



Nursing Practices for a Patient With ALK-Negative Anaplastic Large Cell Lymphoma With a Cancerous Wound: A Case Report
© 2024 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Wound Management & Prevention or HMP Global, their employees, and affiliates.
Abstract
Background: Cancerous wounds are a significant challenge in cancer care, reducing the quality of life and affecting psychological well-being. PURPOSE: This case report describes a 59-year-old female who developed a severe cancerous wound. The report presents comprehensive nursing measures for patients with cancerous wounds and discusses key nursing factors that promote wound healing. CASE STUDY: The patient, diagnosed with stage Ⅲ B ALK-negative anaplastic large cell lymphoma, developed a severe cancerous wound. Specialist nurses developed a detailed wound care plan during 2 inpatient chemotherapy sessions, including wound care, pain management, nutrition support, psychosocial support, and continued transitional care after discharge. Her wound decreased in size and eventually healed. CONCLUSION: Implementing nursing measures for patients with cancerous wounds—including assessment of systemic and local wounds, wound care, pain management, nutrition support, psychosocial support, health education, and transitional care—can help manage wounds and lead to complete healing. Specialized nurses play a key role in treating severe wounds. This case highlights the need for comprehensive and scientific nursing practices for patients with cancerous wounds. It conveys a positive attitude towards treatment and a sense of responsibility among nurses.
Introduction
Anaplastic large cell lymphoma (ALCL) is a rare and aggressive type of T-cell lymphoma, accounting for approximately 2% of all adult non-Hodgkin lymphomas.1 It typically affects lymph nodes, skin, and soft tissue.1,2 There 2 types of ALCL are ALK-positive and ALK-negative. ALK-positive ALCL is more common in children and young adults, while ALK-negative ALCL tends to occur in older adults and has a poorer prognosis.3-5 The treatment for ALCL is chemotherapy, though stem cell transplantation can be performed for individuals with severe or relapsed ALCL.1 Patients with ALCL may develop cancerous wounds due to intensive treatment regimens or disease progression.6 Cancerous wounds impair skin function, leading to local bleeding, exudation, and malodor, making them difficult to heal.2 They are a significant complication faced by patients with cancer and often lead to pain and reduced quality of life.2,7 The management and treatment of these wounds pose significant challenges to health care providers, requiring personalized and comprehensive intervention measures to promote wound healing, alleviate pain, and prevent complications.8
In this article, the authors describe the wound management of a patient with ALK-negative anaplastic large cell lymphoma who presented with a severe cancerous wound during treatment. The authors aim to summarize the nursing experience and establish evidence-based practice standards for cancerous wound management in patients with malignant tumors in nursing units.
Case Report
A 59-year-old female was admitted to the authors’ hospital with a large ulcerated mass in the right groin that had been present for more than 3 months. After extensive examination—including pathological examination, bone marrow puncture, and PET-CT scan—the patient was diagnosed with ALK-negative anaplastic large cell lymphoma. She was subsequently hospitalized and started receiving chemotherapy with the CHOP regimen (cyclophosphamide 750 mg/m2, doxorubicin 75 mg/m2, vincristine 2 mg/m2, and prednisone 100 mg). Upon admission, the patient was pushed into the ward in a wheelchair by her husband, with the wound on the right thigh wrapped in gauze. After removing the gauze, the ulcerated wound was oval-shaped, significantly necrotic with yellow purulent secretions, and malodorous. The patient reported that the wound had not undergone any medical intervention since its onset. The charge nurse and wound specialist nurse conducted a comprehensive assessment of the patient’s systemic and local wounds. Informed consent was obtained from the patient and her family for the publication of this case report and the associated images.
