


Mechanical and Pharmacological Treatment of Symptomatic Acute Portomesenteric Venous Thrombosis Through a TIPS Tract
© 2023 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Vascular Disease Management or HMP Global, their employees, and affiliates.
VASCULAR DISEASE MANAGEMENT 2023;20(10):E183-E192
Abstract
Acute portal vein thrombosis (PVT) is a relatively uncommon cause of abdomen pain and is associated with significant morbidity and mortality, especially when the superior mesenteric vein (SMV) is involved.1,2 Common symptoms of PVT are abdominal pain, nausea, anorexia, and vomiting. Loose stools, with or without bloody diarrhea, are seen in SMV thrombosis.3 Severe cases with intestinal gangrene or perforation present with peritonitis. Medical management is often unsuccessful. Surgical management is associated with significant morbidity and complications. Surgical resection of the involved intestinal segment is often reserved for patients who develop intestinal gangrene and perforation. The role of interventional radiology and minimally invasive procedures is newly evolving and is found to be successful in treating acute portal and SMV thrombosis.4,5,6 In this study, we describe the technique and results in patients who were treated with mechanical and pharmacological clot lysis through a TIPS tract.
Epidemiology and Etiopathogenesis
Incidence of acute portomesenteric thrombosis is 2.7 per 100,000.7 Though the main causes of mesenteric thrombosis can be divided based on Virchow’s triad (venous stasis, hypercoagulable state, and endothelial injury), they commonly coexist. Conditions that predispose to venous stasis are Budd-Chiari syndrome (BCS) and portal hypertension secondary to chronic liver disease. Hypercoagulable states can be inherited, such as factor V Leiden gene mutation, protein C/S deficiency, antithrombin III deficiency, hyperhomocystenemia, and acquired conditions such as malignancy, myeloproliferative disorders, pregnancy, and oral contraceptive use. Endothelial injury can occur in pancreatitis, colitis, placement of surgical shunts, and direct injury during surgery.8,9
Acute portomesenteric thrombosis has high morbidity and mortality and requires prompt treatment. The mortality rate ranges from 20% to 50%.10 Management options include medical, endovascular, and surgical approaches. Recently, there has been an inclination toward nonoperative management. Advances in endovascular techniques make endovascular management a viable option in treating acute portomesenteric thrombosis.11,12 If untreated, it may lead to cavernoma formation and portal hypertension.13
Diagnosis
Doppler ultrasonography is easily available and quick to assess portal and mesenteric circulation in patients with clinical suspicion of acute PVT. Sometimes, acute PVT may be detected on imaging incidentally while evaluating patients with abdominal symptoms. However, the visualization is dependent on an acoustic window. Assessment of the SMV in its entire extent is limited by Doppler scan. Contrast-enhanced computed tomography (CECT) is the mainstay in assessing the portomesenteric vasculature. CECT is rapid, accurate, and delineates the extent of the thrombosis. Information regarding bowel enhancement and intraperitoneal free air and intramural free air is obtained through CT, which is crucial in assessing bowel gangrene. In patients with elevated creatinine, magnetic resonance imaging (MRI) angiography can be used to assess the portomesenteric vasculature. However, MRI is time consuming and may not be as readily available as CT imaging. CT and MRI provide information about the rest of the abdomen and can establish the cause (eg, pancreatitis). Filling defects in the portal vein and SMV in the portal venous phase are the single most important finding indicative of portomesenteric thrombosis. Bowel wall edema, mesenteric congestion, intramural air, intraperitoneal free air, and portal cavernoma are other secondary signs and sequelae of portomesenteric thrombosis.14 The extension of the thrombus into the SMV is the most important finding, which determines the outcome and prognosis. The SMV can be accurately delineated with a CECT scan. CECT scan also delineates any chronic nature of the thrombus, such as attenuated portal vein and SMV with collateral formation. Interventional radiology options may not be beneficial for these patients. Such patients are excluded from the study.
Materials and Methods
A total of 6 patients (4 men, 2 women; median age, 35 years; age range 24-51) who underwent catheter-directed thrombolysis and mechanical thrombectomy for acute portomesenteric thrombosis in our institute, a tertiary care center, were retrospectively analyzed. Institutional review board approval was obtained for the study and ethical committee clearance was obtained. Patient demographics and clinical and procedural data were collected from electronic medical records and the picture archiving and communication system of the hospital.
In all patients, the diagnosis was confirmed on CECT (Discovery CT750 HD [GE Healthcare] and Ingenuity Core [Philips]). The findings on CECT are provided in Table 1. We used the classification proposed by Yerdel et al.15 Grade 1: minimally or partially thrombosed portal vein (PV), wherein the thrombus is mild or confined to less than 50% of the lumen with or without extension into the SMV. Grade 2: greater than 50% occlusion of the PV, including total occlusion with or without minimal extension into the SMV. Grade 3: complete thrombosis of both the PV and proximal SMV. Grade 4: complete thrombosis of the PV and both proximal and distal SMV. All patients we analyzed had complete occlusion of the PV and SMV, grade 4. CT findings are summarized in Table 1.
