



Investigating Nurses' Self-Efficacy in Pressure Injury Management Within Surgical Services
© 2024 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Wound Management & Prevention or HMP Global, their employees, and affiliates.
Abstract
Background: New research is crucial in addressing the role of nurses in preventing pressure injuries (PIs) and remedying deficiencies in their self-efficacy in this area. Purpose: The aim of this study was to examine the self-efficacy perceptions of nurses in managing PIs within surgical services. Methods: The study involved 186 nurses from surgical services. Data were collected using a self-efficacy scale and a personal information form designed to assess nurses' PI management skills. Analysis involved descriptive (number, percentile) and inferential statistics (ANOVA, t- s) in SPSS-24. Results: Surgical nurses reported their self-efficacy in managing PIs with a mean score of 47.38 ± 21.87 on a self-efficacy scale, indicating a broad range of perceptions. Average scores were 43.55 ± 23.47 for evaluation, 48.39 ± 25.65 for planning, 43.68 ± 25.34 for surveillance, and 50.64 ± 22.23 for decision-making. Of note, nurses reported the lowest self-efficacy scores for evaluation. No significant differences were found based on employment duration, gender, or education. Significant differences were observed based on age, service level, and post-graduate education (P < .05). Conclusion: This study highlights the need for enhanced nurse self-efficacy in PI management in surgical services, emphasizing the role of education programs focused on evaluation skills.
Introduction
Pressure injuries (PIs) represent a significant and challenging aspect of healthcare delivery in surgical services. These injuries are a common and serious problem, especially among surgical patients, and the competencies of nurses in this area play a crucial role in the effectiveness of prevention and management strategies. In this context, nurses' self-efficacy in managing PIs can significantly impact patient outcomes. The European Pressure Ulcer Advisory Panel and the National Pressure Ulcer Advisory Panel (now the National Pressure Injury Advisory Panel) define PI as localized damage to the skin and/or subcutaneous tissue, typically caused by pressure exerted on bony prominences, either alone or in combination with shearing forces.1
The widespread prevalence and severity of PIs highlight the potential of nurses' self-efficacy for effectively preventing and managing PIs to improve patient outcomes. Data from the American National Pressure Ulcer Advisory Panel indicates that the incidence of PI ranges from 1% to 12% in acute care clinics, 3.3% to 53.4% in intensive care clinics, 1.9% to 59% in elderly care clinics, 0.25% to 27% in pediatric clinics, and 5% to 53.4% in surgical clinics.2,3,4 In Turkey, the incidence is reported to be 20.5% in surgical intensive care patients, 3.5% to 29.5% in clinical patients undergoing surgery, and approximately 35.3% in other intensive care units.3 PIs are most frequently observed in the sacrum and heels.5 Despite global education efforts, significant investments, and evidence-based practice guidelines, PIs remain a persistent health problem.2,3
The rate of pressure ulcer development in surgical patients increases due to a combination of factors. These include prolonged immobility during and after the surgical process, sensory loss, decreased blood circulation, excessive moisture and sweating, nutritional deficiencies, weakened immune system, and other health issues. Additional factors specific to surgery, such as the stress response to surgery and protein loss, further increase the risk and severity of pressure ulcers. Pre-operative conditions, effects of anesthesia, status of the wound, pain levels, complications such as infection or bleeding, challenges related to treatment, and prolonged immobility during and after surgery place surgical patients at a higher risk of developing pressure ulcers.6 In the intensive care unit, factors such as incontinence, wound discharge, and sweating can exacerbate this risk by causing skin irritation and moisture.7-9 PIs in surgical patients can lead to worsened outcomes, such as increased pain, higher hospital readmission rates, additional surgical interventions, extended hospital stays, possible deformities, significant increases in hospital costs, dissatisfaction with treatment and care, and decline in quality of life.10 The prevalence of PIs is considered an indicator of care quality in health care facilities. It is crucial that primary nurses maintain patient skin integrity and prevent complications, which requires up-to-date, evidence-based knowledge and skills in PI prevention in line with national and international guidelines.11,12,13
Numerous studies have examined nurses' levels of early identification, prevention, and management of PI, evaluating their knowledge and attitudes.14-17 These studies have reported varying results, indicating that nurses possess low,15,17-20 moderate,21,22 and high16,23,24 levels of knowledge regarding early identification, prevention, and management of PI.15-17,20-24 However, limited research has investigated the knowledge and attitudes of nurses working specifically in surgical services.22,25 None of the identified studies have comprehensively assessed the self-efficacy levels of nurses in surgical services pertaining to PI evaluation, planning, surveillance, and decision-making.21,23 It is crucial to note that the self-efficacy of nurses in surgical services significantly influences PI prevention, the provision of quality health care services, the healing process, and patient satisfaction.26,27
Developed by Dellafiore and colleagues in 2019 and later adapted to Turkish by Utli and Dinç, the Pressure Injury Management Self-Efficacy Scale is specifically designed to measure nurses' competencies in managing PIs. This scale comprehensively assesses nurses' self-efficacy perceptions in critical skills such as evaluation, planning, surveillance, and decision-making, making it an appropriate tool for this study focused on levels of self-efficacy and educational needs in PI management.12,26 This study aims to contribute valuable data on nurses' self-efficacy regarding PI, thereby informing the improvement of in-service and pre-graduate training programs on this subject.
