

Renal Denervation in Patients With Resistant Arterial Hypertension: A Single-Center Cohort Study and Learning Curve
Abstract
Objectives: To evaluate the effect of percutaneous renal denervation in patients with resistant arterial hypertension in a prospective, single-center cohort study. Materials and Methods: Renal denervation was performed using the Symplicity Renal Denervation System (Medtronic). Office blood pressure and 24-hour ambulatory blood pressure were measured before the procedure and then 1, 3, 6, and 12 months after the procedure. A total of 19 patients underwent renal denervation and completed the follow-up. Baseline office systolic blood pressure was 165±20 mmHg and ambulatory blood pressure 146±17 mmHg. Results: Office systolic blood pressure dropped significantly in all intervals from 3 months to 12 months (P<.05) while the diastolic blood pressure dropped only at the 1-month interval (P<.05). Ambulatory blood pressure showed only nonsignificant trends toward lower diastolic blood pressure at the 3-month interval and lower systolic blood pressure at the 12-month interval. Office heart rate displayed a nonsignificant decrease at the 6-month follow-up (P=.08). We observed higher use of spironolactone and lower use of centrally acting antihypertensives at the end of the study when compared to baseline. The decline in ABPM at the end of the study was dependent on the order in which the renal denervation procedures were performed (P<.05). Conclusions: Taken together, renal denervation was able to decrease patients’ office blood pressure with no distinct effect on ABPM. Blood pressure at the baseline and the order in which the procedures were performed were factors affecting the results.
VASCULAR DISEASE MANAGEMENT 2016;13(8):E183-E194
Key words: catheter ablation, renal artery intervention, interventional cardiology
_____________________________________________________________________
Resistant arterial hypertension is defined as blood pressure of 140/90 mmHg and higher despite triple antihypertensive therapy, including diuretic.1,2 This condition is accompanied by increased morbidity and mortality.3
The Symplicity HTN-1 clinical trial identified a significant decrease in blood pressure after renal denervation in patients with resistant arterial hypertension.4 Further trials brought similar promising results.5,6 Later, a large randomized controlled trial Symplicity HTN-3 showed a lack of efficacy for treatment of arterial hypertension by renal denervation.7-9 However, it was suggested that many invasive cardiologists participating at the Symplicity HTN-3 trial were inexperienced in the method of renal denervation and were still operating on a “learning curve”; some investigators performed as few as 2 or 3 procedures.10,11
Considering the above-mentioned limitation of the Symplicity HTN-3 trial, we sought to analyze the results of renal denervation in our hospital settings. In addition to the office (“casual”) blood pressure, we also performed the 24-hour ambulatory blood pressure monitoring (ABPM) and analyzed our learning curve.
Materials and Methods
Study Background
This is a prospective, noncontrolled cohort study, approved by the Ethics Committee of Pardubice Hospital (protocol number 374/25, date of approval March 25, 2011). Informed consent was obtained from all individual participants included in the study. All patients were treated in accordance with the Declaration of Helsinki. The study sponsor and supplier ended our study prematurely when the results of Symplicity HTN-3 became available.
Patient Selection
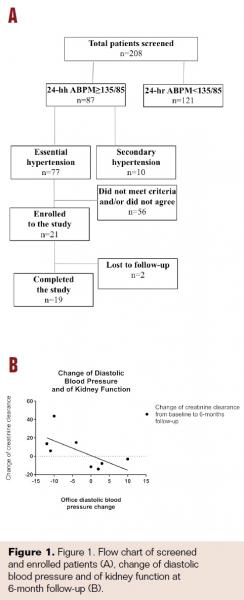 A total of 208 patients were screened from January 2012 to October 2013. Inclusion criteria were based on the expert consensus document from the European Society of Cardiology.12 Patients with repeated office blood pressure measurements over 140/90 mmHg plus systolic blood pressure during 24-hour ABPM of 135 mmHg or higher were invited to participate. Patients with secondary arterial hypertension, pseudoresistant hypertension, and severe kidney disease (eGFR<40 mL/min) were excluded. Of the suitable candidates, 21 patients agreed to be enrolled in the study. Compliance with pharmacotherapy was verified by measurement of plasmatic levels of antihypertensives (n=8), administration during hospital stay (n=6), or by patients recording the use in a diary (n=4). Of the 21 patients, 2 were lost to follow-up. Thus, 19 patients completed the study (Figure 1A). Demographic characteristics are as follows: age 57.1±14.7 years, 10 (53%) women, 8 (42%) patients with diabetes mellitus and body mass index (BMI) 30.4±2.8 kg/m2.