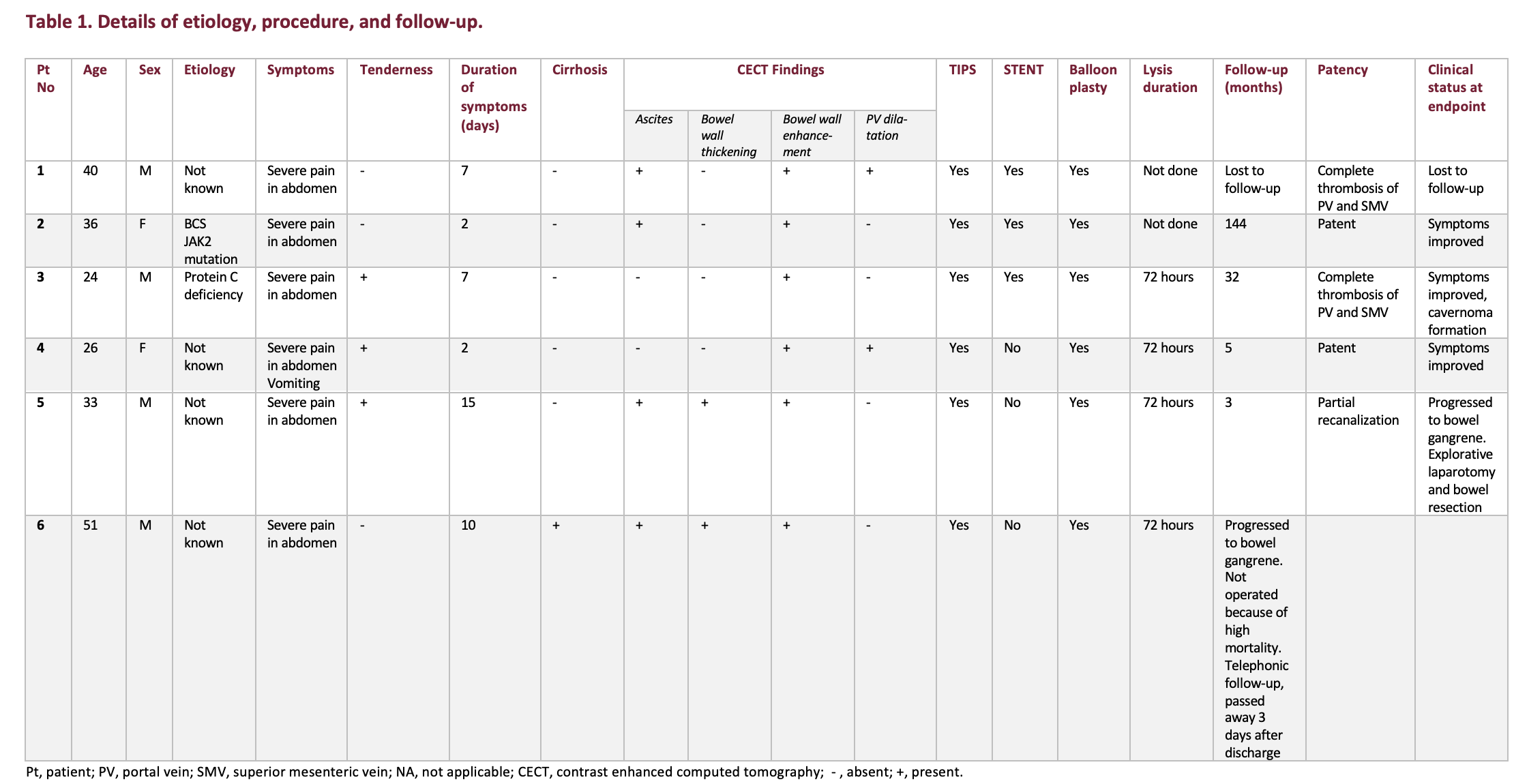
All patients were started on systemic anticoagulation. Patients who did not respond to systemic anticoagulation and had no improvement or worsening of clinical symptoms were taken up for intervention. Technical success was considered if partial recanalization was achieved immediately post procedure. Recanalization was considered successful only when the PV remained patent after the procedure and on 1-week follow-up. Symptomatic improvement was considered a clinical success.
During follow-up, patients were assessed clinically and the patency of the PV and SMV were assessed with Doppler ultrasound.
Management
All the 6 patients were started on oral anticoagulation with a therapeutic dose of subcutaneous low-molecular-weight heparin (LMWH), 60 mg every 12 hours once the diagnosis was established. One patient (patient 5) was found to have heparin resistance and was switched over to subcutaneous dalteparin, 12,000 U. During discharge, 5 patients were started on oral anticoagulants (warfarin) with a target international normalized ratio of 2-3. One patient (Patient 4) was put on rivaroxaban, 20 mg every day.