Purpose
The aim of this study is to investigate the self-efficacy perceptions of nurses in managing PIs within surgical services.
Materials and Methods
Study Design: This was a cross-sectional study conducted in the surgical wards of the Van Training and Research Hospital Van Province in Turkey, from January 16, 2023, to March 11, 2023.
Surgical services and operations specialize in performing treatments through surgical incisions on patients, distinguishing them from other medical treatment units in this respect.
The research was conducted with nurses working in orthopedics, neurosurgery, urology, cardiovascular surgery, thoracic surgery, operating theaters, and the surgical intensive care unit of the hospital. Ethical approval was obtained before commencing the study (Approval no: 2023/4). Nurses were informed about the research, and their written consent was obtained.17 All stages of the research were conducted in accordance with the World Medical Association Declaration of Helsinki.15
Research Universe and Sampling
To determine the adequacy of the sample size for the study, a priori calculation was conducted using the G* Power program (Düsseldorf, Germany). The calculation utilized Cohen's (d) standard effect size table.16 With a 2-tailed hypothesis, an effect size of d=0.3, alpha error: 0.05, beta error: 0.20 (correction from the original beta error of 0.05 to match the power description), and power: 0.95, the minimum required sample size was determined to be (n=147). Considering potential data losses, it was decided to increase the sample size by 10%.
A total of 220 nurses working in the surgical departments of Van Training and Research Hospital were evaluated for eligibility and invited to participate in the study. Due to 23 nurses declining to volunteer and 11 nurses being unreachable for reasons such as being off duty or on leave, a total of 34 nurses were excluded from the sample. The analyses of the study were conducted with 186 nurses, reaching 84.54% of the target population.
Data Collection Tools
Two forms were used for data collection in the study. The first, a Personal Information Form, assessed nurses' socio-demographic characteristics, including age, gender, education level, the surgical ward they worked in, their tenure in that ward, and whether they had received training on PI management. The second form was the Pressure Injury Management Self-Efficacy Scale for Nurses. This scale, comprising 4 sub-scales and 10 items, focuses on evaluation, planning, surveillance, and decision-making. Items are rated on a scale from 1 (not at all competent) to 5 (completely competent). Mean scores for sub-scales were calculated using specific formulas, with the total score range being 0-100. The scale's Cronbach's alpha reliability coefficient was reported as 0.838, indicating high internal consistency.11,28 In this study, the Cronbach's alpha value was calculated as 0.857.
Application of Data Collection Tools
Before starting the research, nurses were informed about the study. The briefing was conducted in person by the researcher, who visited the nurses in their units. Nurses were asked to sign informed consent forms if they were willing to participate in the study, taking note of their email and phone number for communication purposes. To prevent the nurses from influencing each other's responses, the survey questions were sent electronically outside of working hours. Before collecting the data, a pilot study was conducted with 10 nurses to evaluate the clarity of the data collection forms. Because no revisions were made to the data collection forms, the data from the pilot study were included in the research. To ensure the confidentiality of the data, a questionnaire form was created using the website survey.com. This form was shared with the nurses through online platforms such as email and WhatsApp groups. The nurses were instructed to fill out the form themselves. It took approximately 10 to 15 minutes for the nurses to complete the survey questions.