A systemic body assessment includes disease condition, nutritional status, self-care ability, fall risks, pressure ulcers, deep vein thrombosis, pain, and psychological condition. Except for malignant tumors, the patient had no other diseases that may affect wound healing. However, chemotherapy may lead to immune system dysfunction and damage to normal tissues, increasing the risk of wound infection and delaying healing. Chemotherapy-related side effects such as gastrointestinal reactions, hair loss, and rashes can also affect a patient’s nutritional status, which in turn affects wound healing. The patient was 160 cm tall, weighed 50 kg, with a BMI of 19.5. Since the onset of treatment, the patient had maintained a good appetite and was capable of independent eating and meeting her nutritional requirements. No significant weight loss had occurred and the patient had an NRS-2002 score of 1 point, indicating no current nutritional risk. Due to the large cancerous wound in a special location, the patient required partial assistance with dressing, relieving herself, and bed-to-chair transfers. Walking on flat ground and stairs required significant help or complete reliance on others. The Barthel Index total score was 55 points, indicating severe self-care dependency. The patient was mostly bedridden and occasionally experienced sweating, and she had severely limited mobility, with activities restricted to a chair. The existence of shear forces and friction was noted, as indicated by a Braden score of 14, suggesting a moderate risk of pressure ulcers. The patient had multiple diagnoses, required assistive devices for working, received intravenous fluids, exhibited an unbalanced gait, and had a Morse Fall Scale risk assessment score of 60, indicating a high fall risk. The patient was diagnosed with malignant tumors.
A peripherally inserted central catheter (PICC) was inserted into the right upper limb, which had a Caprini risk assessment score of 5 points, indicating a high risk of venous thromboembolism. Using a numeric rating scale, the patient rated her pain as mild at 2 points, which does not affect normal rest. The pain was evaluated once daily by the charge nurse, and the patient was instructed to inform medical staff if the pain intensified. Using the Distress Thermometer, the patient reported her psychological distress level over the past week, rating her current distress on a scale of 0 to 10 in which a score of 5 points indicated moderate psychological distress. The reasons for the patient’s distress included concerns about the appearance of the wound and her personal appearance; bathing and dressing; limited physical activity; nausea; fatigue; interaction with partners, family or friends; and worry. Except for pain evaluation, the charge nurse reviewed the above assessments weekly during the patient's hospitalization and at any point when changes occurred.
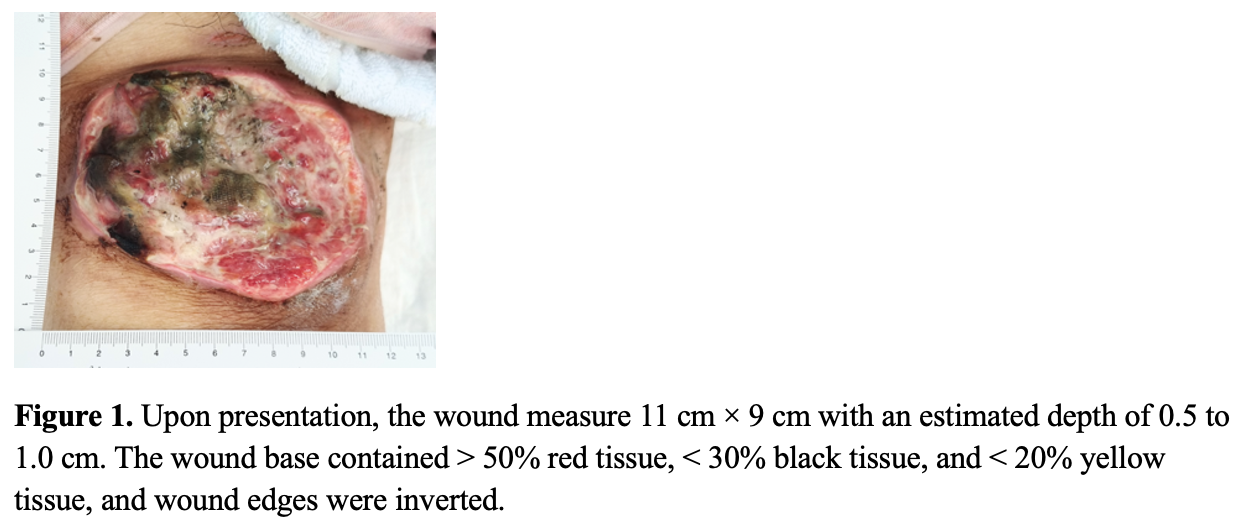
The wound specialist nurse assessed the wound, which was located on the right groin, 2 cm to 3 cm away from the perineum. This area is frequently active and requires a restriction of the patient's mobility or the use of support to protect the wound during the healing process. The lymph nodes and blood vessels in this area are dense, and they are often affected by various factors such as friction, sweat, and bacteria, thus having a higher risk of infection. The wound was oval-shaped, and when measured with a disposable wound ruler presented with a measurement of 11 cm × 9 cm. The depth was estimated to be 0.5 cm to 1.0 cm. The wound base contained > 50% red tissue, < 30% black tissue, and < 20% yellow tissue, and the wound edge was inverted (Figure 1). The surface of the wound was moist, and the exudate was a yellow medium-viscosity purulent secretion. The odor of the wound could be smelled at a distance of one arm’s length from the patient. The patient did not present with a fever. The wound surface secretion was collected for bacterial culture and drug sensitivity tests, and Pseudomonas aeruginosa, Proteus mirabilis, Enterobacter cloacae, and Klebsiella pneumoniae were detected.