A total of 208 patients were screened from January 2012 to October 2013. Inclusion criteria were based on the expert consensus document from the European Society of Cardiology.12 Patients with repeated office blood pressure measurements over 140/90 mmHg plus systolic blood pressure during 24-hour ABPM of 135 mmHg or higher were invited to participate. Patients with secondary arterial hypertension, pseudoresistant hypertension, and severe kidney disease (eGFR<40 mL/min) were excluded. Of the suitable candidates, 21 patients agreed to be enrolled in the study. Compliance with pharmacotherapy was verified by measurement of plasmatic levels of antihypertensives (n=8), administration during hospital stay (n=6), or by patients recording the use in a diary (n=4). Of the 21 patients, 2 were lost to follow-up. Thus, 19 patients completed the study (Figure 1A). Demographic characteristics are as follows: age 57.1±14.7 years, 10 (53%) women, 8 (42%) patients with diabetes mellitus and body mass index (BMI) 30.4±2.8 kg/m2.
Procedure
The procedure was performed using the single-electrode Symplicity system (Medtronic) as described previously4 and according to instructions for use provided by Medtronic Inc. After intravenous analgosedation, an electrode was inserted via a femoral artery, and under fluoroscopy control, further introduced into one of the renal arteries. Sufficient vessel wall contact (with supposed proximity to the perivascular sympathetic fibers) was determined according to visual control using fluoroscopy and by measurement of electrical impedance. Then, a series of 4 to 6 radiofrequency impulses were performed in spiral fashion while progressing proximally; the same was repeated in the contralateral renal artery. Patient vital signs were monitored during the procedure. After the procedure, the patients stayed at the hospital overnight to check for any periprocedural complications.
Follow-up
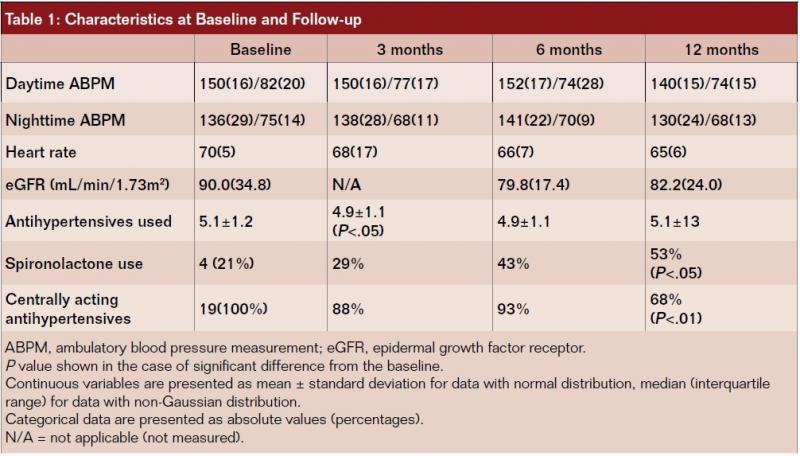
The patients were examined 1 month, 3 months, 6 months, and 12 months after the procedure. Office blood pressure, office heart rate, and 24-hour ambulatory blood pressure were recorded before the procedure and at every medical examination during the follow-up period. Office blood pressure was measured 3 times after at least 5 minutes of physical rest in a sitting position; the average of the second and third measurements was used. Intraindividual diurnal variation was minimized by scheduling every individual patient at the same time of day. In addition, the number of antihypertensives as well as the use of spironolactone and centrally acting antihypertensives were evaluated at all intervals. To verify safety of renal denervation, glomerular filtration rate was calculated at the 6-month and 12-month follow-up time point and were compared to the baseline values.
Patients with a drop in office blood pressure by 10 mmHg4 or with a drop in ABPM by 5 mmHg at 6 months follow-up were considered responders. When the values were missing, we considered the values obtained at the 12-month interval.
Statistical power of our analyses was limited by the lack of ABPM values in some of the patients during follow-up: 15 out of 19 patients came to the ABPM at 3 months, 8 of 19 at the 6-month interval, and 16 of 19 at the end of the follow-up. For office blood pressure, 17 patients fulfilled the follow-up at 3 months, 14 patients at 6 months and 16 patients at 12 months.