Statistical Analysis of the Data
The statistical analysis of the data was conducted using SPSS 24.0 (IBM Inc, Canada) for Windows. For descriptive statistics, the number (n) and percentage (%) value were used to display categorical variables and mean ± standard deviation was used for numerical values. The normality of data distribution was assessed with the Kolmogorov-Smirnov and Shapiro-Wilk tests. Parametric tests were used as the data was normally distributed. The dependent variable of the study was nurses' self-efficacy in PI management, and the independent variables were nurses' age, gender, education level, and experience duration in nursing and surgical services. The dependent and independent variables were statistically compared. The independent samples t-test was used for comparing 2 groups, and the 1-way ANOVA test was used for comparing 3 or more groups. In the ANOVA test, Tukey HSD post hoc analysıs was used to identify the group responsible for the difference. A P value < .05 was considered statistically significant.
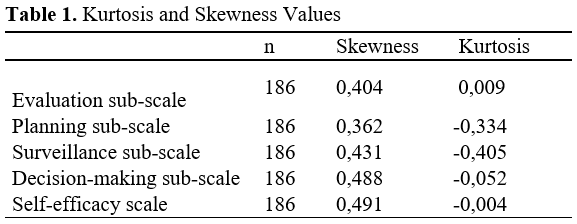
In the study, scale scores were calculated and kurtosis and skewness coefficients were examined to determine the suitability of the scores for a normal distribution. It is considered sufficient for a normal distribution if the kurtosis and skewness values obtained from the scales fall between +3 and -3.
Upon examining the values, it was observed that the kurtosis and skewness coefficients for each score were between -3 and +3. Based on this result, it was concluded that the scores followed a normal distribution. Due to this, parametric test techniques were employed in the study. To analyze whether scale scores differed according to demographic characteristics, t-tests and ANOVA tests were used. The t-test was utilized for analyzing demographic variables with 2 groups, while the ANOVA test was employed for variables with k (k>2) groups (Table 1).
Results
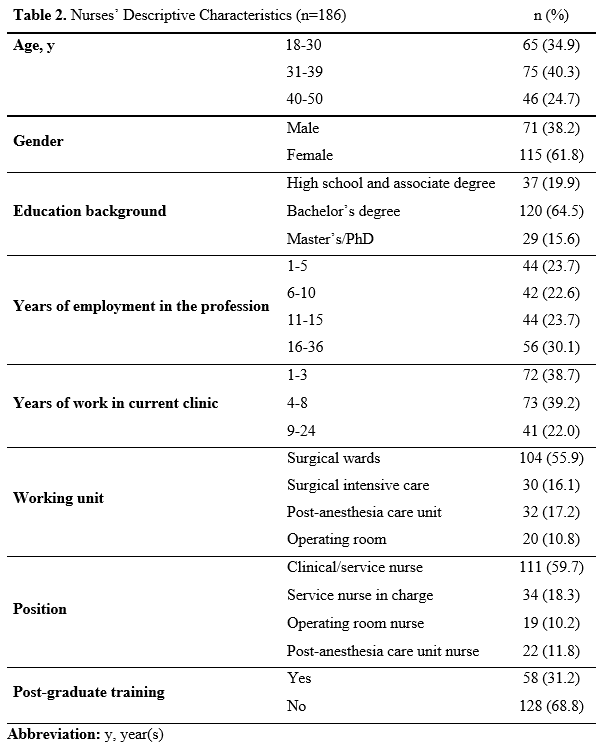
Table 2 displays the descriptive characteristics of the participating nurses. In the study, 40.3% of the nurses belonged to the 31-39 age group and 61.8% were female. Additionally, 64.5% of the nurses held a bachelor's degree, and the majority (59.7%) were employed as surgical nurses. Regarding professional experience, 30.1% of the nurses reported practicing nursing for 16-36 years, and 39.2% had worked in their respective clinics for 4-8 years. Interestingly, 68.8% of the nurses stated that they had not received any postgraduate training or courses specifically related to PI (Table 2).