Thrombolysis was done by creating a TIPS/ direct intrahepatic portocaval shunt tract using Artis zee (Siemens Healthineers) and ultrasonography guidance (SonoScape), as described by Keshava et al.16 The right internal jugular vein was accessed under ultrasonography guidance. A modified Rosch-Uchida transjugular liver access set (RUPS-100; Cook Medical) was used to create a tract from the right hepatic vein to the right branch of the PV under ultrasonography and fluoroscopic guidance. In 1 patient (Patient 2) with irreparable hepatic veins, a direct tract from the inferior vena cava to the right branch of the PV was created. A 0.035" hydrophilic Glidewire (Terumo) was then passed into the SMV through the thrombus, and the thrombus was laced. The parenchymal tract was then balloon-plastied using a 10 mm x 4 cm Advance ATB PTA Dilatation Catheter balloon (Cook Medical). Self-expanding stents were deployed in patients 1, 2, and 3. Uncovered Zilver stents (Cook Medical) were deployed in Patient 1 and Patient 3. A Viatorr e-PTFE covered stent (Gore) was deployed in Patient 2. Using a 4F pigtail catheter (Cordis), thrombus was fragmented followed by suction thrombectomy using a 6F Envoy guiding catheter (Cordis). Pharmacological thrombolysis was performed in 4 patients (Patients 3,4,5, and 6) using continuous urokinase infusion of 50,000 units per hour for 48 hours and 100,000 units per hour from 48 to 2 hours via a 5F Mistique infusion catheter (Merit Medical) or 5F pigtail catheter (Cordis). In 5 patients, therapeutic heparinization was done with subcutaneous LMWH, 60 mg every 12 hours.
In Patient 6, there was right hepatic vein ostial narrowing. The hepatic vein was recanalized using a transjugular liver biopsy cannula, a 0.035" hydrophilic Glidewire, and a 4F multipurpose catheter (Cordis) using ultrasonography guidance.17
A portogram was done after infusion on the following day, followed by once every 24 hours. Repeat balloon plasty and further continuation of urokinase infusion was done based on recanalization status. Serial Doppler ultrasound surveillance was done during the initial week every 24 hours to look for thrombosis. After discharge, follow-up Doppler was done at 1 month, 3 months, and thereafter every 6 months. Four patients showed clinical improvement and were discharged from the hospital after 1 week. Two patients (Patients 5 and 6) showed clinical worsening despite PV recanalization, developed signs of bowel ischemia on follow-up CT after day 5, and showed signs of peritonitis. One patient underwent explorative laparotomy and 60 cm of gangrenous small bowel was resected. He was subsequently discharged in stable condition. The other patient was not operated on considering the high risk of mortality due to underlying chronic liver disease and was given best supportive care. However, he expired after 3 days.
Results
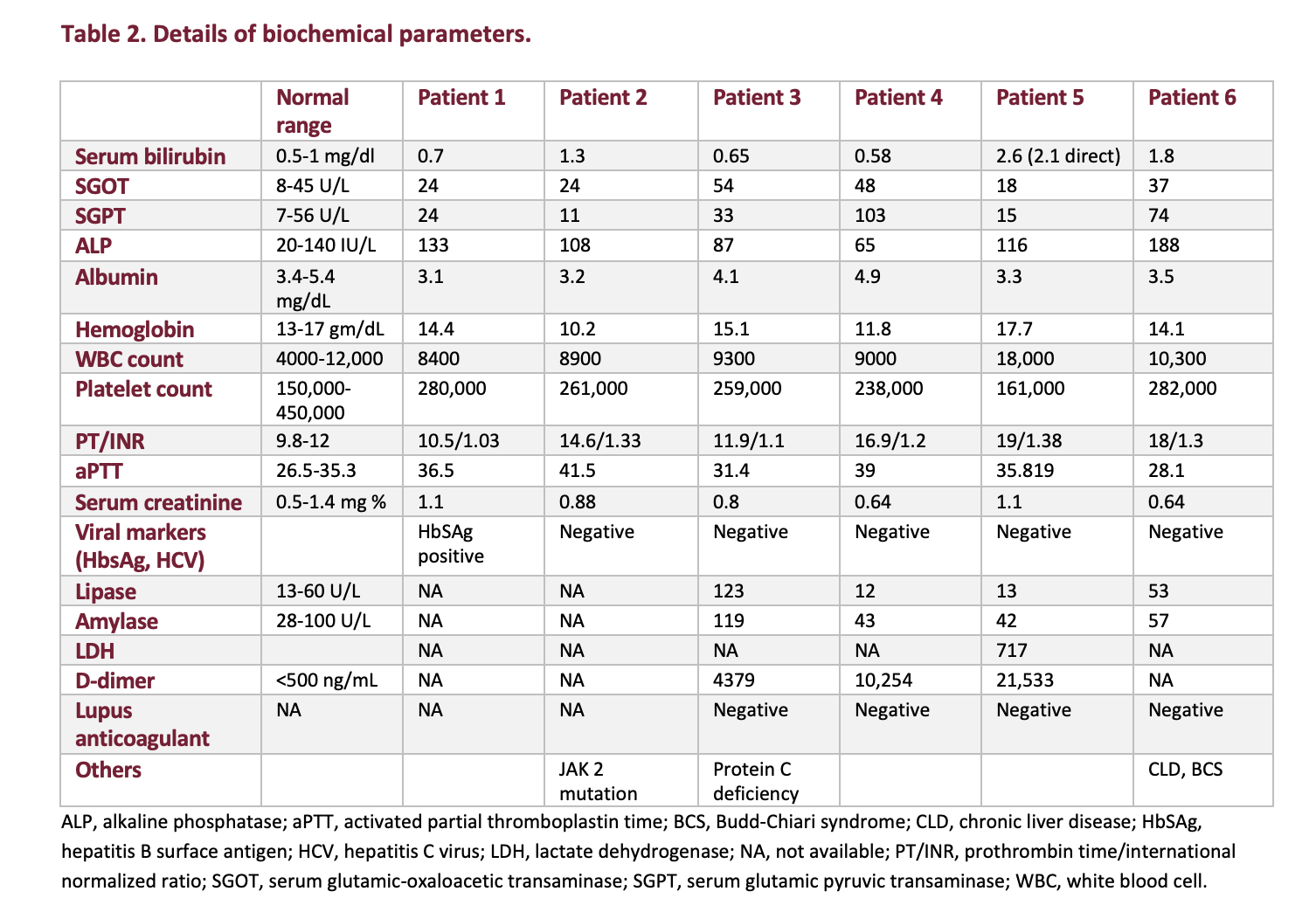
Details of the demographics, biochemical parameters, technique, and follow-up are provided in Table 1 and Table 2.