Statistical Evaluation
Continuous variables are presented as mean ± standard deviation for data with normal distribution, median (interquartile range) for data with non-Gaussian distribution. Categorical data are presented as absolute values (percentages). Most of the analyses were performed using Graph Pad Prism 6.07; the same software was used for the creation of graphs. Normality was tested by means of D’Agostino-Pearson omnibus test. Paired t test was used to compare numeric variables in the case of normal distribution and Mann-Whitney test for non-Gaussian distribution. Chi-square test was used for comparison of frequency. The association between number of lesions and the decline in blood pressure was tested by linear regression, with the number of lesions as an independent value. Similarly, linear regression with order of procedure performed as an independent value and decline in blood pressure as a dependent value was used for learning curve analysis. When comparing responders with nonresponders and when comparing the first and second half of participants;13 an unpaired t test in Microsoft Excel 2010 was used. A P value of <.05 was considered statistically significant.
Results
Safety
Two patients reported strong pain during renal denervation despite adequate analgosedation. Two other patients had episodes of vagal reaction (bradycardia with hypotension) following sheath removal with full spontaneous recovery. Otherwise the procedure was well tolerated. There were no major periprocedural complications, e.g. bleeding, pseudoaneurysm, thromboembolic events, or kidney injury. The estimated glomerular filtration rate displayed a nonsignificant drop from baseline to 6 months follow-up and remained unchanged from 6-month to 12-month follow-up (Table 1). There was no association between the numbers of lesions applied by radiofrequency ablation and change in glomerular filtration rate. When comparing changes in blood pressure and changes in kidney function, there was only a trend (P=.07) toward decreasing glomerular filtration rate with increasing diastolic blood pressure at 6-month follow-up (Figure 1B). No association was found between the order of procedure and change in kidney functions; change in glomerular filtration rate did not differ between the first and second half of participants (not shown).
Office Blood Pressure and Heart Rate
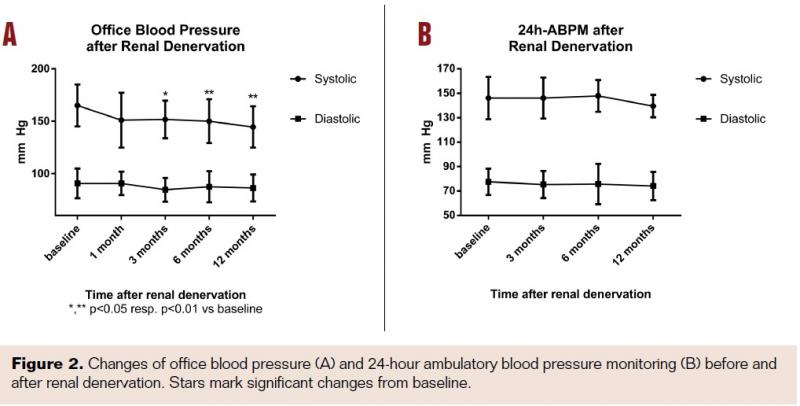
Office systolic blood pressure dropped in all intervals when compared to baseline -13±32 mmHg at 1 month (P=.16, not significant), -13±23 mmHg at 3 months (P<.05), -14±17 mmHg at 6 months (P<.01) and -18±21 mmHg at 12 months (P<0.01).
Diastolic blood pressure displayed the following trend: a decrease by -4±13 mmHg at 3 months (not significant), -7±19 mmHg at 6 months (not significant), and -4±10 mmHg at 12 months (P=.08, not significant) (Figure 2A).
Office heart rate displayed a nonsignificant decline during 3- to 12-month follow-up; the decrease was most pronounced at the end of follow-up: -6±5 beats per minute at 6 months and -5±7 beats per minute at 12 months (Table 1).
There were 8 responders among 16 participants at the 6-month follow-up (50%) and 14 of 18 at the 12-month follow-up (78%). When using the values from 12 months, in cases of missing values at 6 months, a total of 11 out of 19 patients (58%) were considered responders.
