


Trends in the Incidence of Carotid Body Tumors in the United States From 1998 to 2011
VASCULAR DISEASE MANAGEMENT 2014;11(12):E298-E302
Abstract
Objective: The aim of this study was to characterize national trends in carotid body tumors (CBTs) in the United States by year, incidence, patient demographics, and hospital covariates. Methods: This was a retrospective cross-sectional analysis of hospital discharge data from 1998 to 2011 using the Health Care Utilization Project-Nationwide Inpatient Sample database. Patients with benign CBTs identified (ICD-9 227.5) were included and demographics, clinical covariates, and hospital inpatient charges were reported. Results: There were 684 cases of CBTs in the United States, with an overall incidence of 1 case per every 1 million people in 2011. The mean age of patients diagnosed with CBTs was 53.8 years ± 17.9 years, 60.4% were female, and the mean length of stay (LOS) was 3.3 days ± 3.9 days. Total hospital costs were approximately $9,763 per patient. The incidence of CBT has increased by 57% since 1998 (P<.001). Average age, gender, and LOS have not appreciably changed since 1998. 66.2% (452/683) underwent surgical management of the carotid body (ICD-9 39.8) of which 0.7% experienced a stroke. Conclusion: The incidence of CBT has increased by 37% since 1998 (P<.001). In the USA, the incidence is 1/1,000,000 people. Less than 1% of patients with CBT experience stroke as a complication of management.
Carotid body tumors (CBTs) are rare neoplasms that arise from chemoreceptors located within the adventitia near the carotid bifurcation.1,2 Most CBTs are sporadic, but familial types and hyperplastic forms also exist. These tumors constitute approximately 65% of head and neck paragangliomas and can be benign or malignant. Cranial nerve paralysis, pain, dysphagia, stroke, and Horner syndrome are all potential sequelae of this disease.1-3
CBT is understudied as the rarity of the disease makes clinical studies with collections of high patient numbers challenging. One of the largest patient series out of Europe included only 95 patients. This rarity of CBT makes studies about its overall incidence, trends, and outcomes difficult at a local level. The National Inpatient Sample (NIS) is a large, national database inclusive of a 20% stratified sample of all inpatient hospital admissions to nongovernmental hospitals in the United States. This database captures demographics, inpatient hospital charges, procedures, and outcomes for patients during a single hospital stay and is a validated way to determine national incidence patterns of rare disease processes.4
The aim of this study was to characterize national trends in CBTs over a decade in the United States by year, incidence, patient demographics, and hospital covariates.
Methods
This was a retrospective cross-sectional analysis of hospital discharge data from 1998-2011 using the Health Care Utilization Project-Nationwide Inpatient Sample (HCUP-NIS) database, which is a stratified 20% sample of all inpatient admissions to nonfederal acute care hospitals maintained by the Agency for Healthcare Research and Quality.4 It is the largest all-payer inpatient database in the United States, with records from approximately 8 million hospital stays each year.4
Records were limited to inpatients with benign CBT identified using the ICD-9 diagnosis code 227.5. Malignant carotid body tumors were excluded, because patients tend to have multiple hospitalizations, which would have led to overestimating the true incidence of CBTs.
Variables
Year was the primary independent variable of interest. Patient-level covariates included age, gender, and race/ethnicity (white, black, Hispanic, and other, as coded in HCUP-NIS). Clinical covariates included length of stay (LOS) and hospital inpatient charges.
Statistical Analysis
Statistical analysis was completed with the use of analysis of variance for continuous variables (i.e., age) and chi-squared test for categorical variables (i.e., sex, race, and mortality). The Mann-Whitney U test was used for LOS and total charges. Data analysis and management were completed using IBM SPSS (SPSS version 22.0; SPSS Inc). Statistical significance was set at a level of P<.05. All values are population estimates calculated using weighted samples and data provided by the US Census Bureau. Values are presented as mean ± standard deviation for age. Median costs are presented in 2014 USD corrected using the Consumer Price Index, and are available in the NIS starting in 2001. Pooled values from 1998 through 2000 were compared with those from 2009 through 2011 to calculate the increase in incidence. Student t test was utilized to compare these two groups to determine statistical significance.