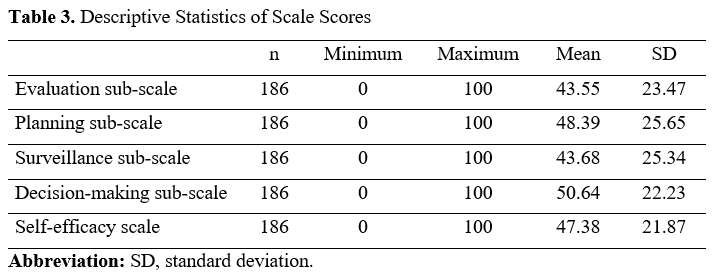
The evaluation sub-scale had a mean score of 43.55 ± 23.47, the planning sub-scale had a mean score of 48.39 ± 25.65, and the surveillance sub-scale had a mean score of 43.68 ± 25.34. The nurses' decision-making sub-scale had a mean score of 50.64 ± 22.23. Lastly, the overall mean score for the entire scale was calculated as 47.38 ± 21.87 (Table 3).
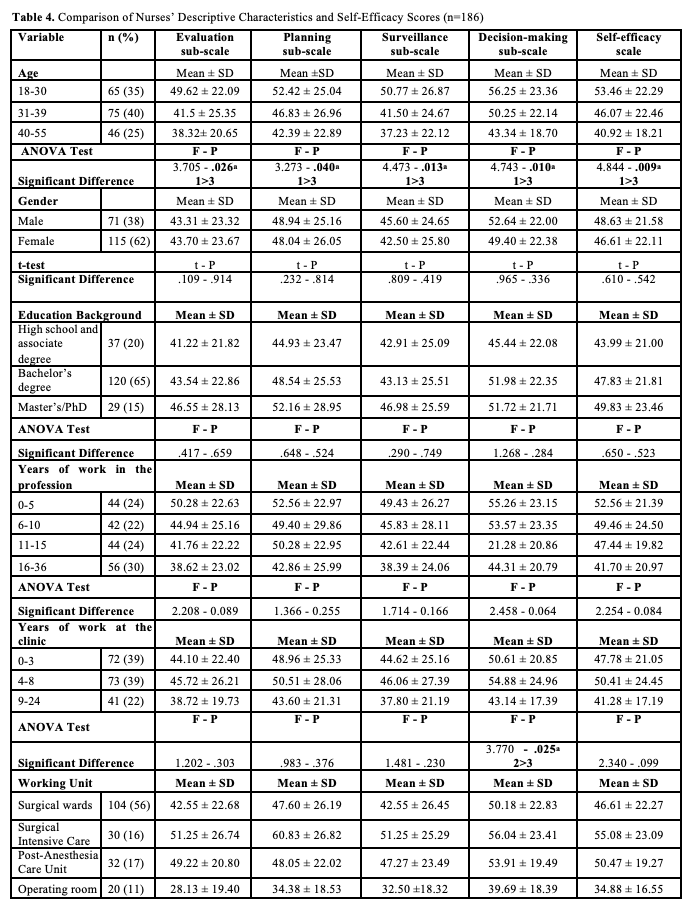
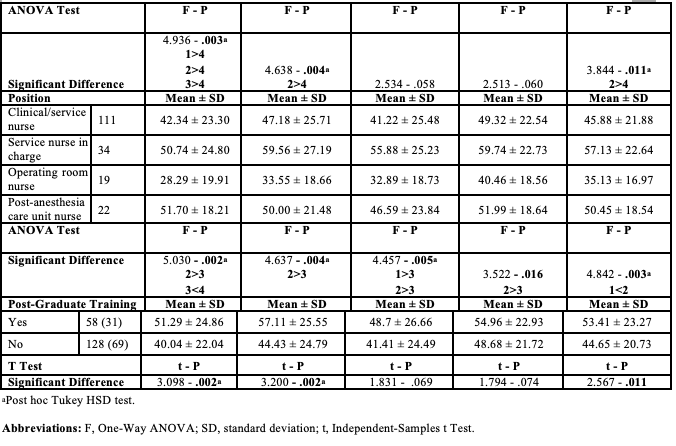
After conducting an analysis of the responses from surgical nurses across the evaluation, planning, surveillance, decision-making, and self-efficacy sub-scales, significant variations were observed. Age was found to be a contributing factor, with nurses between the ages of 18-30 exhibiting higher scores compared to other age groups (P < .05). However, no significant differences were observed in relation to education level, gender, or years of experience. In terms of years of experience in the clinic, nurses with 1-3 years of experience had higher decision-making scores compared to other groups (P < .05). Significant differences were found in the evaluation, planning, and self-efficacy scores were found based on the department in which nurses were employed. Nurses working in surgical intensive care services demonstrated significantly higher scores compared to other groups (P < .05). Furthermore, nurses in charge of the service displayed higher scores across the evaluation, planning, surveillance, decision-making, and self-efficacy scales, indicating their increased levels of responsibility (P < .05). Lastly, participants who underwent postgraduate training or courses specifically focused on PI had higher scores in the evaluation, planning, and self-efficacy scales compared to other groups (P < .05) (Table 4).