ABPM During Follow-up
The systolic blood pressure displayed a nonsignificant trend toward lower values at the end of the follow-up when compared to baseline: -7±16 mmHg (P=.097). The diastolic blood pressure displayed a trend toward lower values at the 3-month interval when compared to baseline: -5 mmHg ± 8 mmHg (P=.053) (Figure 2B).
When separated into daytime and nighttime values, there was a trend toward lower daytime systolic blood pressure at the end of the follow-up when compared to baseline: -10±18 mmHg (P=.057). In addition, both daytime and nighttime diastolic blood pressure were lower at the 3-month interval when compared to baseline (P<.05 for both). There was also a nonsignificant trend to lower daytime diastolic blood pressure at the end of the follow-up when compared to baseline (P=.099). As expected, blood pressure was higher during daytime than during nighttime (Table 1).
There were 4 responders among 8 participants at the 6-month follow-up (50%) and 8 out of 15 at the 12-month follow-up (53%). When using the values from 12 months, to account for cases of missing values at 6 months, a total of 7 out of 16 patients (44%) were considered responders.
Medication Use
The number of antihypertensive drugs dropped slightly from baseline -0.5±1.2 at the 3-month follow-up (P<.05). The count remained the same at 6 months, but it returned to baseline at the 12-month follow-up.
The use of spironolactone displayed an increasing trend during the follow-up. This increase reached statistical significance at the 12-month follow-up: from baseline 21% to 53% at 12 months (P<.05).
The use of centrally acting antihypertensives displayed a nonsignificant drop at the 3-month and 6-month follow-up; the decline from a baseline of 100% to 68% at the 12-month follow-up was significant (P<.01) (Table 1).
Comparison of Responders to Nonresponders
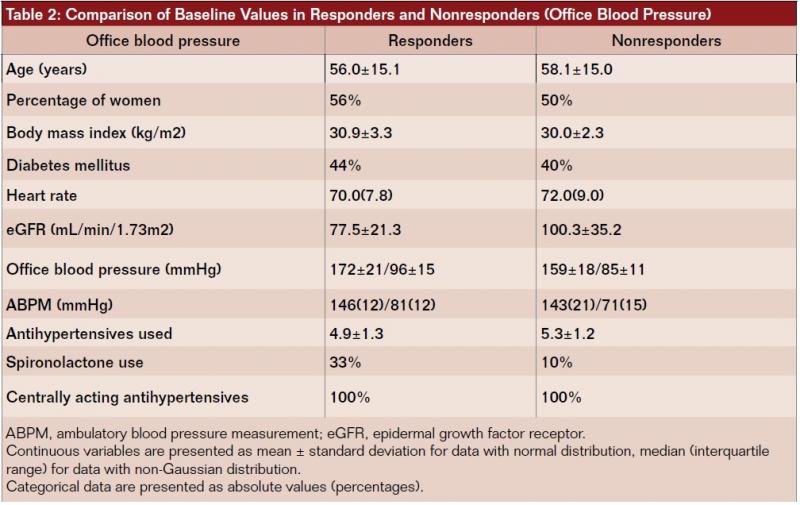
The responders had higher baseline office systolic blood pressure, higher baseline ABPM systolic blood pressure, a lower rate of spironolactone use, and a lower glomerular filtration rate than nonresponders. However, none of these differences reached the level of statistical significance (Table 2).
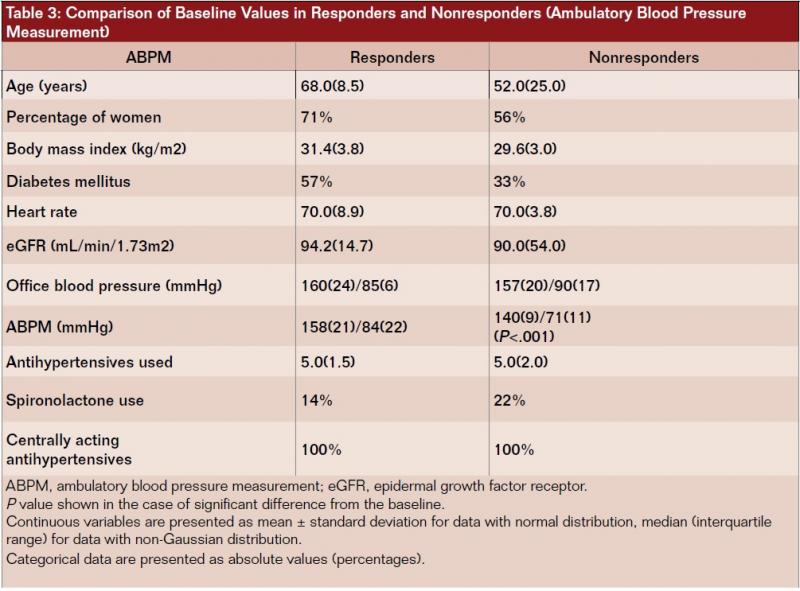
When separating the participants based on ABPM response, the responders had higher baseline systolic blood pressure than the nonresponders (P<.001). The following values in responders displayed nonsignificant trends when compared to nonresponders: greater age (P=.06), higher BMI, higher percentage of diabetes mellitus, and lower glomerular filtration rate (Table 3).
