



Early Postoperative Complications of Elective Versus Emergency Stoma Creation: A Tertiary Academic Center Experience
Bin Traiki Thamer, MBBS1; Fayez Aldarsouni, MBBS2; Razan AlRabah, MBBS3; Hassan Aloraini, MBBS4; Esraa Altawil, SSCPN5; Doaa Alfraidy, MBBS6, 7; Sulaiman Alshammari, MBBS1; Noura Alhassan, MBBS1; and Khayal Alkhayal, MBBS1
© 2024 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Wound Management & Prevention or HMP Global, their employees, and affiliates.
Abstract
Background: Stoma creation is standard in general surgery, yet complication rates remain high.
Purpose: This study investigated the incidence and risk factors for early postoperative stoma complications in elective vs emergency surgery. Methods: All patients who underwent stoma creation between June 2015 and November 2020 were retrospectively reviewed and analyzed. Patients were divided into 2 groups based on the surgery type: elective vs emergency. Results: A total of 375 patients were included in this study. Two hundred fifty-three patients (67.5%) underwent elective stoma creation, while 122 (32.5%) underwent stoma creation during an emergency surgery. In the emergency group, white blood cell, blood urea nitrogen, and creatinine levels were statistically significantly higher (P = .001, .001, and .002, respectively). Albumin levels were statistically significantly lower in the emergency group (P = .001). The mean Emergency Surgery Score was 5.17 ± 2.73 in the emergency group compared to 4.4 ± 2.44 in the elective group (P = .006). Colorectal cancer was the most common cause of stoma creation in both groups. In terms of stoma creation, colostomy was statistically significantly more common in the emergency group (59%, P = .001), compared to ileostomy in the elective group (58.9%, P = .001). Complications were observed in 135 of all patients (36%). Necrosis was statistically significantly more common in emergency cases (9.9%, P < .001). Conclusion: Surgeons should strive to optimize the patient’s condition prior to the operation and, if possible, perform stoma marking or involve a stoma nurse in the operating room to select the most suitable site. In high-risk patients, where complications are more likely, the use of a stoma should be minimized and definitive management should always be pursued if feasible.
Introduction
Stoma creation is pivotal in gastrointestinal surgery, serving as a temporary or permanent solution to redirect bowel content.1,2 Temporary stomas are created during emergent conditions such as trauma, bowel perforation, or as a protective measure for optimal anastomosis healing.3 On the other hand, permanent stomas are made when the anorectum is resected or when the anastomosis is impossible.3
According to the United Ostomy Association, approximately 500 000 individuals in the United States live with a stoma, with around 100 000 patients undergoing stoma-creation procedures annually4 and with colorectal cancer management accounting for over 75% of stoma creations.5 In Saudi Arabia, colorectal cancer is the most prevalent cancer among men and the third most common among women.6 Despite being a routine procedure, the complication rate for stoma creation can be as high as 70%.5 The most common early complications (ie, less than 1 month postoperative) include inappropriate stoma site, vascular compromise, retraction, skin irritation, peristomal infection, abscess, and fistula. In contrast, stoma prolapse is the most common late complication.5,7
Despite the significant burden of stoma-related complications, few studies have comprehensively addressed this issue.3,7-9 As a result, identifying preoperative predictors of postoperative complications is of utmost importance. This study aimed to investigate the incidence and risk factors for early postoperative complications in patients who underwent stoma creation during elective vs emergency surgery.
Methods
After the approval of the Ethical Institutional Review Board at King Saud University, the authors retrospectively reviewed the medical records of all patients who underwent stoma creation at King Saud University Medical City, an academic medical institution and a tertiary hospital in Riyadh, Saudi Arabia. An Excel (Microsoft) data sheet was generated by the research team to encompass all variables examined in the study. Data collection was carried out by the research team and supervised by the principal investigator. The need for written informed consent was waived by the Ethical Institutional Review Board at King Saud University, College of Medicine, due to the retrospective nature of the study.