Discussion
This study revealed that the self-efficacy levels of surgical nurses in managing PIs are generally low, which aligns with some findings and contradicts others in the current literature. Notably, younger nurses and those working in intensive care units exhibited higher self-efficacy perceptions, highlighting the importance of current education and the experience gained in specialized areas such as intensive care. Furthermore, nurses who received postgraduate education had higher self-efficacy scores, emphasizing the importance of professional development and continuous education. These core findings underscore the necessity of supporting nurses' education and professional growth in PI management and provide valuable insights into the need for strengthening educational programs in this area.
The study results also explored surgical nurses' self-efficacy perceptions in managing PIs across various sub-scales. While scores across each sub-scale exhibited a wide distribution, the lowest average scores were found in the evaluation domain and the highest in decision-making. This indicates that nurses feel more competent in making decisions, but less confident in their evaluation skills. Surgical nurses reported low self-efficacy levels concerning the management of PIs. This outcome is consistent with the findings of previous studies by Akese et al20 and Iranmanesh et al27, which highlighted high self-efficacy levels among nurses in identifying, classifying, and preventing PIs. On the other hand, Celik et al23 have documented that nurses' self-efficacy in the prevention and management of PIs was moderate. Contrarily, research conducted by Başayar and Yazıcı18, and Ünlü and Andsoy21, reported a deficiency in nurses' self-efficacy in terms of defining, staging, preventing, and managing PIs.
The present study observed that, in surgical clinics, nurses aged 18 to 30 years scored significantly higher on scales measuring evaluation, planning, surveillance, and decision-making capabilities compared to nurses from other age groups. The reason why younger nurses report higher self-efficacy scores compared to older nurses might be due to more current education and knowledge, innovative aspects of training, adaptability and flexibility, professional ideals, and motivation. However, age could also be a confounding factor in this context. The authors of this study believe that implementing continuous and in-service training programs for nurses, as well as conducting studies with a larger sample size, would be beneficial in further understanding this issue.
This observation is consistent with the findings of Tirgari et al28 and Ebi et al29, who reported that age did not significantly influence nurses' self-efficacy scores in the context of PI prevention. Similarly, studies by Kaddourah et al30 and Başayar and Yazıcı18 revealed that nurses under the age of 30 had significantly higher self-efficacy scores related to PI risk factors compared to those aged 41 and older. This difference may be explained by the fact that newly graduated nurses retain the knowledge gained during their education and are likely to be more current with the latest information and practices.
This study identified no significant differences in the level of knowledge regarding PI among surgical nurses when considering education level, gender, and years of professional experience. This aligns with the outcomes reported by Tubaishat et al31 and Sarı32, who observed no notable variance in nurses' self-efficacy levels concerning PI prevention across different educational backgrounds. In a similar vein, Ünlü and Andsoy21 also found no significant distinctions in knowledge about PI prevention, risk assessment, staging, and wound identification among surgical nurses based on their educational achievements. Contrarily, Saleh et al33 and Ebi et al29 highlighted that nurses holding associate degrees reported significantly lower self-efficacy scores related to PI risk factors and prevention measures in comparison to those with bachelor's and advanced degrees. Meanwhile, Aydın et al3 and Lawrence et al17 reported no significant linkage between educational levels and self-efficacy scores in PI management. In terms of gender differences, the present research findings echo those of Keser and Yüksel19, who detected no significant disparity in self-efficacy concerning PI between male and female nurses. However, Başayar and Yazıcı18 found that female nurses had significantly higher total self-efficacy scores for PI than their male counterparts. As for professional experience, the results reported here are in line with those of Celik et al23, indicating that length of professional experience does not significantly influence nurses' self-efficacy. Yet, Saleh et al33 observed a significant correlation between the extent of working experience and self-efficacy levels in PI management. It is therefore important to acknowledge that available literature presents diverse findings regarding the effects of education level, gender, and professional experience on self-efficacy in PI management.