Based on the above assessment, the patient’s care issues included impaired skin integrity, psychological distress, risk of nutritional disorders, and activity intolerance. The charge nurse developed a care plan for the patient, which was completed in collaboration with the charge nurse, wound specialist nurse, clinical dietitian, and psychiatric specialist nurse. The following measures were taken, all of which were started on the second day of the patient’s hospitalization and continued until the patient was discharged.
Routine nursing measures
The ward was ventilated twice a day and disinfected with UV lights once a day to reduce the risk of bacterial cross-infection. Caregivers assisted with helping the patient bathe daily, providing clean clothes and bed linens, and keeping the skin clean and dry.
Position and activity
The patient was instructed to use support pillows to stabilize her body, elevate the right leg as frequently as possible, change positions at least once every 2 hours, and position soft pillows between her knees when lying on her side to reduce pressure on the wound. The patient was also instructed to pull up the bed rails on both sides when turning and moving in bed, place the bedside bell within reach, and request the assistance of caregivers or nurses when getting out of bed.
Nutrition support
A clinical dietitian was invited for a consultation, and the dietitian formulated 3 meals a day that were high in calories, protein, and vitamins, and easy to digest, which were delivered by the hospital’s canteen. The patient was also instructed to drink more water and avoid spicy snacks, cigarettes, and alcohol.
Pain management
The responsible nurse conducted a pain assessment once a day and notified the physician of drug intervention promptly when the pain worsened or outbreaks of pain occurred. The patient’s pain medication was administered on time, and the nurse watched to ensure it was taken orally.
Psychological care
The responsible nurse actively communicated with the patient, answered her questions, and provided her with effective medical information. The nurse was instructed to empathize with the patient and encourage her to cope positively. The psychological specialist nurse provided cognitive behavioral therapy, coached her in relaxation and positive thinking, and relieved the patient’s worries.
Wound care
Wound care was provided by the wound specialist nurse. The first priority was infection control and the removal of necrotic tissue. The following measures were taken.
Removal of necrotic tissue
On the first day of hospitalization, chlorhexidine was used to clean the periwound skin. After cleaning the wound with saline, necrotic or inactivated tissue was gently debrided with sterile scissors by the surgeon, who assessed the patient’s pain throughout the process; 1% lidocaine was used to avoid any pain or bleeding.
Wound cleaning and protection
Debridement gel was evenly applied to the wound base. The debridement gel hydrates necrotic tissue, releases proteolytic enzymes to dissolve necrotic tissue, maintains a moist wound environment, forms a protective film on the wound surface, and promotes granulation tissue.