Patients who underwent stoma creation between June 2015 and November 2020 were included in this study, though pediatric patients under the age of 16 were excluded. Patients were divided into 2 groups based on surgery type: those with elective surgery and those with emergency surgery. An elective surgery was defined as any stoma created during an elective scheduled procedure. The emergency group included any patient who presented with a surgical emergency and underwent stoma creation. Reported complications included early postoperative complications within the index of admission. The severity of the postoperative complications was graded by the principal investigator following the original definitions of the Clavien-Dindo classification.10
A dedicated stoma care team provided preoperative stoma marking and education. All patients were required to complete a full stoma education by the stoma care team before discharge and outpatient follow-up visits to the stoma clinic.
Statistical analysis
Data were analyzed using the Statistical Package for Social Studies (SPSS 26; IBM Corporation). Continuous variables were expressed as mean ± standard deviation and categorical variables as percentages. The t-test was used for continuous variables with normal distribution. The chi-square test and Fisher's exact test were used for categorical variables. Factors significant in the univariate analysis were investigated for postoperative complications using univariate and multivariate logistic regression models. A P value of < .05 was considered statistically significant.
Results
A total of 375 patients were included in this study. Two hundred fifty-three patients (67.5%) underwent stoma creation in elective surgery, while 122 patients (32.5%) underwent stoma creation during emergency procedures. The baseline demographics and clinical characteristics are presented in Table 1. In the emergency group, white blood cell count (WBC), blood urea nitrogen (BUN), and creatinine levels were significantly higher compared to the elective group (P = .001, .001, and .002, respectively). Albumin was significantly lower in the emergency group than in the elective group (P = .001). The American Society of Anesthesiology score was statistically significant for classes II and