Role of Number of Lesions
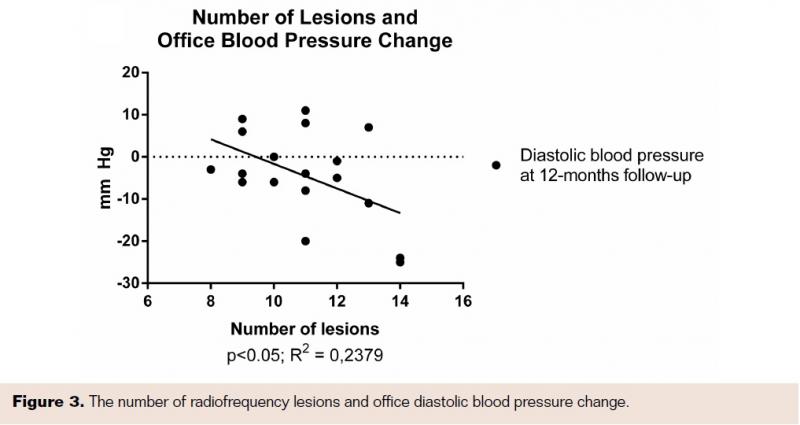
There was no association between the numbers of lesions applied by radiofrequency ablation with the change in office systolic blood pressure at any interval. On the other hand, there was an association between the office diastolic blood pressure decline at the end of the study and the number of lesions (P<0.05; Figure 3).
When evaluating the relationship between the number of lesions and ABPM, we observed only a trend toward deeper decrease of blood pressure at the end of the follow-up with greater number of lesions (P=.06; data not shown).
Number of lesions did not differ either between office blood pressure responders and the nonresponders, or between ABPM responders and nonresponders. There was no correlation between the order in which the procedures were performed and number of lesions applied; number of lesions did not differ in the first and second half of the cohort (data not shown).
Learning Curve Analyses
We were not able to prove any association between order of renal denervation with office blood pressure, neither systolic nor diastolic, at any time point. However, there was a dependence of both ABPM systolic and diastolic blood pressure change at the 12-month follow-up on the order of renal denervation (P<.01 for systolic blood pressure, P<.05 for diastolic blood pressure; Figures 4A and 4B). In addition, the averages of the values obtained during 3-month, 6-month, and 12-month follow-up were also dependent on the order of renal denervation; this was observed for both ABPM systolic and diastolic blood pressure (P<.01 for both; not shown).
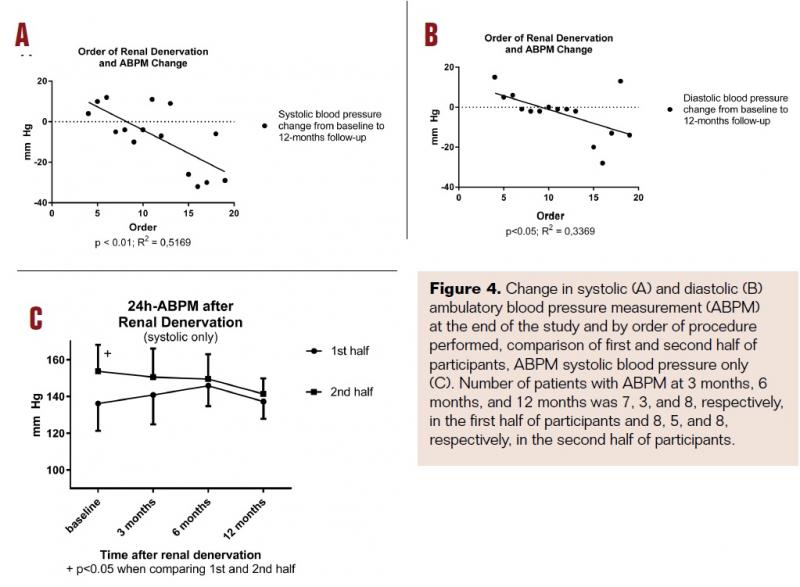
There were no significant differences in the changes of blood pressure between the first and the second half of participants, neither in office blood pressure nor in ABPM. There were nonsignificant trends toward further decline of blood pressure in the second half of participants compared to the first half from 6 months to 12 months: office blood pressure -5±14 at 6 months and -2±6 at 12 months in the first half vs -18±21 at 6 months and -11±23 at 12 months in the second half; ABPM was 0±8 at 6 months and +3±6 at 12 months in the first half vs -13±17 at 6 months and -7±12 at 12 months in the second half. The second half of participants also had higher baseline systolic ABPM than the second half (Figure 4C).