Control of inflammation and infection
As wound exudate increased, alginate was applied to cover the wound on top of the hydrogel, as alginate dressing can absorb 17 to 25 times its weight of exudate and form a gel-like wound mass inside the wound after absorbing exudate, providing a moist healing environment. Sterile gauze was used to cover the wound surface for protection. Wound assessment and dressing changes were performed once daily by the wound specialist nurse during hospitalization.
Health education
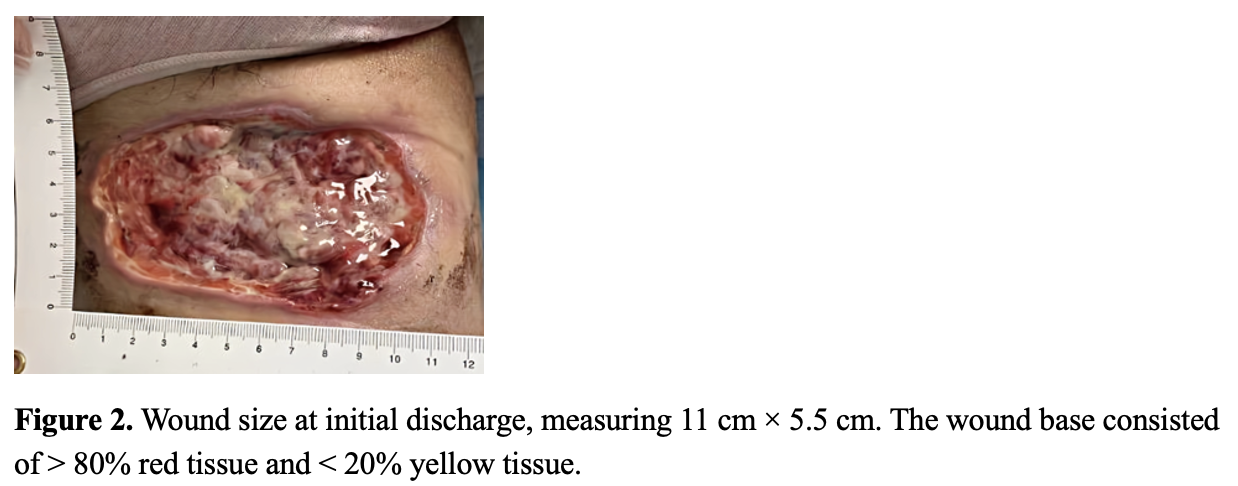
The charge nurse informed the patient and family of the purpose and meaning of each nursing measure during hospitalization and encouraged continued practice after discharge. The wound specialist nurse introduced the role of the drugs and dressings used to the patient and family members and encouraged family members to be present at each wound dressing change to learn the process. Before discharge, the charge nurse verified the effectiveness of health education by having the patient and family members demonstrate the care techniques and determined the patient’s care needs to develop a post-discharge care plan. After communication, the patient and her family consistently agreed that wound dressing changes after discharge were the most worrisome issue. Concerns about wound care included the inability to remember the wound dressing change process and the lack of knowledge of the names and where to purchase the items needed for dressing changes. In addition, there were also problems such as not knowing how to deal with changes in condition and how to be admitted to the hospital next time. In response to the patient’s wound care needs, the authors provided a paper list of items needed for wound dressing changes and how to purchase them, as well as a standardized instructional video on dressing changes. To address the problems of not knowing how to handle changes in the patient’s condition and how to be admitted to the hospital next time, the charge nurse established a transitional care WeChat group through the WeChat platform, which the patient could use to communicate with medical staff remotely by video, voice, or text. Members of the WeChat group included a charge nurse, who was responsible for guiding the patient’s care during the home period; the attending physician, who provided guidance on medication and medical care; and a wound care specialist nurse, who was responsible for wound assessment and guidance on medication changes. Six days later, the patient’s first chemotherapy treatment was completed, and the wound size at discharge was 11 cm × 5.5 cm, with a wound base of > 80% red tissue, < 20% yellow tissue, and a moderate amount of exudate (Figure 2).