IV. Class II was higher in the elective group (P = .001), while class IV was higher in the emergency group (P = .001). The Emergency Surgery Score (ESS) mean was 5.17 ± 2.73 in the emergency group, compared to 4.4 ± 2.44 in the elective group (P = .006). Colorectal cancer was the most common cause of stoma creation in both groups (72.7% in elective vs 52.5% in emergency), followed by inflammatory bowel disease in the elective group (14.6%) and bowel perforation/leak in the emergency group (18.9%).
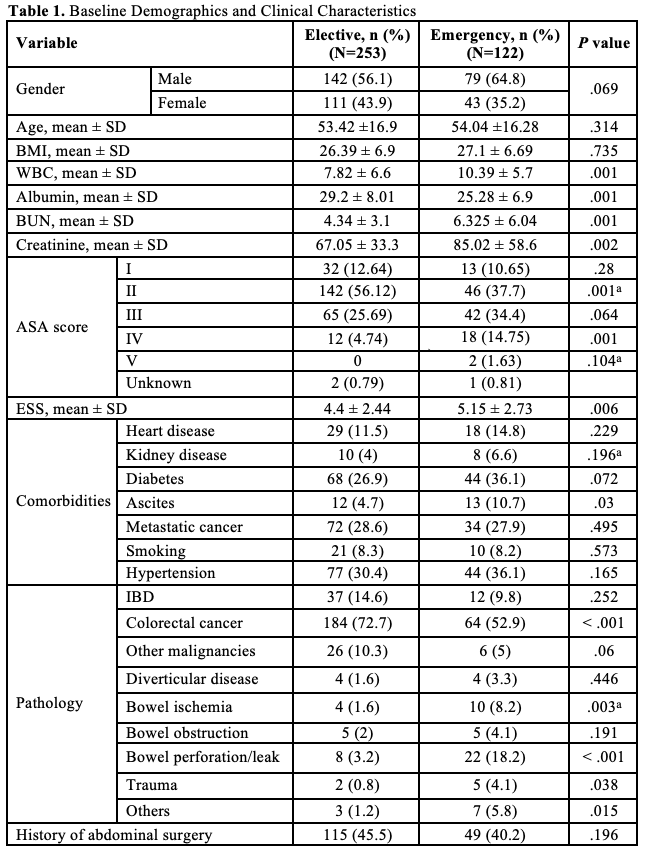

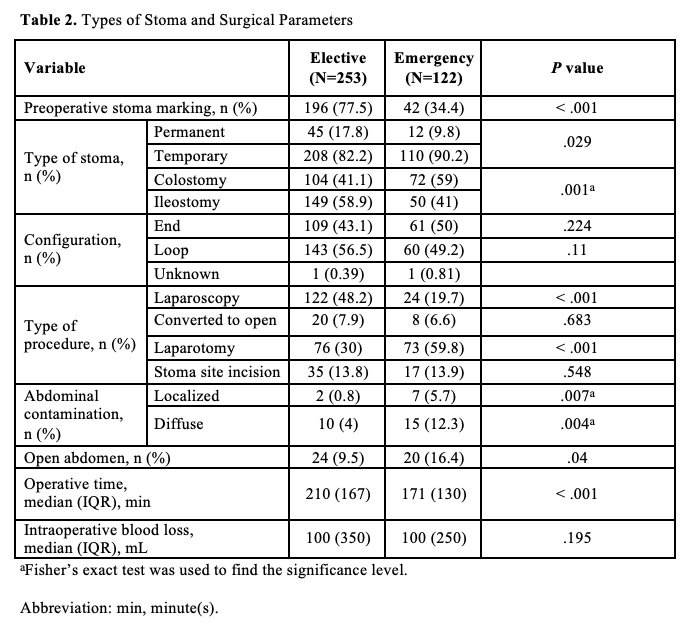
The types of stoma and surgical parameters are presented in Table 2. Preoperative stoma marking was statistically significantly higher in the elective group compared to the emergency group (77.5% vs 34.3%, P < .001). In terms of stoma creation, colostomy was significantly more common in the emergency group (59% vs. 41.1%, P = .001). In comparison, ileostomy creation was significantly more common in the elective group (58.9% vs. 41%, P = .001). Procedures were performed laparoscopically in 48.2% (122 patients) of the elective group, compared to 19.7% (24 patients) of the emergency group (P < .001). A laparotomy approach was more common in the emergency group (59.8%) compared to the elective group (30%) (P < .001). The emergency group had a higher incidence of localized and diffuse abdominal contamination (5.7% and 12.3%, respectively) compared to the elective group (0.8% and 4%, respectively) (P = .007 and .004, respectively). Operative time was significantly longer in the elective group compared to the emergency group (P < .001).
Postoperative complications are presented in Table 3. Complications were observed in 135 patients (36%), with no significant difference in complication rate between the 2 groups. One patient died during surgery, and postoperative complications were unable to be assessed. The most common complication in both groups was electrolyte imbalance, followed by abdominal collection and wound infection. Necrosis was statistically significantly more common in emergency cases (9.9% vs 2%, P = .001). The Clavien-Dindo classification system was used to grade complications, as illustrated in the Figure. The majority of complications were grade I in both groups.