The thrombosed PV was accessed through a TIPS tract in all 6 patients. Technical success was achieved in 4 patients (66.6%) where portal vein recanalization was achieved. Out of the 4 patients, more than 50% recanalization was achieved in 2 patients and less than 50% recanalization was achieved in 2 patients.
The long-term patency of the recanalized PV is 100%. Three out of 4 patients in whom portal vein recanalization was achieved are on follow-up. One patient (Patient 6) expired due to bowel gangrene and underlying chronic liver disease after discharge.
Clinical success was achieved in 3 patients (50%) (Patients 2,3, and 4). Two patients (33.3%), despite partial recanalization (Patients 5 and 6), showed clinical worsening and progressed to bowel gangrene, developed signs of ischemia on follow-up CT after day 5, and showed signs of peritonitis. One of them (Patient 5) underwent explorative laparotomy and 60 cm of gangrenous small bowel was resected, after which he was discharged in stable condition. The other patient (Patient 6) was not operated considering the high risk of mortality due to underlying chronic liver disease and was given best supportive care.
In 2 patients, the PV remained thrombosed (Patients 1 and 3). Out of them, 1 patient (Patient 3) improved clinically and had cavernoma formation on 3-month follow-up.
Out of 6 patients, 4 have been on follow-up (mean follow-up 44 months; range 3-144 months). All 4 patients are doing well. The PV is patent in 3 and in 1 patient (Patient 3), the PV was not recanalized after thrombectomy.
One patient (Patient 6) expired secondary to bowel gangrene and underlying chronic liver disease after 3 days of discharge. Patient 1 was lost to follow-up in the institution.
Management and follow-up are summarized in Table 2.
Discussion
Acute PVT is a relatively rare cause of acute abdomen but is associated with high mortality and morbidity.18,19,20 Early diagnosis and management are necessary for better prognosis.21 Systemic anticoagulation is the initial treatment option, which may not be successful for every patient. Recanalization rates with therapeutic anticoagulation have not been promising.22 Systemic anticoagulation must be initiated as early as possible to achieve better results, as recanalization rate decreases from 69% to 25% when anticoagulation is initiated in the second week instead of the first week.23 A study by Maldonado et al showed that there is a high chance of developing portal hypertension even after recanalization of the PV using systemic anticoagulation.24 Systemic thrombolysis has also been tried; however, the risk of bleeding is high.25
In patients who have shown no symptomatic improvement with anticoagulation, minimally invasive interventions can be offered. Various approaches for recanalization are described in multiple case series, such as transjugular, transhepatic, and trans-splenic. Indirect thrombolysis through the SMA has also been described.11,12,26,27 Intestinal perforation and bowel gangrene should be excluded prior to intervention. It is often challenging to diagnose bowel gangrene clinically or on imaging. Definitive signs of bowel gangrene, such as intramural air and PV air, are not always seen on imaging.
There is no definitive timeline that distinguishes acute from chronic PVT, but the widely accepted clinical definition of acute PVT is symptom duration less than 60 days.25
Liu et al stated that thrombus has low density in the acute phase (less than 1 week), high density during the subacute phase (1-3 weeks), and low density during the chronic phase (more than 3 weeks).26 We used a CECT scan to study the extent and nature of the thrombus. All 6 patients were acute according to clinical definition, acute to subacute in nature according to imaging definition, and all the patients had involvement of the PV and SMV.
In our institution, we used a transjugular approach by which a TIPS tract was created, through which mechanical and chemical thrombolysis was done. Transjugular access and thrombolysis through a TIPS was preferred. When compared with image-guided percutaneous PV access, TIPS creation has the advantage of avoiding peritoneal or liver capsule breach, resulting in reduced chances of bleeding. This can even be performed in patients with ascites. A TIPS tract can also facilitate prolonged catheter stay if required.28,29 TIPS can also relieve the portal hypertension and act as a portosystemic shunt in patients with refractory ascites or variceal bleed.