In the present study, the scores for evaluation, planning, and self-efficacy scales differed among nurses based on their working department. Notably, nurses employed in the intensive care unit (ICU) displayed statistically higher average scores than those in surgical clinics (Table 4). This result mirrors the findings of Ünlü and Andsoy21, who reported significantly elevated mean scores in PI prevention, risk assessment, and wound identification among ICU nurses in comparison to their counterparts in surgical clinics. This observation is also supported by the broader literature, which suggests that ICU nurses often exhibit higher self-efficacy levels than nurses working in other specialties. Studies by Aydın et al,3 Iranmanesh et al,27 and Alsharari et al34 have similarly concluded that ICU nurses possess greater self-efficacy levels than those in different clinical environments. Such findings might be explained by the prevalence of PIs in ICUs, where patients are frequently hospitalized for prolonged durations.2,9,35 Therefore, the present study's insights align with existing scholarly work.
Additionally, the research presented here shows that nurses overseeing services scored significantly higher on evaluation, planning, surveillance, decision-making, and self-efficacy scales compared to nurses with other roles in terms of their duties and working style. This aligns with the study conducted by Keser and Yüksel19, which also identified a higher level of self-efficacy in managing PIs among service nurses versus their peers. This difference in knowledge and self-efficacy levels could be attributed to service-leading nurses having amassed considerable experience by working in the same health care setting for a lengthy period.
In the present study, a correlation was found between nurses who had completed postgraduate education courses and higher scores in evaluation, planning, and self-efficacy scales. This result is in line with the findings of Başayar and Yazıcı18, which demonstrated that nurses with training on PI management achieved significantly higher scores in interventions for PI prevention, staging, and overall self-efficacy. Additional studies in the field have indicated that nurses who receive specific training on PI management tend to show significantly improved self-efficacy levels.1,24,26,29 This improvement is likely attributable to training programs granting nurses access to the latest information, thus broadening their understanding and skills in the prevention and management of PIs.
Limitations
This study's limitations include its cross-sectional design, which restricts the ability to draw causal inferences between nurses' reported self-efficacy and their management of PIs. The findings are based on self-reported data from a single hospital's surgical services, potentially limiting generalizability to other settings or regions. The study's sample size was insufficient for conducting regression analysis to control for confounding factors, constituting a limitation of the research. Additionally, the potential for response bias in self-reported measures might affect the accuracy of the findings. The impact of external factors such as staffing levels, organizational support, and the quality of previous training on PI management was not explored, which could significantly influence the outcomes. Future research could benefit from addressing these limitations to provide more comprehensive insights.
Conclusion
Research conducted on nurses' self-efficacy in managing PIs within surgical services has revealed critical insights into the current state of nursing practices and areas for improvement. Despite the important role nurses play in preventing and managing PIs, the present study identified an overall low level of self-efficacy among surgical nurses in this regard. The findings underscore the necessity of targeted educational and training programs, especially in evaluation skills, to enhance nurses' confidence and capabilities in managing PIs effectively. Additionally, the study highlights the influence of factors such as age, service level, and post-graduate education on nurses' self-efficacy, suggesting that tailored interventions considering these variables could further optimize outcomes. Ultimately, improving nurses' self-efficacy in PI management is pivotal not only for elevating patient care quality but also for advancing health care outcomes within surgical services.
Acknowledgments
Authors: Orhan Polat, RN, PhD1; Ayla Yava, RN, PhD2; Aynur Koyuncu, RN, PhD2; and Remzi Karasungur, RN, PhD3
Affiliations: 1Gaziantep Islamic Science and Technology University, the Vocational School of Higher Education for Health Services, Gaziantep, Turkey; 2Hasan Kalyoncu University, Health Sciences Faculty, Department of Nursing, Gaziantep, Turkey; 3Baykan State Hospital, Faculty of Health Sciences, Siirt, Turkey
Disclosures: The authors have no financial or other conflicts of interest to disclose.
Correspondence: Orhan Polat; Gaziantep Islamic Science and Technology University, the Vocational School of Higher Education for Health Services, Beştepe 104001 Cd. 27260, Gaziantep, Turkey; orhan_m56@hotmail.com
ORCID: Polat, 0000-0002-5180-1866; Yava, 0000-0003-3468-6779; Koyuncu, 0000-0003-3486-458X; Karasungur, 0000-0002-8015-0644
References
1. Nassehi A, Jafari M, Rashvand F, Rafiei H, Hosseinpour F, Shamekhi L. Intensive care unit, cardiac care unit, and emergency department nurses' perceptions of medical device-related pressure injuries: a cross-sectional study. Wound Manag Prev. 2022;68(9):24-28.