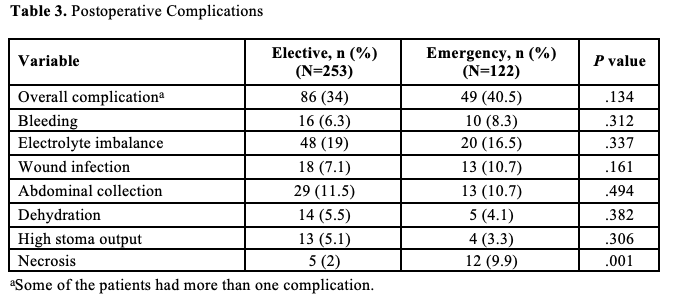
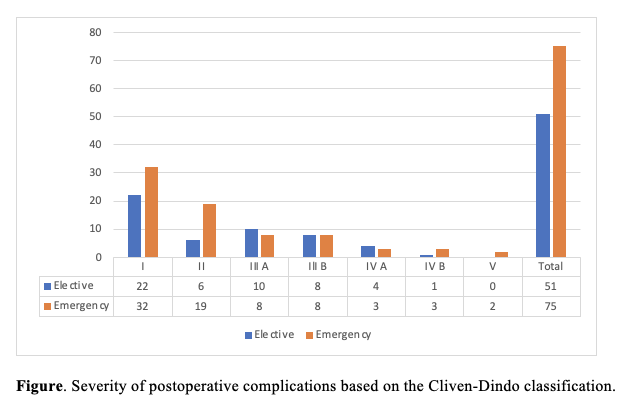
Table 4 examines the association between postoperative complications and the patients’ clinical characteristics. Mean BUN levels and ESS were significantly higher in complicated cases than in non-complicated cases (P = .005 and .001, respectively). Ascites and a history of abdominal surgery were more common in the complicated group (P = .027 and .003, respectively). In terms of stoma configuration, 69 patients (51.1%) (P = .068) with end configuration had complications, while 65 patients (48.1%) (P = .061) with loop configuration had complications. Complications were seen more in patients who underwent laparotomy (53.3%) vs those who underwent laparoscopy (30.4%) (P < .001 and .007, respectively). Stoma site incisions were seen significantly more frequently in the non-complicated group (17.5%) (P = .004). In contrast, the abdomen being left open for a second examination was significantly more frequent in the complicated group (17.8%) (P = .004). Median blood loss was significantly higher in the complicated group at 200 mL (IQR 438) (P < .001). Additionally, the median duration of operation was significantly more extended in the complicated group (237 minutes, IQR 159) (P < .001).
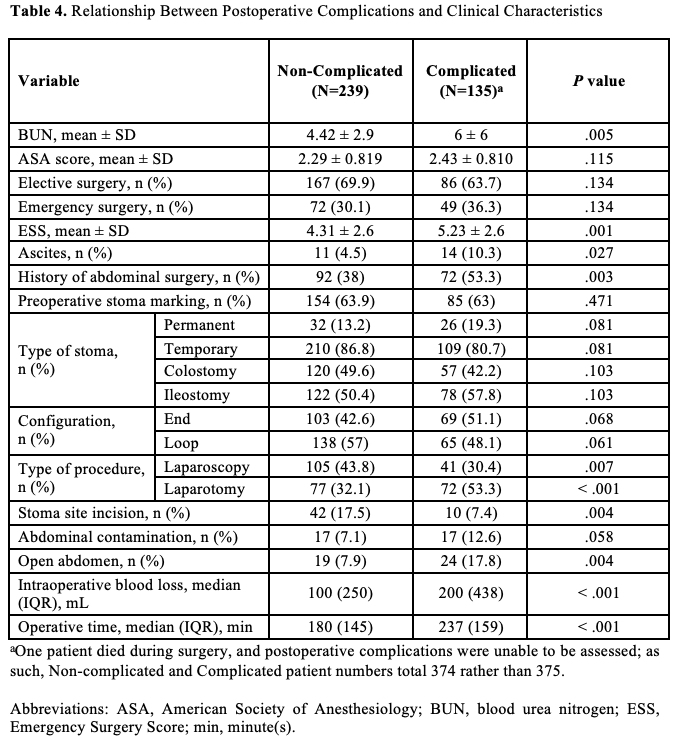
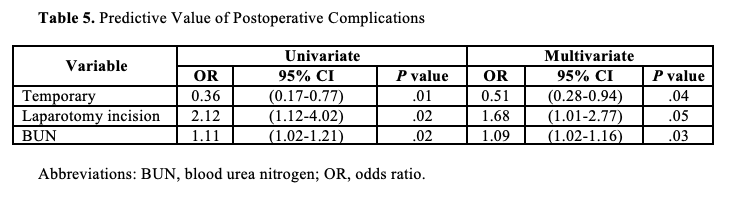
Table 5 presents the predictive values of postoperative complications. In univariate and multivariate analysis, temporary stoma creation, laparotomy incision, and elevated BUN levels significantly predicted postoperative complications in patients undergoing stoma creation.