Gipson et al described 3 types of image-guided techniques for creation of a TIPS: (1) fluoroscopic guidance with portography (contrast medium or carbon dioxide); (2) marker wire guidance; and (3) ultrasound (US) guidance.30,31 Since the PV is thrombosed, after puncture of the PV, there will not be backflow through the needle to confirm it. We used transabdominal ultrasonography to gain the PV access. Even in a nonthrombosed vein, we use transabdominal US guidance to gain the PV access, as the needle can be visualized in real time and the course of the needle can be tracked.32
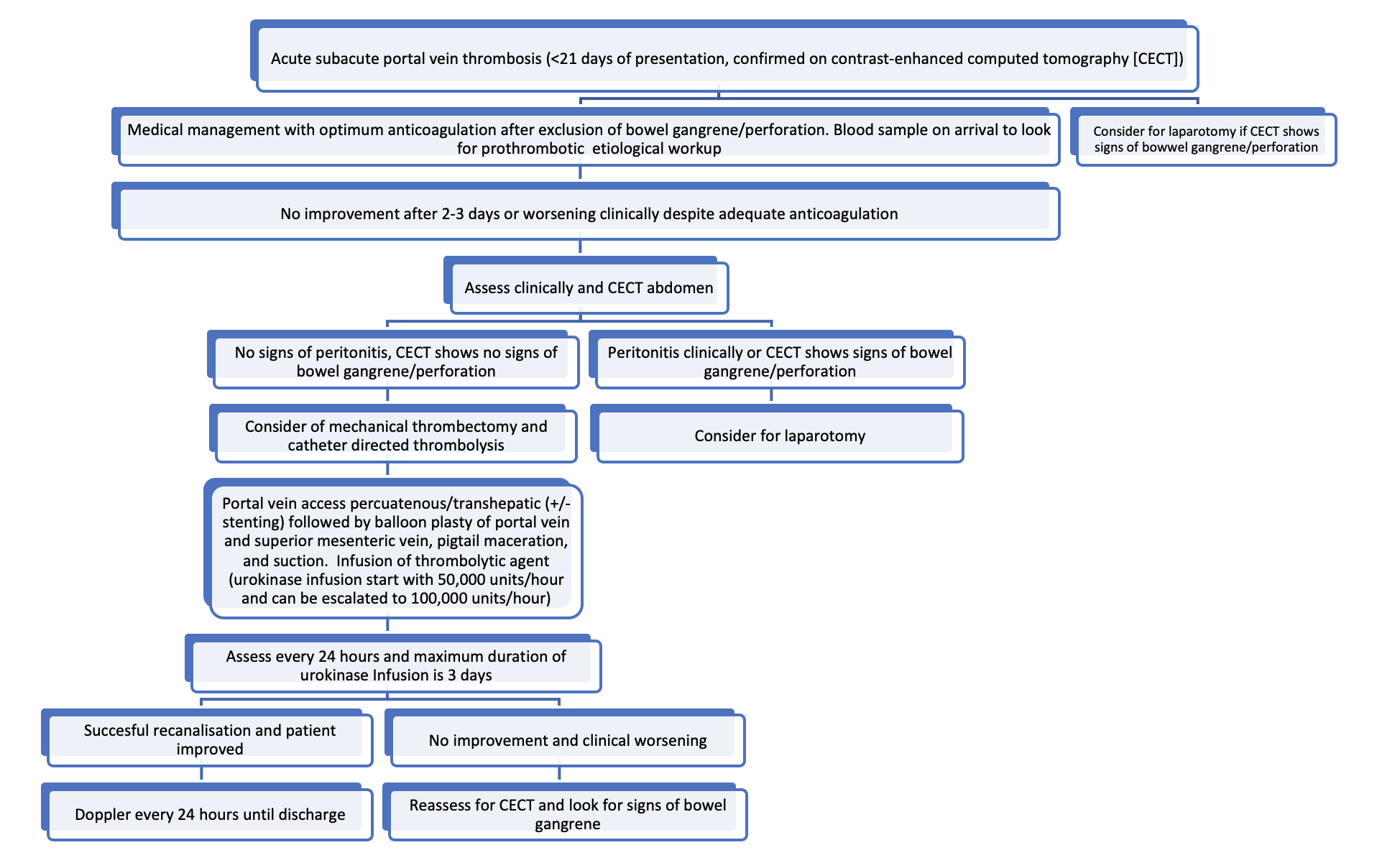
After access was gained through a TIPS into the portal system, mechanical thrombectomy was done in 6 patients. Additional thrombolysis was performed in 4 patients with urokinase at a dose of 50,000 units per hour for 48 hours and 100,000 units per hour from 48 to 72 hours post intervention. Urokinase is a plasminogen activator with a short half-life of 15 to 20 minutes. There are no established guidelines for urokinase infusion. Liu et al described catheter-directed urokinase infusion over a short period of time.26 There is risk of haemorrhage with urokinase infusion and heparinization, so patients should be under continuous monitoring. Contraindications for urokinase must be checked before infusion. In our study, we did not encounter any bleeding complications. Similar doses of urokinase were infused by Klinger et al and no bleeding complications were encountered.33 The treatment algorithm followed in our institute is formulated in Figure 1.