2. European Pressure Ulcer Advisory Panel, National Pressure Injury Advisory Panel and Pan Pacific Pressure Injury Alliance. In: Emily H, ed. Prevention and Treatment of Pressure Ulcers/Injuries: Clinical Practice Guideline. The International Guideline. EPUAP/NPIAP/PPPIA;2019. https://www.partnersinprevention.com/npiap-clinical-guideline
3. Aydın AK, Karadağ A, Gül Ş, Avşar P, Baykara ZG. Nurses' knaowledge and practices related to pressure injury: a cross-sectional study. J Wound Ostomy Continence Nurs. 2019;46(2):117-123. doi:10.1097/WON.0000000000000517
4. Prevention and Treatment of Pressure Ulcers/Injuries: Clinical Practice Guideline 2019. National Pressure Injury Advisory Panel. https://internationalguideline.com/2019
5. Li Z, Lin F, Thalib L, Chaboyer W. Global prevalence and incidence of pressure injuries in hospitalised adult patients: a systematic review and meta-analysis.Int J Nurs Stud. 2020;105:103546. doi:10.1016/j.ijnurstu.2020.103546
6. Kaşıkçı M, Aksoy M, Ay E. Investigation of the prevalence of pressure ulcers and patient-related risk factors in hospitals in the province of Erzurum: a cross-sectional study. J Tissue Viability. 2018;27(3):135-140. doi:10.1016/j.jtv.2018.05.001
7. de Assis IIC, Estevam Dos Santos J, Valadares Sinicio Abib ML, et al. Medical device-related pressure injury in an intensive care unit: a cross-sectional study. Wound Manag Prev. 2021;67(11):26-32.
8. Çetiner M, Akkaya Arı S, Eşkut N, Ocak Ö, Canbaz Kabay S, Özışık Karaman HI. Evaluation of clinical features and the factors related to nutrition in home care patients with pressure ulcer. Fam Pract Palliat Care. 2021;6(1):7-12. doi:10.22391/fppc.776139
9. Karaca Sivrikaya S, Sarıkaya S. Compression management, prevention and care in intensive care patients. Article in Turkish. Journal of Intensive Care Nursing. 2020;24(2):139-149.
10. Kıraner E, Terzi B, Uzun Ekinci A. Tunalı B. Determination of pressure ulcer incidence and risk factors in our intensive care unit. Article in Turkish. Journal of Intensive Care Nursing. 2016;20(2):78-83.
11. Wang I, Walker R, Gillespie BM. Pressure injury prevention in the perioperative setting: an integrative review integrative review. J Perioper Nurs. 2018;31(4):27-35. doi:10.26550/2209-1092.1049
12. Dellafiore F, Arrigoni C, Ghizzardi G, et al. Development and validation of the pressure ulcer management self-efficacy scale for nurses. J Clin Nurs. 2019;28(17-18):3177-3188. doi: 10.1111/jocn.14875
13. Fulbrook P, Lawrence P, Miles S. Australian nurses' knowledge of pressure injury prevention and management: a cross-sectional survey. J Wound Ostomy Continence Nurs. 2019;46(2):106-112. doi:10.1097/WON.000000000000050
14. Emanuel EJ, Wendler D, Killen J, Grady, C. What makes clinic research in developing countries ethical? The bench marks of ethical research. J Infect Dis. 2004;189(5):930-937. doi:10.1086/381709
15. World Medical Association Declaration of Helsinki 2008. Accessed September 9, 2024. https://www.wma.net/what-we-do/medical-ethics/declaration-of-helsinki/doh-oct2008/
16. Cohen J. Statistical power analysis. Curr Dir Psychol Sci. 1992;1(3):98-101. doi:10.1111/1467-8721.ep10768783
17. Lawrence P, Fulbrook P, Miles S. A survey of Australian nurses' knowledge of pressure injury/pressure ulcer management. J Wound Ostomy Continence Nurs. 2015;42(5):450-460. doi:10.1097/WON.0000000000000141
18. Başayar Z, Yazıcı G. Determination of knowledge levels of nurses working in surgical clinics on preventing pressure injuries. Journal of Hacettepe University Faculty of Nursing. 2022;9(2):216-224. doi:10.31125/hunhemsire.1167340