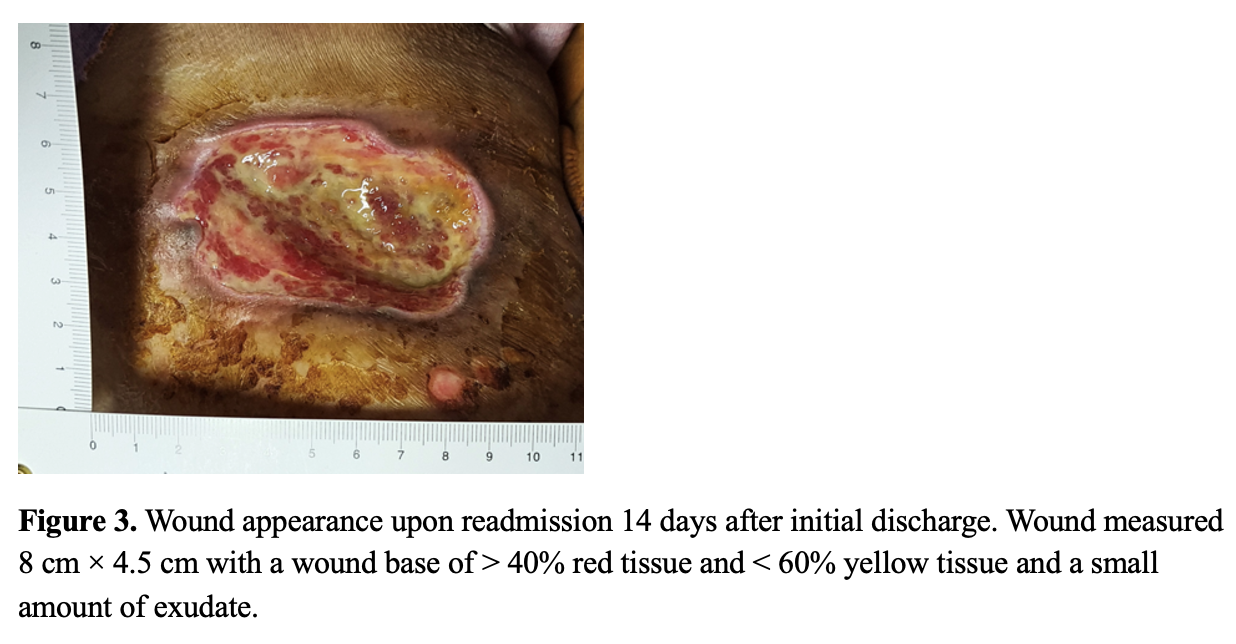
The patient was readmitted 14 days later with a wound measuring 8 cm × 4.5 cm and a base of > 40% red tissue and < 60% yellow tissue with a small amount of exudate (Figure 3). Wound care at this stage was aimed at filling tissue defects and promoting epithelialization of the wound edges. The wound care measures taken were as follows: the wound care nurse removed necrotic tissue, cleaned the wound with saline, and sprayed a silicon-based wound repair material on the wound base that promotes soft tissue angiogenesis and epithelialization.