Results
There were 684 cases of carotid body tumor in the United States between 1998 and 2011, with an overall incidence of 1 case per every 1 million people in 2011 (Table 1). The mean age of patients diagnosed with carotid body tumor was 53.8±17.9 and the majority was female (60.4%). Mean LOS was 3.3±3.9 days and total hospital costs were approximately $9,763 (2014 USD) per patient. Table 1 details the breakdown per year of the incidence, demographics, LOS, and total charges of carotid body tumor from 1998 to 2011.
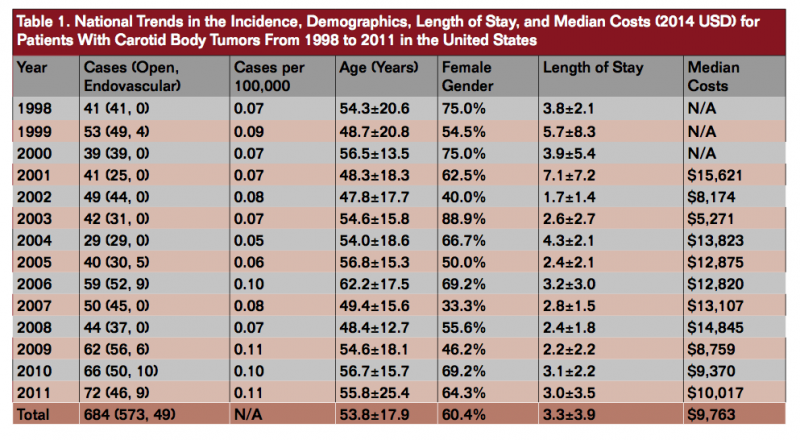
The incidence of CBT has increased by 37% since 1998 (P<.001) when comparing pooled values from 1998 through 2000 against values from 2009 through 2011. On trend analysis, there was also a significant decrease in median costs (P<.05). Average age, gender, and LOS have not appreciably changed since 1998. For the overall group, 83.8% (573/684) underwent surgical management of the carotid body (ICD-9 39.8, 39.89, and 38.62) of which 0.7% experienced a stroke. Of these 684 patients, 49 underwent endovascular embolization and/or stent placement (ICD-9 39.50, 39.72, or 39.90); 34 of 49 underwent endovascular intervention followed by open surgery after an average of 2 days between procedures. The remaining 15 patients underwent endovascular intervention and were discharged, potentially for later resection. Overall, 85.1% of patients were discharged to home, 8.5% discharged to home with home health care, and 6.4% discharged to a skilled nursing facility or intermediate care facility. There were no deaths in this series.
Within this patient group, the majority of patients were white (76%) followed by black (13%) and Hispanic (11%). There was no difference by race with regard to age, gender, or LOS but median costs were significantly higher for Hispanic patients ($15,756) compared to white ($9,448) and black patients ($9,539, P<.001) (Table 2). From this data set, 49% of the patients were white women, 29% white men, 7% black women, 4% black men, 6% Hispanic women, and 5% Hispanic men.

Discussion
Few other studies exist reviewing the trends of CBT demographics, management, and outcomes over time. Luna-Ortiz et al conducted a retrospective study of 66 patients with 69 CBT that were managed over a 20 year period at a single institution.5 Similar to the findings in this study, females were diagnosed with CBT at significantly higher rates than men and the mean age of diagnosis of the cohort was 50 years. Interestingly, this study reported that Hispanic women may be at higher risk for CBT than the general population.5 Our data suggest that white women in their 5th decade of life are most susceptible to the development of CBT, as they are diagnosed more than 7 times as much as their black and Hispanic female counterparts. The incidence of CBT has increased by nearly 37% since 1998. Median costs associated with inpatient care have decreased somewhat from $15,621 in 2001 to $10,017 in 2011 possibly due to the increased utilization of endovascular techniques over open repair for benign CBT. Hispanic patients have a median cost of care that is 67% greater than whites and a longer LOS but in contrast to the conclusion of previous data, do not appear to have a higher incidence of CBT as compared to other races.5 Despite 30 of 49 patients having undergone endovascular intervention followed by open surgery for CBT within the last 4 years of the study, there is a trend toward shorter LOS over the study period (Table 1).