Discussion
The goal of stoma creation is to improve patients’ quality of life and minimize surgical complications.3,11,12 However, inappropriate preoperative management and postoperative complications can result in diminished quality of life, social isolation, and increased medical interventions and costs.11 Postoperative complications following stoma creation are reported in high prevalence.3,7,8 To the best of the knowledge of the authors of the current study, this is the largest retrospective analysis evaluating postoperative stoma complications in Saudi Arabia.
Elective stoma surgery has overall fewer complications than emergency surgery.11 In one study, emergency stomas showed higher complication rates than elective Clavier-Dindo’s grade III (6% vs 20%, respectively) and IV (1% vs 8%, respectively).13 This might be attributed to insufficient preoperative planning and comorbidities optimization. Preoperative stoma marking helps surgeons select the optimal location for the sake of the patient’s well-being and reduced postoperative complications.14 In the current study, preoperative stoma marking was significantly higher in the elective group (77.5% vs 34.3%, P < .001), reflecting insufficient preparation in an emergency. One study compared open stoma creation with laparoscopic stoma creation and found comparable results regarding operation time and time of oral intake.15 However, laparoscopic stoma creation was associated with less blood loss.15 In the current study, as more dissection and reconstruction occur in the elective sitting, the stoma is concurrently created as a part of another major surgery, which explains the higher mean of blood loss and longer operative time among elective patients.
Studies reported an overall rate of stoma-related complications ranging from 10% to 70%, depending on the number of complications scored.3,7,8 The current study's postoperative complication rate was 36.3%, with no significant difference between the 2 groups (P = .208). Stoma necrosis was significantly higher in the emergency group (10.7% vs 2%, P < .001). The literature shows that the necrosis rate ranges between 1.6% and 11%.16-18 Necrosis is associated with poor surgical techniques, including excessive tension and dissection of the mesentery and ligation of primary blood vessels.3,19 Colostomy-type stoma was linked to a higher rate of necrosis.20 In the current study, the colostomy-type stoma was created significantly more frequently in the emergency group (59% vs 41.1%, P = .001), which might have contributed to the higher necrosis rate. Moreover, electrolyte imbalance was the highest complication in both groups, which might be attributed to the ileostomy-type stoma (57.7% in elective vs 41% emergency, P = .003). Patients with an ileostomy experience a state of relative hypovolemia due to the high liquid content of ileostomy effluent, which can lead to dehydration and electrolyte imbalances if not correctly managed.3
The ESS is a validated scoring system to predict mortality in emergency surgery patients.21 The ESS mean score in the current study was significantly higher in the emergency group (P = .006). Reported risk factors for stoma complications include female gender, high body mass index, diabetes, emergency surgery, colostomy-stoma type, short stoma length, lack of preoperative marking, and inappropriate location.20,22-25 In the current study, the risk factors for postoperative complications included temporary stoma creation, laparotomy incision, and elevated BUN levels. Of note, the authors’ institution is a tertiary care and referral center, and most patients have advanced disease and comorbidities, which might be attributed to the recorded risk factors.
Limitations
The current study has limitations that must be considered when interpreting the results. This study has a retrospective nature, subjecting it to potential recall bias. The data collected from medical records were documented by hospital staff who may not have been directly involved in the study, which could have influenced the observed associations. Moreover, the research was conducted in a single center, which may curtail the generalizability of the findings to other contexts. To overcome these limitations, future research should implement a multicentric approach to enhance the validity of the findings and expedite their generalizability to broader populations.
Conclusion
Surgeons should strive to optimize the patient’s condition prior to the operation and, if possible, perform stoma marking or involve a stoma nurse in the operating room to select the most suitable site. In high-risk patients, where complications are more likely, the use of a stoma should be minimized and definitive management should always be pursued if feasible. The skills and experience of the surgeon, as well as consultation with colorectal surgeons, can help minimize complications. Additionally, temporary stoma creation, laparotomy incision, and elevated BUN levels are significant factors that predict postoperative complications in patients undergoing stoma creation.