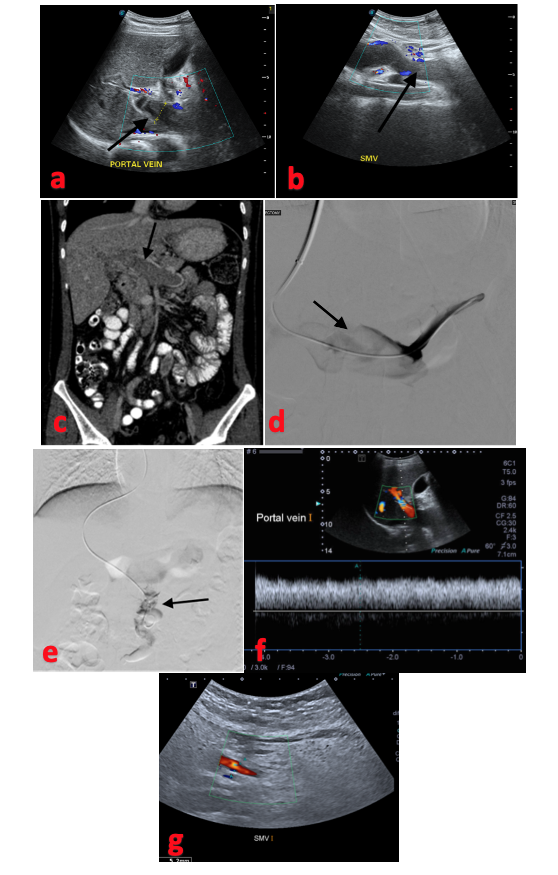
Technical success was achieved in 4 patients; however, out of the 4 patients, 2 (patients 5 and 6) worsened clinically and progressed to bowel gangrene. Klinger et al had a similar result in 2 out of 17 patients.33 The 2 patients (patients 2 and 4) in whom recanalization was achieved and improved clinically were diagnosed promptly, and intervention was done early (within 2 days of symptom onset) (Figure 2). The 2 patients who had clinical worsening had bowel wall thickening on preprocedural CT, although there was mucosal enhancement and no clinical signs of peritonitis. Surgery consultation was sought, and they were inclined toward nonoperative management as there were no obvious clinical signs of gangrene. A combined surgical approach and local thrombolysis were described in a small case series by Loss M et al.34 The combined approach may benefit patients who already have impending signs of bowel ischemia.
In our cases series, the recanalization rate was achieved in 66.6%. A higher percentage of recanalization rates were described in studies by Liu et al (73%) and Klinger et al (94.1%).26,33 Similar to our case series, the etiology was variable. The long-term patency where recanalization was achieved was good in 3 patients, and the PV was patent on follow-up (Patient 6 expired). Similar results were also shown in study by Klinger et al.33
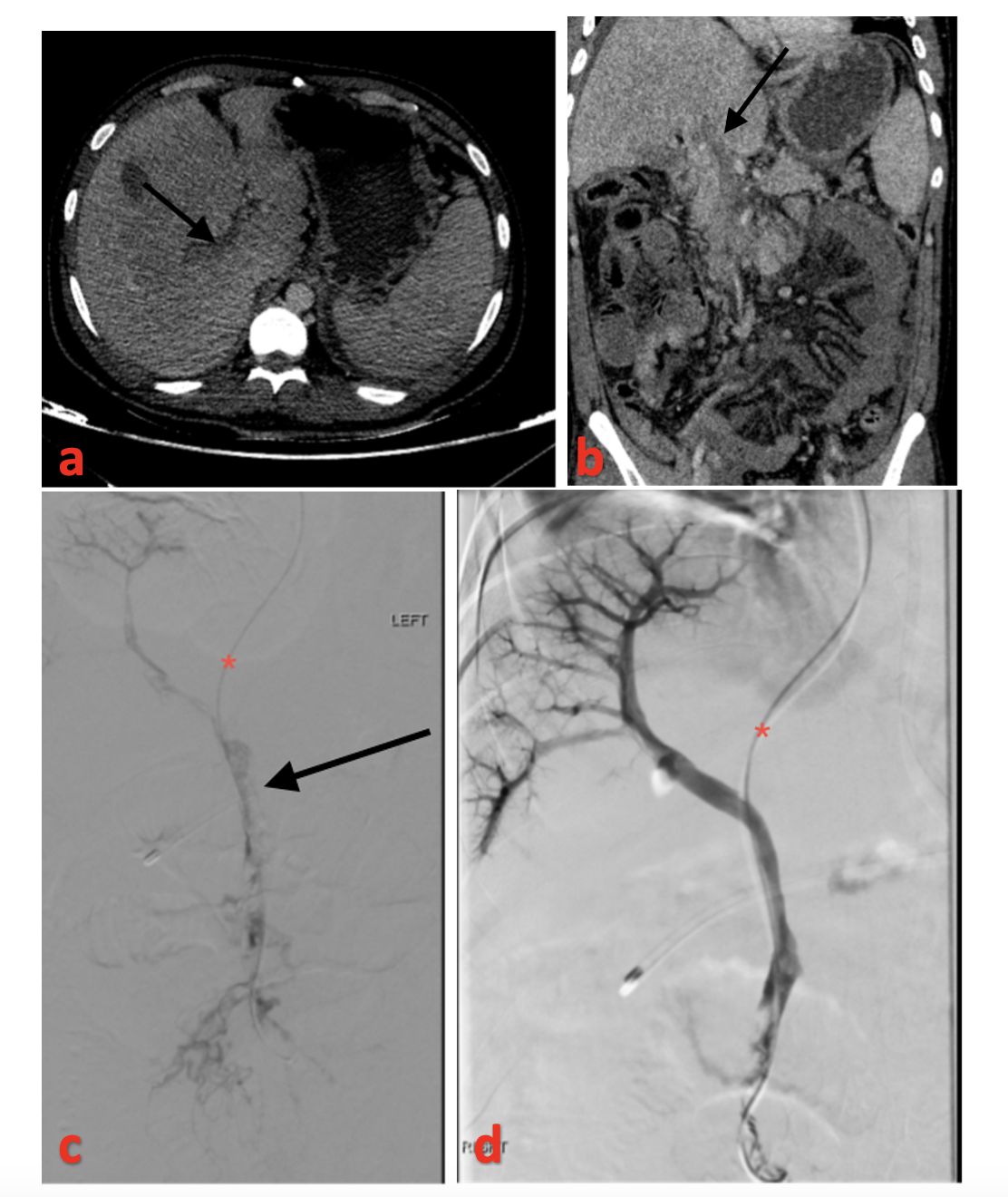
Overall clinical improvement was seen in 4 patients (66.6%), although 1 patient underwent bowel resection (Patient 5, Figure 3), and in 1 patient the PV was not recanalized (Patient 3) and had cavernoma formation on follow-up.
