


Transradial Carotid Artery Stenting Complicated With Neck Hematoma: Conservative Is a Valid Option!
Abstract
We describe a case of carotid artery stenting with a transradial approach resulting in an unusual complication that includes a neck hematoma caused by a guidewire small artery perforation. This complication could potentially be life threatening due to airway compression, but in our case was a mild hematoma with almost no effect and was conservatively managed with no intervention. This highlights the importance of using atraumatic guidewires, advancing the wire under roadmap guidance in the distal external carotid artery and following up on any patient symptoms post-intervention.
VASCULAR DISEASE MANAGEMENT 2021;18(2):E32-E34.
Introduction
Carotid artery stenting (CAS)—when performed by an experienced operator using an embolic protection device—provides a good alternative for carotid endarterectomy in high-risk patients. While femoral artery access is considered the gold standard during CAS, alternative access using the radial artery may be preferred in patients with peripheral arterial disease (PAD).1
Many trials show the feasibility and safety of radial access for CAS, especially for right carotid artery intervention. When directly compared to femoral artery interventions, radial access showed similar vascular complications and shorter hospitalization stays.2
Arterial perforations and neck hematomas are rare and could be fatal if they cause airway compression and may need arterial embolization to seal the arterial rupture or perforation. Early diagnosis and management is important and depends mainly on ultrasound diagnosis.3
Case Report
We report on a 56-year-old male patient with a history of diabetes and hypertension. He has a prior history of ischemic heart disease that was treated with multiple percutaneous coronary interventions (PCI). The patient experienced a transient ischemic attack (TIA) three weeks prior, for which carotid doppler was performed. The ultrasound revealed a right internal carotid artery stenosis with a systolic flow velocity of 300 cm/sec, and was then confirmed on computational tomography (CT) scan.
The patient’s case was discussed at our cardio team meeting and percutaneous carotid artery stenting was advised given the high cardiovascular risk for carotid artery endarterectomy. Right radial access was chosen for the procedure with a standard 6F sheath. An XB 3.5 guide catheter was advanced to the aortic arch. The guidewire was withdrawn to allow the catheter to bend on itself and with slight rotation we directed the catheter tip towards the brachiocephalic trunk.
A stiff Terumo 300 cm wire was advanced towards the common carotid artery (CCA), under road map guidance and the wire was advanced to the distal portion of the external carotid artery. The guide catheter and the sheath were withdrawn and exchanged for a 6F 90cm long sheath and advanced to the common carotid artery.
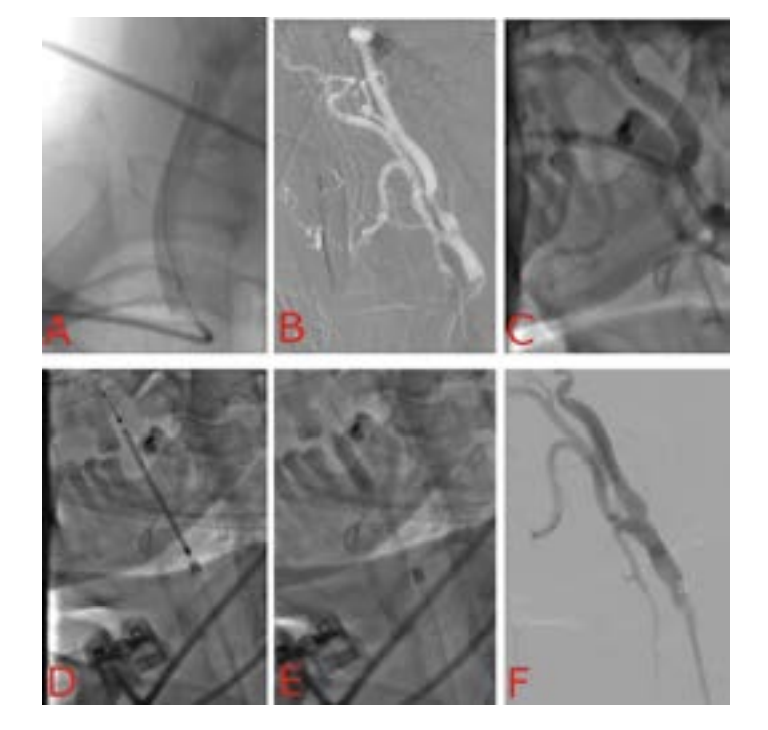
A Runthrough extra floppy wire was advanced to the distal internal carotid artery, and the spider FX filter wire was secured 3 centimeters distal to the ICA lesion. A Protege Rx carotid stent was then deployed followed by post dilation with a 5.0 x 20 mm balloon (Figure 1). The intraoperative course was smooth and then the patient was transferred to the ICU.
One hour later, the patient started to complain of neck pain at the site of intervention, and we observed a small supraclavicular soft swelling. Ultrasound was performed and revealed a fluid collection around the sternomastoid muscle with no continuation with the CCA or any of its branches (Figure 3A).