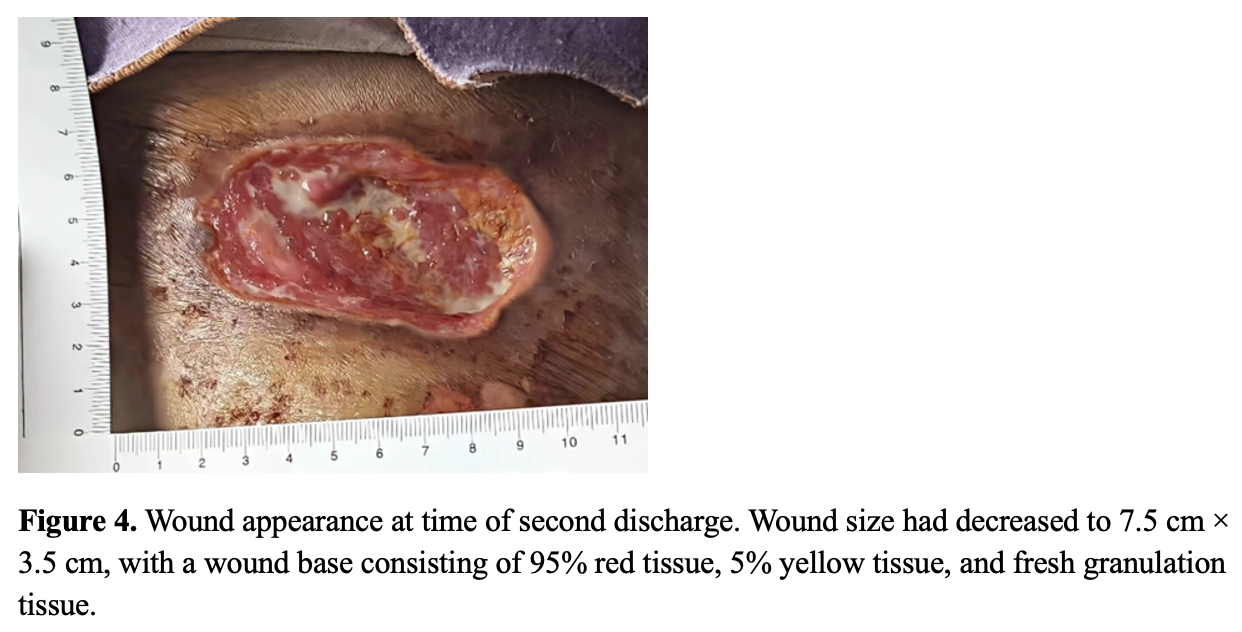
The patient was discharged again 3 days later, and the wound size had been reduced to 7.5 cm × 3.5 cm, and the wound base was 95% red tissue and 5% yellow tissue, with a small amount of exudate and fresh granulation tissue (Figure 4).
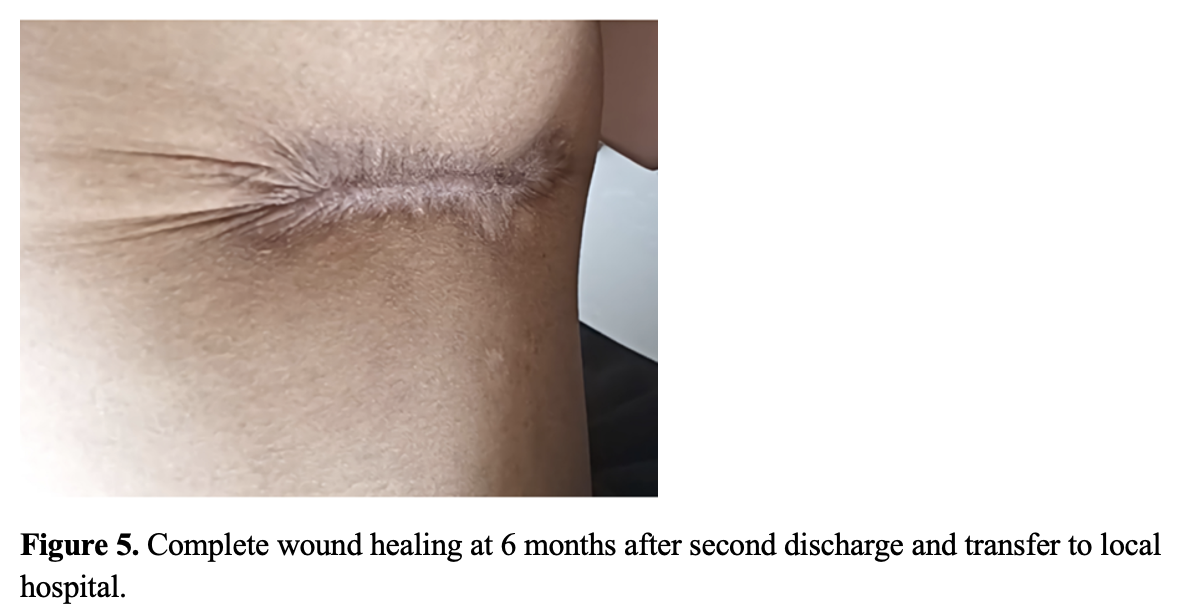
The patient was then transferred to the local hospital to complete the follow-up protocol, and the charge nurse made a handover to the local hospital and maintained weekly follow-ups. Six months later, the patient’s wound had completely healed (Figure 5).