Study Limitations
Limitations of the study include its small sample size, retrospective nature, and variations of technical protocol for treatment. The small sample size can be attributed to the rarity of the condition, and only a small proportion of patients need intervention. The techniques and hardware in interventional radiology are rapidly evolving, which partially explains the non-uniformity among the technique followed.
Conclusions
Catheter-directed thrombolysis through a TIPS tract is a safe and effective modality in treating patients presenting with acute portomesenteric thrombosis and inadequate clinical response despite optimal systemic anticoagulation. Bowel gangrene at the time of presentation is a relative contraindication, and surgical resection of affected bowel should be considered in these cases. The long-term patency rate after recanalization appears promising. Although the entity is rare, the associated mortality is high and post-thrombotic sequelae are significant. Results seen in this small case series are encouraging; however, larger studies are required to formulate guidelines.
With this short experience, the treatment algorithm seen in Figure 1 is being followed in patients presenting with acute portomesenteric thrombosis. n
The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no financial relationships or conflicts of interest regarding the content herein.
Manuscript accepted September 8, 2023.
Address for correspondence: Shyamkumar N. Keshava, MBBS, DNB, FRCR, Radiology Department, Christian Medical College, Vellore, Tamil Nadu, India. Email: shyamkumar.n.keshava@gmail.com
REFERENCES
1. Lladó L, Fabregat J, Castellote J, et al. Management of portal vein thrombosis in liver transplantation: influence on morbidity and mortality. Clin Transplant. 2007;21(6):716-721. doi:10.1111/j.1399-0012.2007.00728.x
2. Rhee RY, Gloviczki P, Mendonca CT, et al. Mesenteric venous thrombosis: still a lethal disease in the 1990s. J Vasc Surg. 1994;20(5), 688-697. doi:10.1016/S0741-5214(94)70155-5
3. McKinsey JF, Gewertz BL. Acute mesenteric ischemia. Surg Clin North Am. 1997;77(2):307-318. doi:10.1016/s0039-6109(05)70550-8
4. Valentin N, Korrapati P, Constantino J, Young A, Weisberg I. The role of transjugular intrahepatic portosystemic shunt in the management of portal vein thrombosis: a systematic review and meta-analysis. Eur J Gastroenterol Hepatol. 2018;30(10):1187-1193. doi:10.1097/MEG.0000000000001219
5. Streitparth F, Santosa F, Milz J, et al. [Transjugular intrahepatic portosystemic shunt in patients with portal vein thrombosis]. Rofo. 2008;180(10):899-905. doi:10.1055/s-2008-1027698
6. Li CQ, Mao Y, Xu DH, Zhou A, Li P. Clinical observation on interventional recanalization of portal vein stenosis and occlusion due to thrombosis. Zhongguo Gandan Waike Zazhi. 2007;13:304-306.
7. Acosta S, Alhadad A, Svensson P, Ekberg O. Epidemiology, risk and prognostic factors in mesenteric venous thrombosis. Br J Surg. 2008;95(10):1245-1251. doi:10.1002/bjs.6319
8. Valla DC, Condat B. Portal vein thrombosis in adults: pathophysiology, pathogenesis and management. J Hepatol. 2000;32(5):865-871. doi:10.1016/s0168-8278(00)80259-7
9. Chawla Y, Duseja A, Dhiman RK. Review article: the modern management of portal vein thrombosis. Aliment Pharmacol Ther. 2009;30(9):881-894. doi:10.1111/j.1365-2036.2009.04116.x
10. Kumar S, Sarr MG, Kamath PS. Mesenteric venous thrombosis. N Engl J Med. 2001;345(23):1683-1688. doi:10.1056/NEJMra010076
11. Rosenqvist K, Eriksson LG, Rorsman F, Sangfelt P, Nyman R. Endovascular treatment of acute and chronic portal vein thrombosis in patients with cirrhotic and non-cirrhotic liver. Acta Radiol. 2016;57(5):572-579. doi:10.1177/0284185115595060
12. Wolter K, Decker G, Kuetting D, et al. Interventional treatment of acute portal vein thrombosis. Rofo. 2018;190(8):740-746. doi:10.1055/a-0631-9265
13. Quarrie R, Stawicki SP. Portal vein thrombosis: what surgeons need to know. Int J Crit Illn Inj Sci. 2018;8(2):73-77. doi:10.4103/IJCIIS.IJCIIS_71_17
14. Hauenstein K, Li Y. Radiological diagnosis of portal/mesenteric vein occlusion. Viszeralmedizin. 2014;30(6):382-387. doi:10.1159/000370055
15. Yerdel MA, Gunson B, Mirza D, et al. Portal vein thrombosis in adults undergoing liver transplantation: risk factors, screening, management, and outcome. Transplantation. 2000;69(9):1873-1881. doi:10.1097/00007890-200005150-00023
16. Keshava SN, Kota GK, Mammen T, et al. Direct intrahepatic cavo-portal shunts in Budd-Chiari syndrome: role of simultaneous fluoroscopy and trans-abdominal ultrasonography. Indian J Gastroenterol. 2006;25(5):248-250.