Acknowledgments
Authors: Bin Traiki Thamer, MBBS1; Fayez Aldarsouni, MBBS2; Razan AlRabah, MBBS3; Hassan Aloraini, MBBS4; Esraa Altawil, SSCPN5; Doaa Alfraidy, MBBS6, 7; Sulaiman Alshammari, MBBS1; Noura Alhassan, MBBS1; and Khayal Alkhayal, MBBS1
Affiliations: 1Colorectal Research Chair, Department of Surgery, College of Medicine, King Saud University, Riyadh, Saudi Arabia; 2Department of Trauma Surgery, King Saud Medical City, Riyadh, Saudi Arabia; 3College of Medicine, King Saud University, Riyadh, Saudi Arabia; 4Department of Emergency Medicine, King Saud University Medical City, Riyadh, Saudi Arabia; 5Pharmacy Department, Clinical Pharmacy Services, King Saud University Medical City, Riyadh, Saudi Arabia; 6Trauma and Acute Care Surgery Unit, Department of Surgery, King Saud University Medical City, King Saud University, Riyadh, Saudi Arabia; 7Department of Critical Care King Saud University Medical City, King Saud University, Riyadh, Saudi Arabia
Disclosure: The authors have no financial or other conflicts of interest to disclose.
Correspondence: Razan AlRabah, MBBS, College of Medicine, King Saud University, 12372 P.O Box 7065, Riyadh, Saudi Arabia; razanalrabah@gmail.com
References
1. Aboulian A. Ostomy complications in Crohn's disease. Clin Colon Rectal Surg. 2019;32(4):314-322. doi:10.1055/s-0039-1683924
2. Kugler CM, Breuing J, Rombey T, et al. The effect of preoperative stoma site marking on risk of stoma-related complications in patients with intestinal ostomy-protocol of a systematic review and meta-analysis. Syst Rev. 2021;10(1):146. doi:10.1186/s13643-021-01684-8
3. Shabbir J, Britton DC. Stoma complications: a literature overview. Colorectal Dis. 2010;12(10):958-964. doi:10.1111/j.1463-1318.2009.02006.x
4. Sheetz KH, Waits SA, Krell RW, et al. Complication rates of ostomy surgery are high and vary significantly between hospitals. Dis Colon Rectum. 2014;57(5):632-637. doi:10.1097/DCR.0000000000000038
5. Ambe PC, Kurz NR, Nitschke C, Odeh SF, Möslein G, Zirngibl H. Intestinal ostomy. Dtsch Arztebl Int. 2018;115(11):182-187. doi:10.3238/arztebl.2018.0182
6. Alsanea N, Abduljabbar AS, Alhomoud S, Ashari LH, Hibbert D, Bazarbashi S. Colorectal cancer in Saudi Arabia: incidence, survival, demographics and implications for national policies. Ann Saudi Med. 2015;35(3):196-202. doi:10.5144/0256-4947.2015.196
7. Murken DR, Bleier JIS. Ostomy-related complications. Clin Colon Rectal Surg. 2019;32(3):176-182. doi:10.1055/s-0038-1676995
8. Nastro P, Knowles CH, McGrath A, Heyman B, Porrett TR, Lunniss PJ. Complications of intestinal stomas. Br J Surg. 2010;97(12):1885-1889. doi:10.1002/bjs.7259
9. MacDonald S, Wong LS, Ng HJ, et al. Postoperative outcomes and identification of risk factors for complications after emergency intestinal stoma surgery - a multicentre retrospective study. Colorectal Dis. 2024;26(5):994-1003. doi:10.1111/codi.16947
10. Clavien PA, Barkun J, de Oliveira ML, et al. The Clavien-Dindo classification of surgical complications: five-year experience. Ann Surg. 2009;250(2):187-196. doi:10.1097/SLA.0b013e3181b13ca2
11. Tsujinaka S, Tan KY, Miyakura Y, et al. Current management of intestinal stomas and their complications. J Anus Rectum Colon. 2020;4(1):25-33. doi:10.23922/jarc.2019-032
12. Parini D, Bondurri A, Ferrara F, et al; Multidisciplinary Italian Study group for STOmas (MISSTO). Surgical management of ostomy complications: a MISSTO-WSES mapping review. World J Emerg Surg. 2023;18(1):48. doi:10.1186/s13017-023-00516-5
13. Qureshi A, Cunningham J, Hemandas A. Emergency stomas; should non-colorectal surgeons be doing it? Gastroenterol Hepatol Bed Bench. 2018;11(4):306-312.