Discussion
Cancerous wounds are a common clinical occurrence and are often difficult to heal due to disease progression, malnutrition, infection, and other factors.9 Symptoms such as high exudate, odor, and pain cause embarrassment, anxiety, fear of socialization, fear of discrimination, and reduced quality of life.9 In such cases, developing an effective approach to cancer wound care and management is critical to wound healing and symptom management. During the care of this patient, the authors conducted a comprehensive assessment and developed a detailed nursing plan, and through the cooperation of multiple specialist nurses and the implementation of transitional care, the care team was able to achieve a favorable physical and psychological state during the patient’s hospitalization and home stay, which promoted recovery and improved quality of life.
Multidisciplinary teamwork consists of health care professionals from different medical specialties collaborating to discuss a particular patient’s diagnosis and treatment, in which each health care professional can make an independent contribution.10 Specialized nurses in different roles played a key role in the treatment and care of this patient’s wound. For example, the psychiatric specialist nurse helped to relieve the patient’s psychological pain and enhance her self-control and self-management skills. Clinical dietitians developed an appropriate dietary plan and guided food choices to help the patient establish good eating habits to improve her nutritional status. Wound specialist nurses’ careful treatment of wounds promotes healing of the wound.11 At the end of the treatment, the patient’s physical condition and psychological status were improved. The patient did not experience significant nausea, vomiting, or loss of appetite during chemotherapy and did not experience adverse events such as pressure injuries, falls, or deep vein thrombosis. The patient’s weight gain was 1 kg, her psychological distress score decreased from 5 to 3, and the cancerous wound healed 6 months after discharge. These results suggest that comprehensive assessment and wound care measures and a collaborative model of nurse specialists in multiple areas of care are important and necessary for the treatment and rehabilitation of patients with large cancerous wounds.
Transitional care is a group of activities that ensure the coordination and continuity of health care services for patients as they move between sites or between levels of care in the same site.12 The presence of a cancerous wound resulted in a high level of medical and nursing care needs for this patient even after discharge from the hospital. After this patient was discharged from the hospital, the authors used WeChat and remote technology to provide transitional care. This ensured continuity of care, thereby improving the patient's ability to self-manage the disease, helping her transition smoothly from the hospital to the home, reducing the risk of complications and adverse outcomes, and decreasing the time and financial burdens related to her medical visits.
Several issues and challenges were also identified during the treatment of this patient. The patient’s psychological status was greatly affected during the treatment process and required active psychological intervention, and her nutritional status also required close attention and adjustment. The management of these issues required the joint efforts and collaboration of the nursing team to better ensure the treatment outcome and quality of life of the patient.
In summary, a comprehensive assessment, wound care measures, transitional care, and a collaborative model of specialized nurses from multiple nursing areas effectively improved the physical and psychological status of a patient with a large cancerous wound and reduced the occurrence of adverse events. Based on this successful example, the authors hope to better apply these experiences and methods in future nursing work to provide better nursing services to more patients in need.
Limitations
This case report only includes one patient’s experience and cannot be generalized to all patients with ALK-negative anaplastic large cell lymphoma and cancerous wounds. Additionally, the impact of the patient’s mental health and social support systems on wound healing was not fully addressed in this report. Future research should consider the role of mental health and social support systems in wound healing to develop more comprehensive nursing interventions for patients with cancerous wounds.