17. Keshava SN, Moses V, Surendrababu NRS. Cannula-assisted and transabdominal ultrasound-guided hepatic venous recanalization in Budd Chiari syndrome: a novel technique to avoid percutaneous transabdominal access. Cardiovasc Intervent Radiol. 2009;32(6):1257-1259. doi:10.1007/s00270-009-9615-6
18. Cohen J, Edelman RR, Chopra S. Portal vein thrombosis: a review. Am J Med. 1992;92(2):173-182. doi:10.1016/0002-9343(92)90109-o
19. Rhee RY, Gloviczki P. Mesenteric venous thrombosis. Surg Clin North Am. 1997;77(2):327-338. doi:10.1016/s0039-6109(05)70552-1
20. Gertsch P, Matthews J, Lerut J, Luder P, Blumgart LH. Acute thrombosis of the splanchnic veins. Arch Surg. 1993;128(3):341-345. doi:10.1001/archsurg.1993.01420150101018
21. Ferro C, Rossi UG, Bovio G, Dahamane M, Centanaro M. Transjugular intrahepatic portosystemic shunt, mechanical aspiration thrombectomy, and direct thrombolysis in the treatment of acute portal and superior mesenteric vein thrombosis. Cardiovasc Intervent Radiol. 2007;30(5):1070-1074. doi:10.1007/s00270-007-9137-z
22. Plessier A, Darwish-Murad S, Hernandez-Guerra M, et al. Acute portal vein thrombosis unrelated to cirrhosis: a prospective multicenter follow-up study. Hepatology. 2010;51(2):210-218. doi:10.1002/hep.23259
23. Turnes J, García-Pagán JC, González M, et al. Portal hypertension-related complications after acute portal vein thrombosis: impact of early anticoagulation. Clin Gastroenterol Hepatol. 2008;6(12):1412-1417. doi:10.1016/j.cgh.2008.07.031
24. Maldonado TS, Blumberg SN, Sheth SU, et al. Mesenteric vein thrombosis can be safely treated with anticoagulation but is associated with significant sequelae of portal hypertension. J Vasc Surg Venous Lymphat Disord. 2016;4(4):400-406. doi:10.1016/j.jvsv.2016.05.003
25. Malkowski P, Pawlak J, Michalowicz B, et al. Thrombolytic treatment of portal thrombosis. Hepatogastroenterology. 2003;50(54):2098-2100.
26. Liu FY, Wang MQ, Fan QS, Duan F, Wang ZJ, Song P. Interventional treatment for symptomatic acute-subacute portal and superior mesenteric vein thrombosis. World J Gastroenterol. 2009;15(40):5028-5034. doi:10.3748/wjg.15.5028
27. Hollingshead M, Burke CT, Mauro MA, Weeks SM, Dixon RG, Jaques PF. Transcatheter thrombolytic therapy for acute mesenteric and portal vein thrombosis. J Vasc Interv Radiol. 2005;16(5):651-661. doi:10.1097/01.RVI.0000156265.79960.86
28. Aytekin C, Boyvat F, Kurt A, Yologlu Z, Coskun M. Catheter-directed thrombolysis with transjugular access in portal vein thrombosis secondary to pancreatitis. Eur J Radiol. 2001;39(2):80-82. doi:10.1016/s0720-048x(01)00289-3
29. Mammen S, Keshava SN, Kattiparambil S. Acute portal vein thrombosis, no longer a contraindication for Transjugular Intrahepatic Porto-Systemic Shunt (TIPS) insertion. J Clin Exp Hepatol. 2015;5(3):259-261. Available from: doi:10.1016/j.jceh.2014.08.008
30. Gipson MG, Smith MT, Durham JD, et al. Intravascular US-guided portal vein access: improved procedural metrics during TIPS creation. J Vasc Interv Radiol. 2016;27(8):1140-1147. doi:10.1016/j.jvir.2015.12.002
31. Win AZ. Image guided portal vein access techniques in TIPS creation and considerations regarding their use. Ann Transl Med. 2016;4(11):226. doi:10.21037/atm.2016.05.43
32. Leong S, Kok HK, Govender P, Torreggiani W. Reducing risk of transjugular intrahepatic portosystemic shunt using ultrasound guided single needle pass. World J Gastroenterol. 2013;19(22):3528-3530. doi:10.3748/wjg.v19.i22.3528
33. Klinger C, Riecken B, Schmidt A, et al. Transjugular local thrombolysis with/without TIPS in patients with acute non-cirrhotic, non-malignant portal vein thrombosis. Dig Liver Dis. 2017;49(12):1345-1352. doi:10.1016/j.dld.2017.05.020
34. Loss M, Lang SA, Uller W, Wohlgemuth WA, Schlitt HJ. Combined surgical and interventional therapy of acute portal vein thrombosis without cirrhosis: a new effective hybrid approach for recanalization of the portal venous system. J Am Coll Surg. 2014;218(3):e79-86. doi:10.1016/j.jamcollsurg.2013.11.010