14. Wound, Ostomy and Continence Nurses Society; Guideline Development Task Force. WOCN society clinical guideline: management of the adult patient with a fecal or urinary ostomy-an executive summary. J Wound Ostomy Continence Nurs. 2018;45(1):50-58. doi:10.1097/WON.0000000000000396
15. Hayashi K, Kotake M, Hada M, et al. Laparoscopic versus open stoma creation: a retrospective analysis. J Anus Rectum Colon. 2017;1(3):84-88. doi:10.23922/jarc.2016-014
16. Franklyn J, Varghese G, Mittal R, Rebekah G, Jesudason MR, Perakath B. A prospective randomized controlled trial comparing early postoperative complications in patients undergoing loop colostomy with and without a stoma rod. Colorectal Dis. 2017;19(7):675-680. doi:10.1111/codi.13600
17. Whiteley I, Russell M, Nassar N, Gladman MA. Outcomes of support rod usage in loop stoma formation. Int J Colorectal Dis. 2016;31(6):1189-1195. doi:10.1007/s00384-016-2569-7
18. Cross AJ, Buchwald PL, Frizelle FA, Eglinton TW. Meta-analysis of prophylactic mesh to prevent parastomal hernia. Br J Surg. 2017;104(3):179-186. doi:10.1002/bjs.10402
19. Krishnamurty DM, Blatnik J, Mutch M. Stoma complications. Clin Colon Rectal Surg. 2017;30(3):193-200. doi:10.1055/s-0037-1598160
20. Formijne Jonkers HA, Draaisma WA, Roskott AM, van Overbeeke AJ, Broeders IA, Consten EC. Early complications after stoma formation: a prospective cohort study in 100 patients with 1-year follow-up. Int J Colorectal Dis. 2012;27(8):1095-1099. doi:10.1007/s00384-012-1413-y
21. Nandan AR, Bohnen JD, Sangji NF, et al. The Emergency Surgery Score (ESS) accurately predicts the occurrence of postoperative complications in emergency surgery patients. J Trauma Acute Care Surg. 2017;83(1):84-89. doi:10.1097/TA.0000000000001500
22. Arumugam PJ, Bevan L, Macdonald L, et al. A prospective audit of stomas--analysis of risk factors and complications and their management. Colorectal Dis. 2003;5(1):49-52. doi:10.1046/j.1463-1318.2003.00403.x
23. Persson E, Berndtsson I, Carlsson E, Hallén AM, Lindholm E. Stoma-related complications and stoma size - a 2-year follow up. Colorectal Dis. 2010;12(10):971-976. doi:10.1111/j.1463-1318.2009.01941.x
24. Parmar KL, Zammit M, Smith A, Kenyon D, Lees NP; Greater Manchester and Cheshire Colorectal Cancer Network. A prospective audit of early stoma complications in colorectal cancer treatment throughout the Greater Manchester and Cheshire colorectal cancer network. Colorectal Dis. 2011;13(8):935-938. doi:10.1111/j.1463-1318.2010.02325.x
25. Cottam J, Richards K, Hasted A, Blackman A. Results of a nationwide prospective audit of stoma complications within 3 weeks of surgery. Colorectal Dis. 2007;9(9):834-838. doi:10.1111/j.1463-1318.2007.01213.x