We reviewed the angiograms again and we discovered a small perforation at the takeoff of a very small branch of the external carotid artery (Figure 2). We reviewed the literature for recommendations and we found similar cases but at the ECA itself that required coiling and embolization.4
As the patient was stable and this small hematoma was not affecting his respiration, we took a conservative approach with close follow up and started soft compression over the sternomastoid muscle and ultrasound examination every two hours.
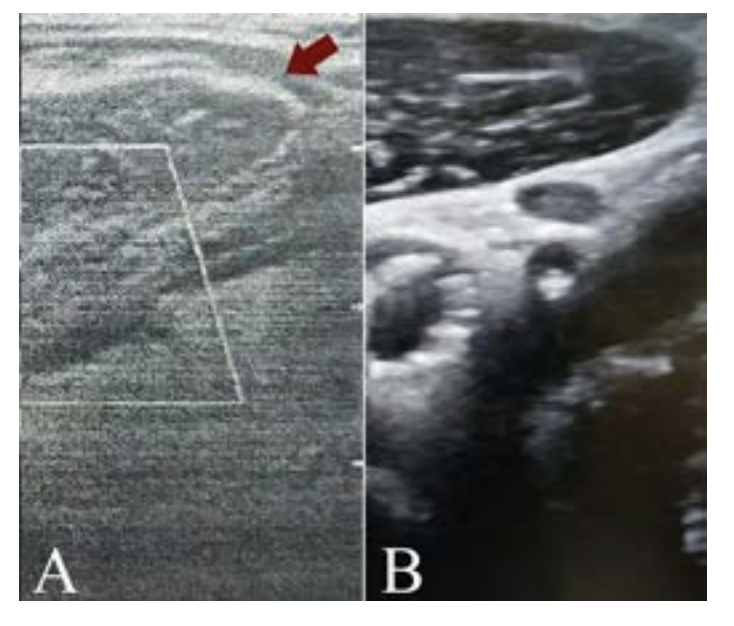
After 4 hours the ultrasound confirmed that the size of the hematoma was not increasing and patient symptoms started to resolve. At 24 hours the ultrasound confirmed that the hematoma size was decreasing so the patient was discharged home almost asymptomatic. Finally, the one week follow up ultrasound examination confirmed complete resolution of the hematoma and the patient was completely asymptomatic (Figure 3B).
Discussion
Stroke represents the most common complication of the CAS. Arterial ruptures and neck hematomas are rare and are described in some case reports and small registries. In most cases the arterial rupture is caused by the guidewire as most operators prefer Amplaz super stiff guidewires.5 Arterial rupture severity varies and may occur in the common carotid artery itself and may require stent graft implantation to seal the perforation or may involve other large side branches that would necessitate vessel embolization to stop the bleeding.4,6
Sonographic evaluation is the first step in recognizing hematomas and evaluating the size and rate of expansion.3 Basic experience with carotid artery ultrasound is necessary for operators to make a rapid diagnosis. In our case ultrasound was able to confirm the absence of continuity of the hematoma with any of the carotid arterial tree, and the operators’ experience with ultrasound helped for continuous monitoring of the hematoma and allowed us to avoid an unnecessary intervention.
In the modern era of percutaneous interventions, operator experience, and proper patient and toolbox selection all play an important role in preventing complications. The use of an atraumatic exchange guidewire, meticulous wire advancement in the external carotid artery, roadmap guidance as well as continuous monitoring of the guidewire tip during catheter exchanges are crucial for patient safety.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no financial relationships or conflicts of interest regarding the content herein. Authors state that human subjects have given informed consent and that the authors have conformed to institutional guidelines and those of the American Physiological Society.
Address for Correspondence: Osama Shoeib, MD, PhD, Email: oshouip@gmail.com Telephone: 00201111300044
REFERENCES
1. Jaroenngarmsamer T, Bhatia KD, Kortman H, Orru E, Krings T. Procedural success with radial access for carotid artery stenting: systematic review and meta-analysis. J NeuroInterv Surg. 2020;12(1):87-93.
2. Ruzsa Z, Nemes B, Pintér L, et al. A randomised comparison of transradial and transfemoral approach for carotid artery stenting: RADCAR (RADial access for CARotid artery stenting) study. EuroIntervention. 2014;10(3):381-391.
3. Millet JD, Cavallo JJ, Scoutt LM, Gunabushanam G. Sonographic evaluation of complications of extracranial carotid artery interventions. J Ultrasound Med. 2018;37(3):769-781.
4. Grandhi R, Gande A, Zwagerman NT, Jankowitz BT. Facial and neck hematoma after carotid artery stenting: an uncommon misadventure in endovascular carotid revascularization. BMJ Case Rep. 2013. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3794109/. Accessed November 6, 2020.
5. Ecker RD, Guidot CA, Hanel RA, et al. Perforation of external carotid artery branch arteries during endoluminal carotid revascularization procedures: consequences and management. J Invasive Cardiol. 2005;17(6):292-295.
6. Choi HC, Park SE, Choi DS, et al. Ruptured extracranial carotid artery: endovascular treatment with covered stent graft. J Neuroradiol. 2018;45(4):217-223.