Discussion
Renal denervation was found to be safe because no major periprocedural complications were observed. There was no significant alteration of kidney function, which supports findings of other groups.7,14,15 The anatomical dispositions in our cohort allowed standard femoral access as recommended by the manufacturer. Transradial approach suggested by some authors15,16 would not be possible in our study due to length of the catheter.
In our cohort, we were able to document a decline in office blood pressure after renal denervation. On the other hand, the values obtained by 24-hour ABPM were not significantly affected. Ambulatory blood pressure monitoring is considered to be a more sensitive risk predictor of clinical cardiovascular outcomes, such as coronary morbid or fatal events and stroke, than office blood pressure.1 Therefore, the question remains whether the decline in office blood pressure in our study group was caused by bias or due to the fact that the patient cohort size was too small to identify any difference in ABPM.
The change of office diastolic blood pressure at the end of the follow-up was dependent on the number of lesions applied during the procedure. Interestingly, office systolic blood pressure was not affected by this factor at any time point. We found that the change in ABPM at the end of the follow-up was related to the order of procedure. This suggests that we were in a learning curve during the study. We suspect that the lack of significant differences in blood pressure as determined by ABPM may be attributed to the premature termination of the study. Another possible explanation is that the patient selection was more stringent in the second half of the participants as the second half of participants had more severe arterial hypertension at the baseline.
Our results are in accord with Desch et al, who reported no benefit of renal denervation on 24-hour systolic blood pressure at 6 months in patients with mild resistant arterial hypertension.17 The values of baseline ABPM in our cohort were similar to those reported in their study.
In a larger study, Mahfoud et al described an improvement in both office blood pressure and ABPM in patients with true resistant hypertension, whereas only office blood pressure was affected in patients with pseudoresistant hypertension.18 We considered their approach to separate patients according to baseline ABPM into true resistant hypertension and pseudoresistant hypertension to be optimal. Our findings of higher baseline ABPM in responders compared to nonresponders are in accord with their findings.
Sharp et al from the United Kingdom performed a multicenter retrospective analysis with an average of 15 cases per center, which is similar to the number in our study. They reported a decline in both office blood pressure and ABPM.19 In contrast, we were not able to prove differences in ABPM. This discrepancy might have been caused by markedly higher values of baseline ABPM in their study when compared to ours as well as higher statistical power of the multicenter analysis. When compared to the Symplicity HTN-3 study with an average of 4 renal denervations per center,7 the study by Sharp et al19 seems to have reached beyond the period of a “learning curve.” Clearly, it would be optimal to perform a randomized, sham-controlled trial with experienced cardiologists and a high number of renal denervations per center.
When we compared responders to nonresponders, we found that more severe hypertension at the beginning predicts a higher chance of its decrease after renal denervation. This is in accord with the data from the Global SYMPLICITY Registry20,21 in which the authors described deepest decline of blood pressure in patients with baseline systolic blood pressure of at least 160 mmHg; similar findings were observed by Id et al.22 On the other hand, very high values at the baseline were suggested to be the case of a big-day bias, that is, local maximum at the time of measurement while fluctuating over a longer time period.23
Besides high baseline blood pressure, low BMI was identified as a predictor of good response to renal denervation and, conversely, high BMI was associated with poor response.22 In the present study, the differences in BMI were neither significant nor clinically relevant.
