1), with complete occlusion of the infrapopliteal vessels.
Treatment
Considering the length of the lesion, the degree of calcification, and the hyperacute angle of the aortic bifurcation, we opted for left femoral access antegrade approach for better support. A 6 Fr sheath was placed in the left common femoral artery in antegrade direction. An attempt to cross the CTO with a 0.035” angled Glidewire (Terumo) supported with a 5 Fr Glidecath (Terumo) was unsuccessful. Attempts with an Asahi 0.014˝ MiracleBros 3 g wire (Abbott Vascular) and a 0.014˝ Astato 20 g wire (Asahi), both supported by 0.014˝ Quick Cross catheter (Spectranetics), were also unsuccessful. We decided to attempt opening the CTO using the Ocelot device (Avinger). The 6 Fr sheath was upsized to 7 Fr. We advanced the Asahi 0.014˝ MiracleBros 3 g wire to the entry cap of the CTO. The Ocelot catheter was introduced over the wire to the entry cap of the CTO as well.
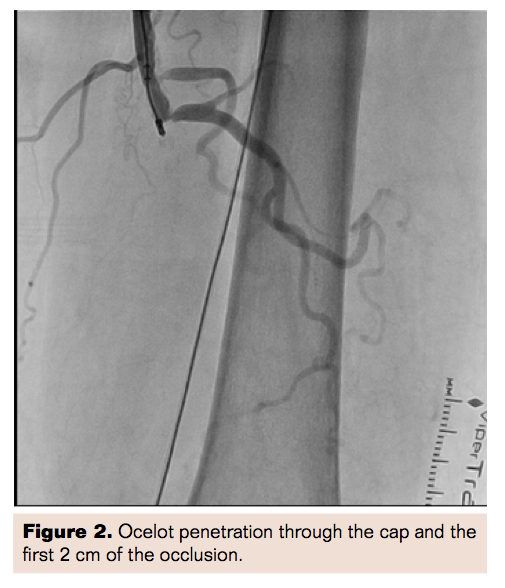 With the guidance of the OCT, the Ocelot catheter was successful in penetrating through the cap and the first centimeter of the total occlusion while remaining intraluminal (Figure 2). We were unable to make further progress despite increasing the speed of the Ocelot device and using a more supportive wire (Astato 20 g).
With the guidance of the OCT, the Ocelot catheter was successful in penetrating through the cap and the first centimeter of the total occlusion while remaining intraluminal (Figure 2). We were unable to make further progress despite increasing the speed of the Ocelot device and using a more supportive wire (Astato 20 g).
Because we were certain the device was intraluminal, we decided to remove the Ocelot and use the Wildcat, which offers a higher speed than is available in the Ocelot device. The Wildcat requires a 0.035˝ wire, which was introduced through wire exchanges using the Quick Cross catheter.
The Wildcat was easily advanced through the rest of the total occlusion along the SFA into the popliteal and proximal third the anterior tibial (AT) artery. The Wildcat catheter was removed, and the 0.035˝ wire was exchanged for a 0.014˝ Command guidewire (Abbott Vascular) using the Quick Cross catheter. The Command wire was easily advanced through the AT into the collateral to the posterior tibial (PT) artery in a retrograde fashion. The AT was ballooned using an Armada 2.5 mm x 200 mm x 150 cm balloon (Abbott Vascular). The balloon was removed and 0.014˝ Quick Cross catheter was used to traverse the plantar collaterals to the PT to attempt to open the occlusion in retrograde fashion, but the attempt was unsuccessful. Because the patient did not have critical limb ischemia, we focused on restoring flow through the AT and SFA.
The AT was further ballooned using a Powerflex 3.0 mm x 22 cm x 135 cm balloon (Cordis Corporation) with good angiographic result and improvement in collaterals to the PT. An Armada 5.0 mm x 250 mm x 135 cm was used to balloon the left SFA, with higher pressures proximally for better preparation for the use of the Supera self-expanding stent (Abbott Vascular).