19. Keser E, Yüksel S. Knowledge and attitudes of surgical nurses towards pressure ulcer prevention. Selcuk Medical Journal. 2020;36(3):216-225. doi:10.30733/std.2020.01384
20. Akese MI, Adejumo PO, Ilesanmi RE, Obilor HN. Assessment of nurses' knowledge on evidence-based preventive practices for pressure ulcer risk reduction in patients with impaired mobility. Afr J Med Med Sci. 2014;43(3):251-258
21. Ünlü AA, Andsoy II. Examination of surgical nurses' information on pressure injury, risk factors, and prevention. Journal of General Medicine. 2021;31(2):168-174. doi:10.15321/GenelTipDer.2021.307
22. Tallier PC, Reineke PR, Asadoorian K, Choonoo JG, Campo M, Malmgreen-Wallen C. Perioperative registered nurses knowledge, attitudes, behaviors, and barriers regarding pressure ulcer prevention in perioperative patients. Appl Nurs Res. 2017;36:106-110. doi:10.1016/j.apnr.2017.06.009
23. Çelik S, Dirimeşe E, Taşdemir N, et al. Pressure sore prevention and treatment knowledge of nurses. Med J Bakirkoy. 2017;13(3):133-139. doi:10.5350/BTDMJB201713305
24. Ünver S, Fındık ÜY, Özkan ZK, Sürücü Ç. Attitudes of surgical nurses towards pressure ulcer prevention. J Tissue Viability. 2017;26(4):277-281. doi:10.1016/j.jtv.2017.09.001
25. Nuru N, Zewdu F, Amsalu S, Mehretie Y. Knowledge and practice of nurses towards prevention of pressure ulcer and associated factors in Gondar University Hospital, Northwest Ethiopia. BMC Nurs. 2015;14:34. doi:10.1186/s12912-015-0076-8
26. Utli H, Dinç M. Turkish validity and reliability study of Pressure Injury Management Self-Efficacy Scale for Nurses. Article in Turkish. Journal of İnönü University Vocational School of Health Services. 2022;10(3):948-964. doi:10.33715/inonusaglik.1063082
27. Iranmanesh S, Tafti AA, Rafiei H, Dehghan M, Razban F. Orthopaedic nurses' knowledge about pressure ulcers in Iran: a cross-sectional study. J Wound Care. 2013;22(3):138-40, 142-143. doi: 10.12968/jowc.2013.22.3.138
28. Tirgari B, Mirshekari L, Forouzi MA. Pressure injury prevention: knowledge and attitudes of Iranian intensive care nurses. Adv Skin Wound Care 2018;31(4):1-8. doi: 10.1097/01.ASW.0000530848.50085.ef
29. Ebi WE, Hirko GF, Mijena DA. Nurses' knowledge to pressure ulcer prevention in public hospitals in Wollega: a cross-sectional study design. BMC Nurs. 2019;18:20. doi: 10.1186/s12912-019-0346-y
30. Kaddourah B, Abu-Shaheen AK, Al-Tannir M. Knowledge and attitudes of health professionals towards pressure ulcers at a rehabilitation hospital: a cross-sectional study. BMC Nurs. 2016;15(1):17. doi:10.1186/s12912-016-0138-6
31. Tubaishat A, Aljezawi M, Al Qadire M. Nurses' attitudes and perceived barriers to pressure ulcer prevention in Jordan. J Wound Care. 2013;22(9):490-497. doi:10.12968/jowc.2013.22.9.490
32. Sarı E. Knowledge levels of intensive care nurses about pressure ulcers. Akkadian Geriatrics. 2013;5(1):73-79. doi:10.5350/BTDMJB201713305
33. Saleh YN, Al-Hussami M, Anthay DM. Pressure ulcer prevention and treatment knowledge of Jordanian nurses. J Tissue Viability. 2013;22(1):1-11. doi:10.1016/j.jtv.2013.01.003
34. Alsharari FA, Khadam QA, Albagawi BS, Alotaibi JS, Alqahtani ME. Nurses' knowledge, attitudes and beliefs toward pressure ulcers prevention. Aljouf University Medical Journal. 2017;4(3):21-28. doi:10.12816/0060140
35. Tanrıkulu F, Dikmen Y, Tanrıkulu F. Pressure sores in intensive care patients: risk factors and precautions. Journal of Human Rhythm. 2017;3(4):177-182.