Conclusion
This article discusses a 59-year-old female who was admitted to the hospital with a large right inguinal mass with ulceration, diagnosed with ALK-negative mesenchymal large cell lymphoma after examination, and started on chemotherapy. The patient’s risk assessment, wound assessment, and management measures were described in detail. The patient’s wound was effectively controlled and treated, and complete healing was eventually achieved. This case emphasizes the importance of a thorough assessment and individualized care plan for patients, as well as the critical role of various specialty nurses and transitional care in wound management.
Acknowledgments
Authors: Mei Liu, MD, RN; Nina Cai, MD, RN; Meichen Du, MD, RN; and Juan Guo, MD, RN
Affiliation: Oncology Department of Tongji Hospital of Tongji Medical College of Huazhong University of Science and Technology
Correspondence: Juan Guo, MD, RN, Oncology Department of Tongji Hospital of Tongji Medical College of Huazhong University of Science and Technology, No.1095 Jiefang Avenue, Wuhan City, Hubei Province, China; 39153240@qq.com
Disclosure: The authors disclose no financial or other conflicts of interest.
Funding: None.
References
1. Pina-Oviedo S, Ortiz-Hidalgo C, Carballo-Zarate AA, Zarate-Osorno A. ALK-negative anaplastic large cell lymphoma: current concepts and molecular pathogenesis of a heterogeneous group of large T-cell lymphomas. Cancers. 2021;13(18):4667. doi:10.3390/cancers13184667
2. Furka A, Simkó C, Kostyál L, et al. Treatment algorithm for cancerous wounds: a systematic review. Cancers (Basel). 2022;14(5):1203. doi:10.3390/cancers14051203
3. Kao EY, Mukkamalla SKR, Lynch DT. ALK Negative anaplastic large cell lymphoma. In: StatPearls. StatPearls Publishing; 2024. Accessed July 25, 2024. http://www.ncbi.nlm.nih.gov/books/NBK519019/
4. Gromowsky MJ, D’Angelo CR, Lunning MA, Armitage JO. ALK-positive anaplastic large cell lymphoma in adults. Fac Rev. 2023;12:21. doi:10.12703/r/12-21
5. Zade B, Rao V, Patil T, Chharchhodawala T. A rare case of anaplastic large cell lymphoma of the knee joint. J Orthop Case Rep. 2023;13(8):37-41. doi:10.13107/jocr.2023.v13.i08.3806
6. Fernández-de-Misa R, Hernández-Machín B, Combalía A, et al. Prognostic factors in patients with primary cutaneous anaplastic large cell lymphoma: a multicentric, retrospective analysis of the Spanish Group of Cutaneous Lymphoma. J Eur Acad Dermatol Venereol. 2020;34(4):762-768. doi:10.1111/jdv.16006
7. Beers EH. Palliative wound care: less is more. Surg Clin North Am. 2019;99(5):899-919. doi:10.1016/j.suc.2019.06.008
8. Fallah N, Rasouli M, Amini MR. The current and advanced therapeutic modalities for wound healing management. J Diabetes Metab Disord. 2021;20(2):1883-1899. doi:10.1007/s40200-021-00868-2
9. Starace M, Carpanese MA, Pampaloni F, et al. Management of malignant cutaneous wounds in oncologic patients. Support Care Cancer. 2022;30(9):7615-7623. doi:10.1007/s00520-022-07194-0
10. Taberna M, Gil Moncayo F, Jané-Salas E, et al. The multidisciplinary team (MDT) approach and quality of care. Front Oncol. 2020;10:85. doi:10.3389/fonc.2020.00085
11. Kuhnke JL, Keast D, Rosenthal S, Evans RJ. Health professionals’ perspectives on delivering patient-focused wound management: a qualitative study. J Wound Care. 2019;28(Sup7):S4-S13. doi:10.12968/jowc.2019.28.Sup7.S4
12. Shahsavari H, Zarei M, Aliheydari Mamaghani J. Transitional care: concept analysis using Rodgers’ evolutionary approach. Int J Nurs Stud. 2019;99:103387. doi:10.1016/j.ijnurstu.2019.103387