Identifying the incidence and risk factors associated with CBT are important as surgical resection is the mainstay of therapy and early detection with prompt surgical resection decreases morbidity from this tumor.6 Attempts at surgical excision of CBT began in 1880 but were treacherous, resulting in high rates of nerve damage, stroke, hemorrhage, and death.6-8 In 1971, Shamblin et al9 created a classification system to determine the resectability of CBT based on the proportion of carotid encirclement: type I had no encirclement, type II had partial encirclement and were hence more difficult to resect, type III were associated with total encirclement and were the most dangerous type for which to attempt resection.9 As these tumors grow, even benign CBT require resection to prevent compression of the carotid and surrounding structures. In the cohort of benign CBT, 84% of patients underwent resection. For patients who underwent surgical intervention, the overall national rate of stroke was similar (1%) which is in keeping with the reported stroke results from the literature.10 There were no deaths reported in the NIS from management of benign CBT; mortality from this process is rarely reported, with only isolated cases detailed in the literature.10
Limitations
This study uses an administrative database, which is limited with regard to the number of variables that can be measured. Follow-up data, operative times, adjunct procedures such as mandibular subluxation, and long-term outcomes are unavailable along with specifications of the tumor type or classification. This also limits the ability to calculate costs associated with CBT recurrence follow-up. Due to multiple hospitalizations in patients with malignant CBT, these patients could not be included in this study as it would have led to double counting and skewed the true incidence of all CBTs. Despite this, at least 15 patients may have been double counted as they underwent initial endovascular procedure and were discharged, presumably for later open surgery. Furthermore, the Shamblin classification for the CBTs is unknown, and some of the variation in cost may be due to procedures on more advanced tumors rather than race or gender.
Conclusion
The incidence of CBT has increased significantly over a 14-year period in the United States from 38 cases in 1998 up to 72 by 2011. White women in their 5th decade of life are most susceptible to the development of CBT. Stroke after surgical intervention is uncommon (0.7%), and mortality is rare (0% in this series).
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no disclosures related to the content herein.
Manuscript submitted July 7, 2014; final version accepted August 19, 2014.
Address for correspondence: Anahita Dua, MD, University of Texas-Houston, Center for Translational Injury Research, Department of Surgery, MSB 5.030, 6413 Fannin Street, Houston, TX 77034, USA. Email: anahita.dua@uth.tmc.edu.
REFERENCES
- Unlü Y, Becit N, Ceviz M, Koçak H. Management of carotid body tumors and familial paragangliomas: review of 30 years’ experience. Ann Vasc Surg. 2009;23(5):616-620.
- Grotemeyer D, Loghmanieh SM, Pourhassan S, et al. Dignity of carotid body tumors. Review of the literature and clinical experiences. Chirurg. 2009;80(9):854-863.
- Williams MD, Phillips MJ, Nelson WR, Rainer WG. Carotid body tumor. Arch Surg. 1992;127(8):963-967; discussion 967-968.
- Healthcare Cost and Utilization Project (HCUP)-NIS [database online]. Rockville, Md: July Agency for Healthcare Research and Quality; 2014. www.hcup-us.ahrq.gov/nisoverview.jsp.
- Lim JY, Kim J, Kim SH, et al. Surgical treatment of carotid body paragangliomas: outcomes and complications according to the shamblin classification. Clin Exp Otorhinolaryngol. 2010;3(2):91-95.
- Soto GS, Valdes EF, Kramer Sch A, et al. Carotid body tumors: report of ten cases. Rev Med Chil. 2007;135(11):1414-1420.
- Köhler HF, Carvalho AL, Mattos Granja NV, Nishinari K, Kowalski LP. Surgical treatment of paragangliomas of the carotid bifurcation: results of 36 patients. Head Neck. 2004;26(12):1058-1063.
- Desmond TH, Christopher HK. Current concepts in the management of carotid body tumours. Med J Malaysia. 2010;65(4):268-270.
- Knight TT Jr, Gonzalez JA, Rary JM, Rush DS. Current concepts for the surgical management of carotid body tumor. Am J Surg. 2006 Jan;191(1):104-110.
- Sajid MS, Hamilton G, Baker DM; Joint Vascular Research Group. A multicenter review of carotid body tumour management. Eur J Vasc Endovasc Surg. 2007 Aug;34(2):127-130.