A Supera 5.0 mm x 120 mm x 120 cm was carefully positioned in the distal SFA and deployed under magnified fluoroscopy to ensure appropriate deployment and avoiding stretching or compressing the stent. The lesion at the origin of the initial CTO still had residual stenosis, so it was ballooned further with an Armada 5 mm x 40 mm x 135 cm balloon. Then another Supera 5.0 mm x 40 mm x 120 cm was deployed in similar fashion overlapping the first stent and was postdilated using the same Armada 5 mm x 40 mm x 135 cm balloon.
Results
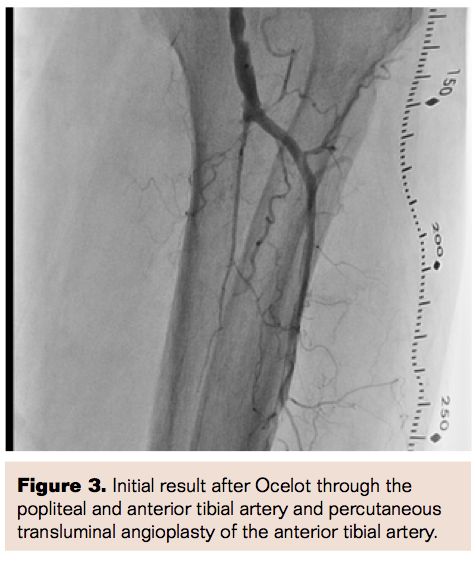
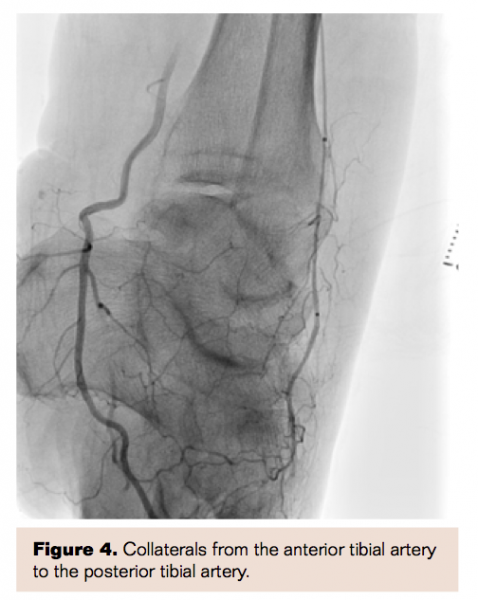 Following the intervention, the patient had excellent revascularization of the left SFA and the AT, which provided excellent collaterals to the PT (functional 2-vessel run-off to the lower extremity) (Figures 3 and 4. If the patient has further symptoms or critical limb ischemia, we will reassess with another ABI and consider opening the PT in retrograde fashion.
Following the intervention, the patient had excellent revascularization of the left SFA and the AT, which provided excellent collaterals to the PT (functional 2-vessel run-off to the lower extremity) (Figures 3 and 4. If the patient has further symptoms or critical limb ischemia, we will reassess with another ABI and consider opening the PT in retrograde fashion.
Conclusion
It is well recognized that subintimal revascularization of CTO with re-entry has been associated with reduced stent patency long term. It makes biologic and physiologic sense that avoiding a subintimal course would improve long-term patency. The real-time OCT in the Ocelot device provides assurance that the Ocelot catheter remains intraluminal as it chips at the occlusion. If the Ocelot could not complete penetration of the CTO, the Wildcat offers a more robust CTO device.
Starting the intervention intraluminal makes the use of the Wildcat the more aggressive device, safer and more likely to remain intraluminal. We have found from series of these cases that the Ocelot is very helpful in penetrating the proximal cap and first 1 cm to 2 cm of the CTO and when it could not be advanced any further, exchanging it for the Wildcat to overcome the rest of the occlusion. We believe that starting intraluminal with the Ocelot facilitates the Wildcat to successfully open the CTO while remaining intraluminal and avoiding dissections and perforations.
Editor’s Note: Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. Dr. Moualla reports no conflicts of interest regarding the content herein. Dr. Heuser reports stock ownership in Avinger.
Manuscript received April 3, 2014; manuscript accepted May 6, 2014.
Address for correspondence: Soundos K. Moualla, MD, FACC, Phoenix Heart Center, 555 N. 18th Street, Suite 300, Phoenix, Arizona 85006. Email: soundosmoualla@yahoo.com