Some authors reported a decrease in number of administered antihypertensives after renal denervation,24 whereas others reported no change.25 We did not observe any change in the total number of antihypertensive medications. We noted two significant changes: higher use of spironolactone and lower use of centrally acting antihypertensives at the end of the study when compared to baseline. Addition of spironolactone to the therapy might lead to a bias by proper titration of pharmacotherapy after the procedure. Using spironolactone was led by the results of the ASCOT-BPLA (Anglo-Scandinavian Cardiac Outcomes Trial-Blood Pressure Lowering Arm) study26 together with preliminary results of the ASPIRANT (Addition of Spironolactone in Patients With Resistant Arterial Hypertension) study.27,28 Efficiency of spironolactone for this indication was confirmed by other groups.29,30
There were some limitations in our study. First, the number of the patients was relatively low and may have led to negative results even in the presence of clinical effect. Second, some patients missed out some of the controls during the follow-up, thus further diminishing statistical power of our study. On the other hand, the percentage of ABPM available at the end of our study (79%) was similar to a multicenter study from the United Kingdom (73%)19 and higher than in the Global SYMPLICITY Registry (51%).20,21 Third, we used only a single-electrode system, whereas the multielectrode systems have been suggested to better position the lesions.31
Conclusions
Taken together, renal denervation was able to decrease patients’ office blood pressure, especially systolic blood pressure, but had no distinct effect in the ABPM. Blood pressure at the baseline and the order of performed procedure were factors affecting the results in the present study.
Editor’s note: Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. All authors declare that they have no conflicts of interest.
Manuscript received April 26, 2016; provisional acceptance given May 18, 2016; manuscript accepted June 9, 2016.
Address for correspondence: Vojtech Mezera, MD, PhD, The Buck Institute for Research on Aging, 8001 Redwood Blvd. Novato, CA 94945, United States. Email: wojslaw@seznam.cz
References
- Mancia G, Fagard R, Narkiewicz K, et al. 2013 ESH/ESC guidelines for the management of arterial hypertension: the Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). Eur Heart J. 2013;34(28):2159-2219.
- Calhoun DA, Jones D, Textor S, et al. Resistant hypertension: diagnosis, evaluation, and treatment: a scientific statement from the American Heart Association Professional Education Committee of the Council for High Blood Pressure Research. Circulation. 2008;117(25):e510-e526.
- Daugherty SL, Powers JD, Magid DJ, et al. Incidence and prognosis of resistant hypertension in hypertensive patients. Circulation. 2012;125(13):1635-1642.
- Krum H, Schlaich M, Whitbourn R, et al. Catheter-based renal sympathetic denervation for resistant hypertension: a multicentre safety and proof-of-principle cohort study. Lancet. 2009;373(9671):1275-1281.
- Symplicity HTN-2 Investigators, Esler MD, Krum H, et al. Renal sympathetic denervation in patients with treatment-resistant hypertension (The Symplicity HTN-2 Trial): a randomised controlled trial. Lancet. 2010;376(9756):1903-1909.
- Pokushalov E, Romanov A, Corbucci G, et al. A randomized comparison of pulmonary vein isolation with versus without concomitant renal artery denervation in patients with refractory symptomatic atrial fibrillation and resistant hypertension. J Am Coll Cardiol. 2012;60(13):1163-1170.
- Bhatt DL, Kandzari DE, O’Neill WW, et al. A controlled trial of renal denervation for resistant hypertension. N Engl J Med. 2014;370(15):1393-1401.
- Bakris GL, Townsend RR, Liu M, et al. Impact of renal denervation on 24-hour ambulatory blood pressure: results from SYMPLICITY HTN-3. J Am Coll Cardiol. 2014;64(11):1071-1078.
- Bakris GL, Townsend RR, Flack JM, et al. 12-month blood pressure results of catheter-based renal artery denervation for resistant hypertension: the SYMPLICITY HTN-3 trial. J Am Coll Cardiol. 2015;65(13):1314-1321.
- Luscher TF, Mahfoud F. Renal nerve ablation after SYMPLICITY HTN-3: confused at the higher level? Eur Heart J. 2014;35(26):1706-1711.
- Esler M. Renal denervation for treatment of drug-resistant hypertension. Trends Cardiovasc Med. 2015;25(2):107-115.
- Mahfoud F, Luscher TF, Andersson B, et al. Expert consensus document from the European Society of Cardiology on catheter-based renal denervation. Eur Heart J. 2013;34(28):2149-2157.
- Avital S, Hermon H, Greenberg R, Karin E, Skornick Y. Learning curve in laparoscopic colorectal surgery: our first 100 patients. Isr Med Assoc J. 2006;8(10):683-686.
- Hamza M, Khamis H. Renal sympathetic denervation for treatment of resistant hypertension: Egyptian experience. J Intervent Cardiol. 2014;27(4):423-427.
- Dong H, Jiang X, Liang T, et al. Transradial renal denervation for the treatment of resistant hypertension. J Invasive Cardiol. 2014;26(7):322-327.
- de Araujo Goncalves P, Teles RC, Raposo L. Catheter-based renal denervation for resistant hypertension performed by radial access. J Invasive Cardiol. 2013;25(3):147-149.
- Desch S, Okon T, Heinemann D, et al. Randomized sham-controlled trial of renal sympathetic denervation in mild resistant hypertension. Hypertension. 2015;65(6):1202-1208.
- Mahfoud F, Ukena C, Schmieder RE, et al. Ambulatory blood pressure changes after renal sympathetic denervation in patients with resistant hypertension. Circulation. 2013;128(2):132-140.
- Sharp A, Hameed A, Nightingale A, et al. Results from the UK renal denervation affiliation- 246 cases from 17 centres. J Hypertens. 2015;33(Suppl 1):e109.
- Mancia G, Mahfoud F, Narkiewicz K, et al. 4A.01: Long-term effects of renal artery denervation in real world patients with uncontrolled hypertension from the Global SYMPLICITY Registry. J Hypertens. 2015;33(Suppl 1):e49.
- Bohm M, Mahfoud F, Ukena C, et al. First report of the Global SYMPLICITY Registry on the effect of renal artery denervation in patients with uncontrolled hypertension. Hypertension. 2015;65(4):766-774.
- Id D, Bertog SC, Ziegler AK, et al. Predictors of blood pressure response: obesity is associated with a less pronounced treatment response after renal denervation. Catheter Cardiovasc Interv. 2015.
- Howard JP, Francis DP. Overcoming the three biases obscuring the science of renal denervation in humans: big-day bias, check-once-more bias and I-will-take-it-now bias. Trends Cardiovasc Med. 2015;25(2):116-118.
- Armaganijan L, Staico R, Moraes A, et al. Renal denervation using an irrigated catheter in patients with resistant hypertension: a promising strategy? Arq Bras Cardiol. 2014;102(4):355-363.
- Krum H, Schlaich MP, Sobotka PA, et al. Percutaneous renal denervation in patients with treatment-resistant hypertension: final 3-year report of the Symplicity HTN-1 study. Lancet. 2014;383(9917):622-629.
- Chapman N, Dobson J, Wilson S, et al. Effect of spironolactone on blood pressure in subjects with resistant hypertension. Hypertension. 2007;49(4):839-845.
- Vaclavik J, Sedlak R, Jarkovsky J, Kocianova E, Taborsky M. The effect of spironolactone in patients with resistant arterial hypertension in relation to baseline blood pressure and secondary causes of hypertension. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2013;157(1):50-55.
- Vaclavik J, Sedlak R, Plachy M, et al. Addition of spironolactone in patients with resistant arterial hypertension (ASPIRANT): a randomized, double-blind, placebo-controlled trial. Hypertension. 2011;57(6):1069-1075.
- Williams B, MacDonald TM, Morant S, et al. Spironolactone versus placebo, bisoprolol, and doxazosin to determine the optimal treatment for drug-resistant hypertension (PATHWAY-2): a randomised, double-blind, crossover trial. Lancet. 2015;386(10008):2059-2068.
- Rosa J, Widimsky P, Waldauf P, et al. Role of Adding Spironolactone and Renal Denervation in True Resistant Hypertension: One-Year Outcomes of Randomized PRAGUE-15 Study. Hypertension. 2016;67(2):397-403.
- Chokka RG, Delacroix S, Psaltis PJ, Anavekar NS, Worthley SG. Percutaneous renal denervation and the second generation EnligHTN System. Minerva Cardioangiol. 2014;62(1):99-104.
